
Abstract
Abstract
Background:
The objective was to identify the clinical and laboratory parameters, ultrasonographic (USG) morphology, and to predict surgical treatment for patients with tubo-ovarian abscess (TOA).
Patients and Methods:
Data for a total of 318 patients with a diagnosis of TOA between January 2005 and December 2016 were analyzed retrospectively at a referral center in Turkey. Patients requiring surgical treatment were compared with those who did not with respect to demographic characteristics and clinical, USG, and laboratory findings.
Results:
Ninety-three (29.25%) patients whose medical treatment failed underwent surgical intervention and a minimally invasive drainage procedure. Menopausal status, diabetes mellitus, long-term intrauterine device use, fever at admission, bilateral and multi-cystic TOA, and TOA size are risk factors for surgical treatment. An abscess size of 6.5 cm was a significant indicator for surgical intervention (odds ratio = 16.632; 95% confidence interval 8.745–31.632; p < 0.05). The area under the curve (AUC = 0.868) in the receiver operating characteristic (ROC) curve analysis was found to be statistically significant for TOA size, with a threshold value of 6.5 cm. The recommended cutoff value for erythrocyte sedimentation rate (ESR) was 61.0 mm/h, and the cutoff point of the C-reactive protein (CRP) level in the ROC analysis was found to be 24.5 mg/dL. There were no complications in the USG-guided drainage surgical treatment group.
Conclusion:
The TOA size, complex multi-cystic mass image, CRP, and ESR are useful indicators as to whether surgical treatment is required for the management of TOA. The USG-guided drainage was less invasive with fewer complications and should be the preferred surgical treatment.
T
Lower abdominal pain, fever, chills, and vaginal discharge symptoms may be seen in patients with TOA, similar to PID. Fever may not be seen in all TOA patients, however [6,7]. The TOA may be present with acute abdominal pain, if ruptured, and signs of sepsis can be seen. Therefore, early diagnosis and management of TOA are of vital importance because diagnosis and treatment delay can negatively affect fertility and even can be fatal [4,8].
Primarily, a complete history should be taken from patients with TOA, and a pelvic examination should be performed. In addition to biochemical tests, a complete blood cell count, a C-reactive protein (CRP) test, erythrocyte sedimentation rate (ESR), and a pregnancy test should be performed because results may affect the choice of antibiotic agents [9]. For pelvic imaging, an initial pelvic ultrasonography (USG) should be preferred. The USG is non-invasive, less expensive, and radiation-free and has sensitivities of 98.8% and a specificity of 93%; USG can distinguish simple cysts, ectopic pregnancy, and uterine fibroids [4]. If appendicitis, phlegmon, or an abscess associated with inflammatory bowel disease is suspected, computed tomography (CT) or magnetic resonance imaging (MRI) can be used. Thick-walled and rim-enhancing adnexal mass appearance indicates inflammatory events. If TOA findings are seen in post-menopausal situations, pelvic malignancy should be investigated [10,11].
The optimal treatment for patients with TOA is still unclear, controversial, and there is no consensus. The TOA treatment consists of broad-spectrum antibiotic agents, minimally invasive drainage procedure, invasive surgical procedure (laparotomy or laparoscopy), or a combination of these interventions [4,8]. The most commonly used medical treatment regimen is the completion of intravenous (IV) broad-spectrum antibiotic agents followed by oral antibiotic agents [9,12]. Despite medical treatment, 25% to 30% of patients with TOA may need surgical intervention [4,9,13]. Many clinical, laboratory, and USG parameters have been evaluated in the literature to predict the necessity of surgical treatment. Increased age, higher leukocyte levels, CRP and ESR levels, neutrophil-lymphocyte rate, and TOA size greater than 6.5 cm are risk factors for surgical treatment [4,8,9,12]. It is not known, however, exactly which parameter is most determinative.
In this study, we aimed to identify clinical and laboratory parameters, USG morphology, and predict which patients with TOA require surgical treatment.
