
Abstract
Abstract
Background:
Ventilator-associated pneumonia (VAP) is common in critically injured patients. The pathogenesis of VAP is not completely understood. We hypothesized that mechanically ventilated trauma patients who develop pneumonia have a progressive increase in pathogen burden over the course of ventilation until a threshold for symptomatic pneumonia is reached, leading to clinical suspicion of VAP.
Methods:
Critically injured adults ventilated for more than two successive days were enrolled. Patients underwent daily surveillance mini-bronchoscopic alveolar lavage (mBAL) while ventilated for 14 days or until extubation. Standard semi-quantitative cultures were performed, and the investigators were blinded to the results. Standard patient management was performed by the clinical team. Patients suspected of having VAP by the clinical team underwent bronchoscopic bronchoalveolar lavage (bBAL) and semi-quantitative culture, with VAP defined as clinical symptoms plus >104 colony-forming units (CFU) of bacteria. Standard statistical analysis for non-parametric data was performed.
Results:
The 37 patients enrolled were ventilated for a median of nine days. While ventilated, 23 patients met the criteria for a clinical suspicion of VAP, of which two were too ill for bronchoscopy. Thus, 21 patients underwent bBALs because of a suspicion of VAP, and 13 (35%) were positive, with >104 CFU of one or more pathogens, and were treated for pneumonia. The bacterial burden on mBAL remained <104 CFU during ventilation for 32% of patients. None developed clinical symptoms of VAP. Two-thirds (67%) had an mBAL bacterial burden of >104 CFU without clinical suspicion of VAP. Half (56%) of positive surveillance cultures were followed by clinical VAP, confirmed by bBAL, all of which had identical pathogens on mBAL and bBAL. Almost half (44%) of the patients with positive surveillance mBALs never developed clinical VAP.
Conclusion:
A significant percentage of critically injured, ventilated adults develop high bacterial burdens in the lungs early in their course, and many clear these bacteria without developing VAP. Further study is needed to identify the factors causing progression to VAP.
T
Although timely and adequate antibiotic therapy significantly improves outcomes in patients with VAP, the clinical signs and symptoms suggesting pneumonia are non-specific and result from non-pneumonic causes in 40%–60% of instances [11-15]. An accurate and specific diagnosis of VAP requires the use of invasive specimen collection techniques such as bronchoscopy-directed bronchoalveolar lavage (bBAL) with quantitative bacterial culture and sensitivity assessment [16]. At our institution, invasive culture techniques, such as bBAL, are undertaken only when there has been clinical deterioration and pneumonia is suspected. Culture results frequently are not available for three days after bBAL is performed. The non-specific nature of the clinical signs and symptoms of VAP, coupled with the significant delay in finalized culture data, creates the need to cover those patients suspected of pneumonia empirically with broad-spectrum antibiotics until the specific pathogen can be identified or VAP ruled out. Thus, for those who actually have VAP, antibiotics are initiated only after the infection process has established itself well enough to produce signs and symptoms. In the remaining patients, unneeded empiric antibiotics are continued for several days. This current management strategy not only delays appropriate therapy but also contributes to significant antibiotic exposure that eventually proves unnecessary, increasing the risk of antibiotic-resistant infections and the associated costs.
As part of a larger research initiative to improve the timing and accuracy of the diagnosis of VAP in critically ill and injured patients, we have sought to understand better the relation of pathogen burden to the establishment of infection and the development of symptoms of VAP. To examine the relation of bacterial burden to the subsequent development of VAP, we assayed patients with quantitative cultures daily and determined their relation to the development of clinical signs of VAP. We hypothesized that critically injured, mechanically ventilated patients who develop VAP demonstrate a progressive increase in the alveolar pathogen burden over the course of ventilation until a threshold for symptomatic pneumonia is reached, and VAP is suspected clinically.
Patients and Methods
This study is part of a Vanderbilt University Medical Center Institutional Review Board-approved, National Institutes of Health-funded (NIH-RO1 GM115353) prospective study. Critically injured, mechanically ventilated patients in the Trauma Intensive Care Unit (TICU) who met the inclusion and exclusion criteria and for whom surrogate consent was available were enrolled.