Patients and Methods
We retrospectively analyzed data of 339 patients who underwent medical treatment or surgical interventions for diagnosis of TOA between January 2005 and December 2016 at the department of gynecology, Hitit University Education and Research Hospital (a tertiary referral center), Corum, Turkey. A total of 21 patients were excluded from the study because data were incomplete for 12 patients, and nine patients had a pathology result of malignant tumors. When data of the 318 patients included in the study were evaluated, surgical interventions were performed in 93 (29.25%) patients because of medical treatment failure. The study was reviewed by the local Institutional Review Board, and written informed consent was obtained from the participants at the time of hospitalization for future data use.
The TOA was diagnosed according to classic PID findings (abdominal or pelvic pain, cervical and adnexal sensitivity to vaginal examination, one or more of the following minor criteria: Fever (>38.3°C), leukocytosis (>10,000/mL), higher ESR (>15 mm/h) and presence of mass on pelvic USG). Physical and pelvic examinations were performed on all the patients with TOA, and venous blood samples were taken for laboratory evaluation before antibiotherapy.
Initially, binary IV antibiotic agents (clindamycin and gentamicin or ceftriaxone and metronidazole) were administrated as medical treatment for at least three days, and IUDs were removed after 48 hours. At the end of 72 hours, IV antibiotherapy for patients with clinical improvements was completed within seven days, and patients were discharged with 100 mg of oral doxycycline for a total 14 days. If no clinical response was obtained at the end of this process (fever >38.3°C, positive peritoneal sign, no decrease in TOA size, persistent pelvic pain, or rupture of TOA), patients with TOA underwent surgical intervention. The USG-guided transvaginal abscess drainage, uni- or bilateral salpingo-oophorectomy via laparoscopy or laparotomy, total hysterectomy combined with uni- or bilateral salpingo-oophorectomy via laparoscopy or laparotomy were performed in surgical intervention. The CT-guided abscess drainage was not performed because there was no educated and experienced radiologist. If TOAs are ruptured, multi-loculated, or difficult to access via transvaginal USG, laparoscopy or laparotomy is preferred.
Data were collected from patients' files for sociodemographic characteristics, menopausal status, duration of IUD use, history of tubal ligation, previous pelvis surgical procedure, pelvic USG findings, clinical and laboratory outcomes, operation types, and complications. Patients were divided into two groups: Successful medical treatment and surgical intervention required. The two groups were compared with respect to sociodemographic characteristics, pelvic USG findings, and clinical and laboratory outcomes. Operation type and complications from surgical procedures were also compared in the surgical intervention group.
Statistical analyses were performed using the SPSS 15.0 for Windows (SPSS, Chicago, IL). The Kolmogorov-Smirnov test was used to examine the continuous variables, with normal and without normal distributions. The Independent Samples t test was used for the normally distributed continuous variables. The Mann–Whitney U test was used for the continuous variables that were not normally distributed. Nominal variables were analyzed using the Pearson chi-square or Fisher exact test, when applicable. Continuous variables were presented as mean-standard deviation (SD), and categoric variables were presented as the number of cases and percentages. Logistic regression analyses were used to evaluate the effect of variables on the odds of a patient with TOA requiring surgical treatment. A receiver operating characteristic (ROC) curve was used to determine cutoff with sensitivity and specificity values for predicting surgical intervention for TOA treatment. Statistical significance was considered as p < 0.05.
Results
Sociodemographic characteristics of the patients with TOA are given in Table 1. The patients in the surgical interventions group were older, and the duration of IUD use was longer (p < 0.05). More patients in menopause, patients with diabetes, and patients with fever (>38.3°C) at admission were also in the surgical intervention group (p < 0.05).
BMI = body mass index; IUD = intrauterine device.
Statistically significant.
The USG findings of patients with TOA are summarized in Table 2. The mean TOA size was significantly larger in the surgical treatment group (5.53 ± 2.04 vs. 8.92 ± 3.18, p < 0.001). The surgical management group also had a greater number of bilateral TOA images and complex multi-cyst images on the USG (p < 0.05). An abscess size of 6.5 cm was a significant indicator for the risk of surgical intervention (odds ratio [OR] = 16.632; 95% confidence interval [CI] 8.745–31.632; p < 0.001). Likewise, a multi-cystic mass image on the USG was also a significant indicator for the risk of surgical intervention (OR = 3.652; 95% CI 2.204–6.062; p < 0.001).