Inclusion/exclusion criteria
The inclusion criteria were age 18 years or older and on mechanical ventilation for at least two successive days without planned extubation within 24 hours of enrollment. The exclusion criteria were expected survival <24 hours, known prisoners, pneumonia diagnosis at the time of TICU admission, and the presence of conditions that would limit the subject's ability to tolerate collection of mini-bronchoalveolar lavage (mBAL). Such conditions included FiO2
Patient management and data abstraction
All patients were handled by the clinical management team according to the standards established by the TICU (Supplement 1). By TICU protocol, patients who developed signs and symptoms of possible VAP underwent bBAL and semi-quantitative culture (separate from the blinded mBAL) for the diagnosis of pneumonia by the TICU team and initiation of empiric antibiotics. The clinical suspicion of VAP is defined as the presence of three of five clinical signs, namely: (1) New, persistent, or progressive infiltrate on chest radiography; (2) purulent or copious tracheobronchial secretions; (3) a decline in pulmonary oxygenation status; (4) fever (38.5°C); or (5) leukocytosis (white blood cell count (WBC) >12,000/mcL). Institutionally approved methods were utilized for performance of bBAL (Supplement 2). A positive bBAL was defined as
All patients had clinical data abstracted from the medical records and entered in a REDCap data collection tool [17]. Abstracted data include demographic and injury severity data, including Injury Severity Score (ISS) and the daily Modified Sequential Organ Failure Assessment Score (mSOFA), clinical criteria for a clinical suspicion of pneumonia, the components of the Clinical Pulmonary Infection (CPIS) score [18], performance of bBAL and test results, and antibiotic use. The sepsis-related organ failure assessment score (SOFA) was used to quantify injury severity. Because of the infrequency of bilirubin assays, a modified score that eliminates this value was used with the remaining five parameters [19,20].
Performance of mini-BAL
Data were collected daily on study patients for 14 days or until they were extubated. On each study day, enrolled patients underwent blind mini-bronchoalveolar lavage sampling to obtain fluid for semi-quantitative microbiologic culture. The results of these cultures were not available for clinical use. Trained, dedicated research personnel performed all mBAL procedures. Sterile, protected-tip mBAL collection catheters (Kimberly-Clark Health Care, Roswell, GA) were used for the collection of the daily mBAL specimens as directed by the manufacturer. Catheters were inserted via a sterile access port at the connection of the ventilator circuit with the endotracheal tube and advanced until the polyethylene glycol (PEG) plug in the external catheter tip. After wedging of the external catheter, the sterile internal portion was extended. First, 20 mL of sterile, non-bacteriostatic saline was instilled, and then the syringe was aspirated to collect a minimum of 3 mL for culture. If inadequate fluid was returned, one or two additional 20-mL aliquots were used (60 mL total).
Performance of microbiologic cultures
All microbiologic cultures of both clinical (bBAL) and research (mBAL) specimens were performed in the Vanderbilt University Medical Center Clinical Microbiology Laboratory. Cultures were obtained according to the Clinical Laboratory Improvement Amendment (CLIA) standards for aerobic and anaerobic bacteria. Viral and fungal cultures were not performed for this study.
Statistical analysis
The frequency of the presence or absence of various clinical features used to establish VAP were compared by the Fisher exact test.
Results
There were 37 patients enrolled over an eight-month period from March 1, 2016 to November 1, 2016 from among a total of 403 screened patients admitted to the TICU (Fig. 1). The patient characteristics are shown in Table 1. The median age was 48 years, with the majority being white males between the ages of 36 and 59 years. Most of the patients (92%) were victims of blunt trauma (motor vehicle or motorcycle accident, fall, auto vs. pedestrian accident), whereas 8% sustained penetrating trauma. The mean Injury Severity Score (ISS) for the population was 31, and the median mSOFA score at enrollment was 8 (range 5–14).

Results of the enrollment and screening process.
Clinical suspicion of pneumonia
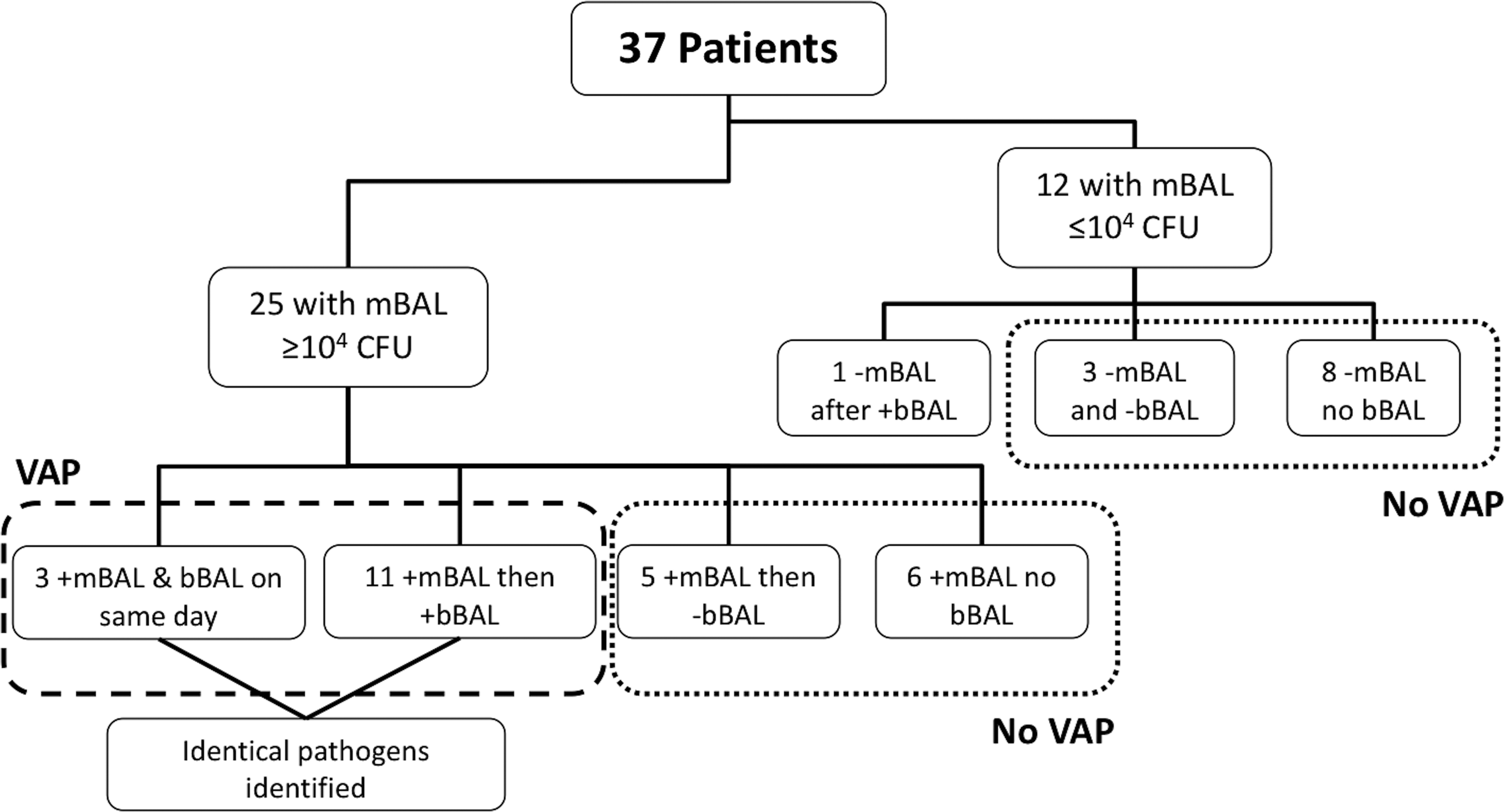
Figure 2 demonstrates the outcomes for those patients with and without clinical suspicion of VAP. Of the 37 patients, 23 (62%) were suspected on clinical grounds of having pneumonia, and 21 patients underwent a total of 30 bBALs and semi-quantitative cultures. Two of the 23 patients were too unstable to tolerate bBAL. These two patients were started on empiric antibiotics without quantitative cultures and were considered positive for VAP. Among patients who received more than one bBAL in the 14-day period, culture data from the first bBAL was used for analysis. Of the 21 patients undergoing bBAL, 13 had ≥104 CFU of bacteria, confirming VAP (62% of bBALs). Eight patients had <104 CFU, and antibiotics were discontinued. Table 2 shows the distribution of pathogens isolated from patients with VAP by quantitative bBAL. Staphylococcus aureus and Haemophilus influenzae were the two most common isolates (both present in 38% of patients).