Statistically significant.
Clinical and laboratory outcomes of the patients with TOA are shown in Table 3. While hemoglobin and hematocrit levels were lower in the surgical treatment group, leukocyte counts, neutrophil counts, lymphocyte counts, monocyte counts, platelet counts, red blood cell distribution width (RDW), neutrophil to lymphocyte rate (NLR), platelet to lymphocyte ratio (PLR), CRP and ESR levels were higher (p < 0.05), and the duration of hospitalization was longer in this group (p < 0.05).
Hb = hemoglobin; Htc = hemotocrit; RDW = red cell distribution width; NLR = neutrophil/lymphocyte ratio; PLR = platelet/lymphocyte ratio; CRP = C-reactive protein.
Statistically significant.
Operations and complications in the surgical treatment group are presented in Table 4. Of the 93 patients requiring a surgical procedure, 47 (50.54%) underwent abscess drainage, nine (19.15%) patients via laparotomy, 15 (31.91%) patients via laparoscopy, and 23 (48.94%) patients via USG-guided drainage (p = 0.004). There were no complications in patients with USG-guided drainage (p < 0.001). There was no statistical significance in terms of complications and surgical procedures performed between patients with TOA undergoing laparotomy and laparoscopy (p > 0.05).
USG = ultrasonography.
Statistically significant.
Table 5 describes the cutoff values of abscess size, leukocyte count, and CRP and ESR levels to predict surgical treatment. The estimated areas under the ROC curves for abscess size, leukocyte count, CRP levels, ESR, NLR, and PLR are shown in Figure 1. The AUC ( = 0.868) in the ROC analysis was found to be statistically significant for TOA size, with a cutoff value of 6.5 cm (95% CI 0.827–0.908, sensitivity 84.9%, specificity 74.7%). The recommended threshold for leukocyte count was found to be 15.50 (103) (AUC = 0.689, 95% CI 0.619–0.758, sensitivity 66.7%, specificity 72.7%). The cutoff point of CRP levels in the ROC analysis was found to be 24.5 mg/dL (AUC = 0.811, 95% CI 0.761–0.863, sensitivity 67.7%, specificity 76.4%). The best cutoff level of the ESR was 61.0 mm/h in the ROC analysis (AUC = 0.946, 95% CI 0.919–0.973, sensitivity 80.6%, specificity 90.8%).