Ventilator-associated pneumonia outcomes.
Total greater than number of patients because of multiple pathogens in some patients.
BAL = bronchoscopic bronchoalveolar lavage; CFU = colony-forming units.
The clinical findings for the patients are shown in Table 3. Most patients develop the individual clinical components of VAP at some point during their mechanical ventilation. However, the frequency of these symptoms was not different in those patients who did (positive bBAL) and did not (negative bBAL) have confirmed VAP.
bBAL = bronchoscopic bronchoalveolar lavage; CFU = colony-forming units; CPIS = Clinical Pulmonary Infection Score; P:F = PaO2/FiO2; VAP = ventilator-associated pneumonia.
Pneumonia severity by CPIS score
The median CPIS score of all 37 patients was 3 (Table 3). For those patients who underwent bBAL for a clinical suspicion of VAP (n = 21), the median CPIS was 4. This was also true for the patients who were found to have VAP (n = 13). However, in the patient population that was suspected of VAP, but had <104 CFUs (n = 8), the median CPIS score was 3.5.
Clinical outcomes
The median number of days on the ventilator was 9. There was an almost equal split between patients who required tracheostomy and those who did not (49% vs. 51%). Our mortality rate was 32%.
Quantitative bacterial surveillance
To determine the course of the bacterial burden in these critically ill patients, daily bacterial surveillance with mBALs and quantitative culture was performed from study enrollment (48 hours) until extubation. The results are shown in Fig. 3. In 12 of the 37 patients, the quantitative bacterial results remained <104 CFU throughout the period of mechanical ventilation. Eleven of these 12 patients were extubated (n = 9) or died (n = 2) without developing clinical suspicion of VAP. One patient had signs on VAP on the day of enrollment and had the first mBAL after initiation of antibiotics.
Surveillance culture outcomes.
Also in Figure 3, it can be seen that 25 patients had quantitative surveillance cultures that demonstrated at least one bacterial species with a count of
In 11 of the 25 patients with bacterial counts
We examined whether any clinical differences could be detected between those patients with mBAL of
bBAL = bronchoscopic bronchoalveolar lavage; CFU = colony-forming units; CPIS = Clinical Pulmonary Infection Score; mBAL = mini-bronchoscopic bronchoalveolar lavage; mBAL = mini-bronchoscopic alveolar lavage; mSOFA = Modified Sequential Organ Failure Assessment Score; P:F = PaO2/FiO2; VAP = ventilator-associated pneumonia.
Pathogens isolated in mBALs are shown in Table 5. The distribution is similar to that of those with pneumonia except that more pathogens were isolated.
Does not add up to total number of positive mBALs as 12 patients had more than two pathogens.
CFU = colony-forming units; mBAL = mBAL = mini-bronchoscopic bronchoalveolar lavage.
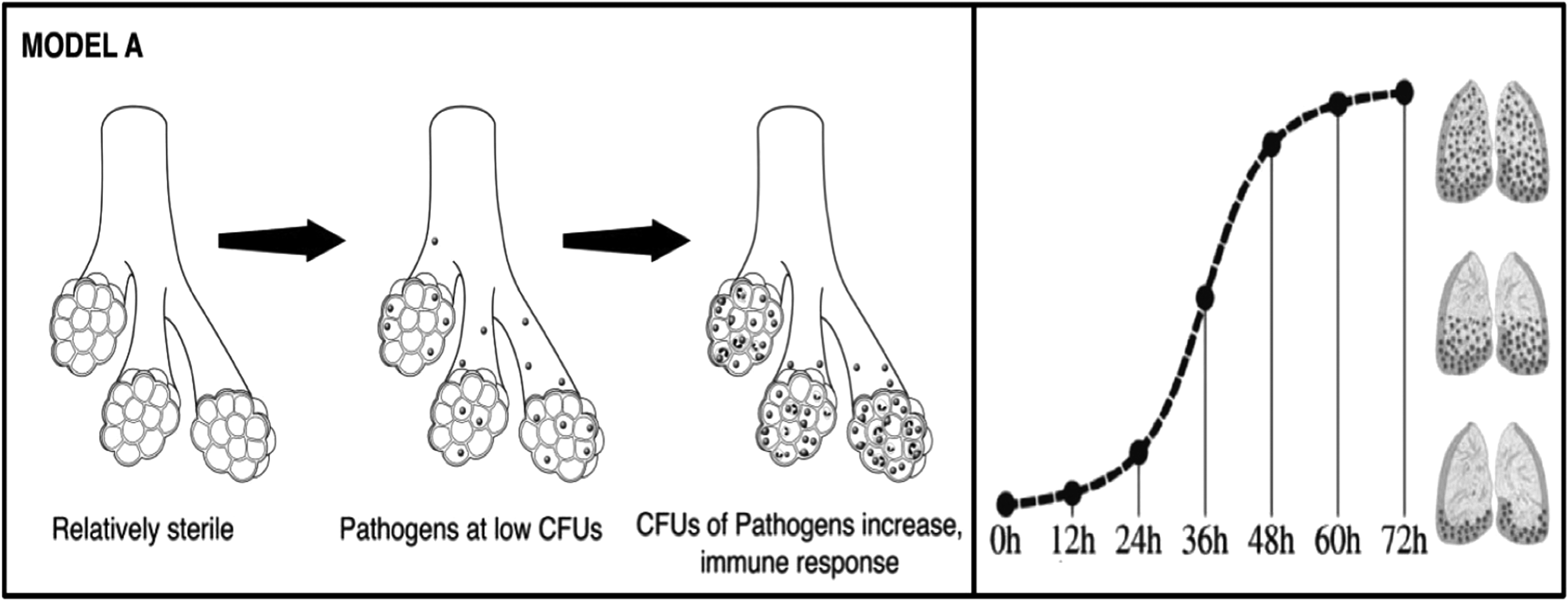
Discussion
Traditionally, VAP is thought to develop from bacterial contamination of the alveolar space, which, in the right environment, leads to bacterial growth. Signs of pneumonia are absent at low CFUs, but after bacterial proliferation to a critical mass, clinically evident pneumonia develops when the immune response is overwhelmed (Fig. 4). This critical mass typically is considered to be ≥104 CFU [21, 22]. Interestingly, our study demonstrates that critically injured trauma patients develop significant bacterial burdens (
Traditional hypotheses for pneumonia pathogenesis.
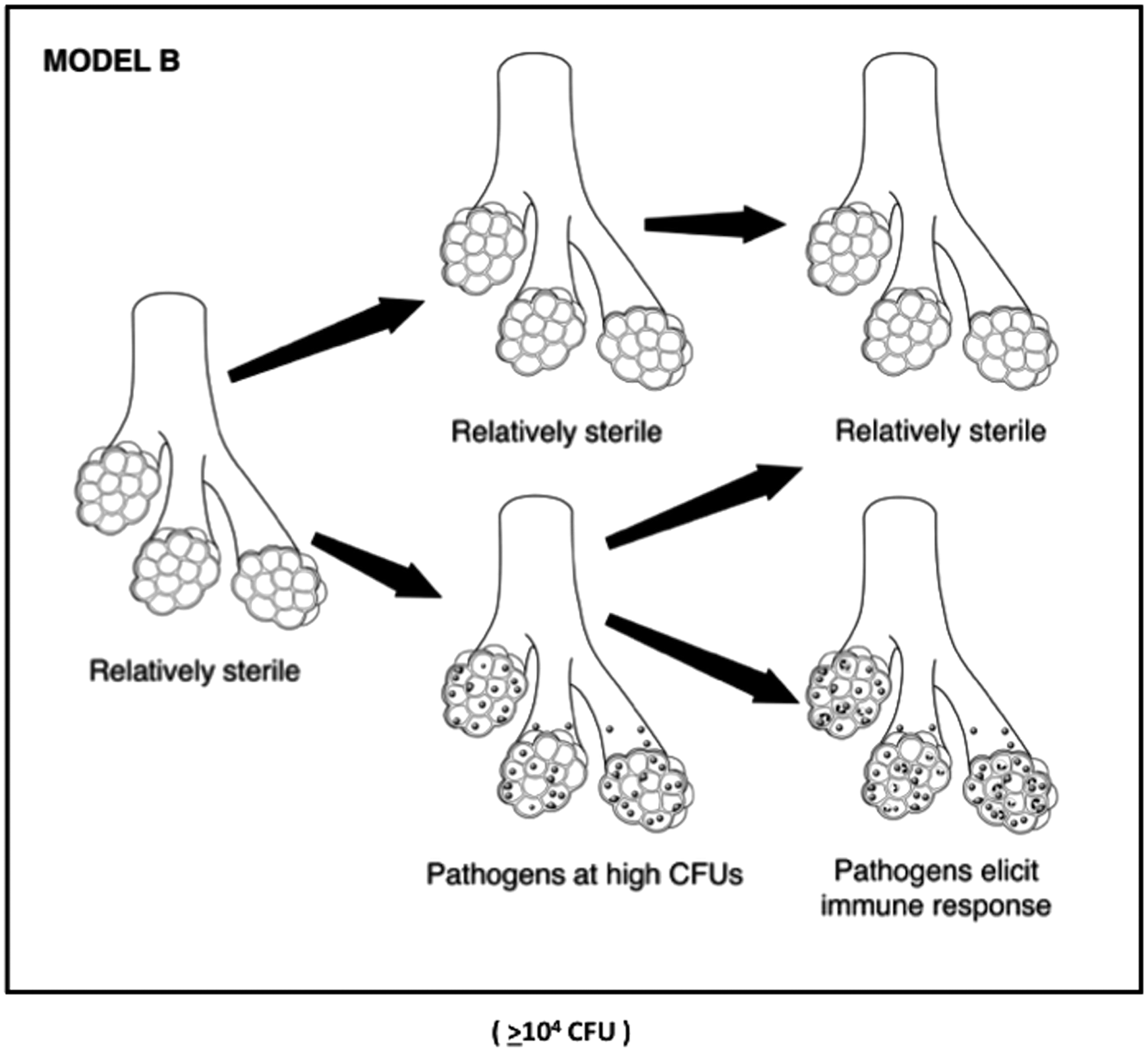
Proposed new hypothesis for pneumonia pathogenesis.
We found that 21 of 37 patients had bronchoalveolar lavages performed because of clinical suspicion of VAP. However, only 13 of these patients had VAP, defined as
Unfortunately, analysis of the clinical symptoms did not demonstrate any differences in those who did and did not develop pneumonia according to quantitative bacterial cultures (bBAL). This was the same for patients with positive surveillance cultures (+mBAL). This group did not reveal any significant differences between those who developed VAP and those who did not.
This study is the first to our knowledge to perform serial quantitative cultures prospectively on a population of mechanically ventilated trauma patients. This design is unique in that it provides the opportunity to follow the pulmonary flora of ventilated trauma patients longitudinally. This also is the first microbial characterization of pulmonary flora in mechanically ventilated trauma patients early in their hospitalization. Contrary to our hypothesis, a significant percentage of critically injured, ventilated adults developed high bacterial burdens in the lungs early during their courses. Although many of these patients went on to develop clinical signs of pneumonia, a significant number cleared these bacteria without ever being found to have suspicion of VAP. Defining patient characteristics that separate these two groups requires further study.
There are some notable limitations of this study that warrant mention. First, it was significantly limited by the sample size, which was only 37 patients. This study is part of an NIH-funded project evaluating the pulmonary flora of critically injured, ventilated patients; and patient enrollment is continuing which should eventually overcome this drawback. Another possible limitation is the inherent heterogeneity of trauma patients. Although ISS scores were similar for all groups, different injuries and injury mechanisms can have variable effects on the pulmonary flora. Furthermore, it is difficult to determine which patients had aspirated prior to hospital arrival. The finding that more than half of the patients had high CFUs within 48 hours of admission suggests a large number of aspirations in our population. The wide variety of pathogens cultured, the multitude of antibiotics used, and the small sample deterred investigations into other salient topics such as the influence of antibiotics used for all causes (VAP treatment, pre-procedural prophylaxis, treatment for other infectious processes) on the pulmonary flora, but this certainly is a topic that will be investigated as enrollment increases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
This study was supported by grants from the National Institutes of Health (NIH-R01 GM115353) and the Vanderbilt Institute for Clinical and Translational Research (VICTR Nos. 1824 and 1083) and other NIH funding (NIH-CTSA 1 UL1 RR024975).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.