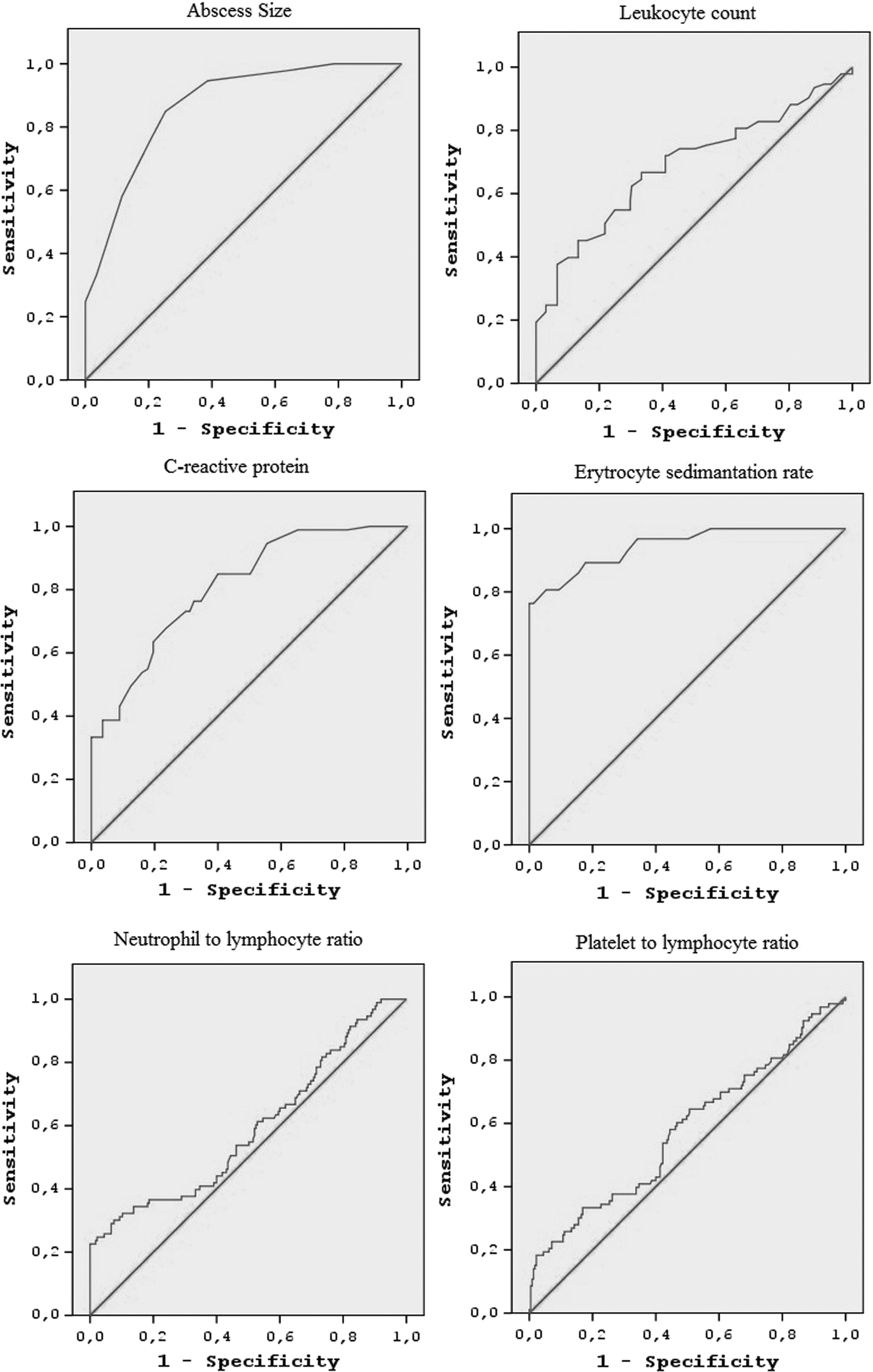
Receiver operating characteristic curves for abscess size, C-reactive protein level, erythrocyte sedimentation rate, neutrophil to lymphocyte ratio, and platelet to lymphocyte ratio in predicting the surgical treatment.
AUC = area under the curve; CI = confidence interval; CRP = C-reactive protein; ESR = erytrocyte sedimentation rate.
Statistically significant.
Discussion
In this retrospective study, the clinical and laboratory outcomes and the USG findings of 318 patients with TOA included in the study were analyzed to determine which parameters could be used to predict whether a patient will require surgical treatment. Menopausal status, diabetes mellitus, longer duration of IUD use, fever at admission, bilateral and complex multi-cyst appearance, ESR 61.0 mm/h, CRP >24.5 mg/dL, and TOA size >6.5 cm have been found to be risk factors for surgical treatment.
The TOAs, which are usually seen in the reproductive age group and in those presenting with lower abdominal or pelvic pain, fever, chills, and vaginal discharge, are polymicrobial inflammatory masses mostly involving the fallopian tubes, ovaries, and adjacent pelvic organs. Patients suspected of having TOA should first have a complete physical and pelvic examination performed, and then the required laboratory tests and pelvic imaging methods should be used. Early diagnosis and treatment are very important because TOA can affect fertility and, more importantly, it can be fatal [4,8,12,14].
Sociodemographic risk factors for medical treatment failure in TOA management are conflicted in the literature. While older age, an increased number of pregnancies, previous pelvic surgery, menopausal status, IUD existence and longer duration of IUD existence are shown as risk factors in some studies [4,15–17], some researchers did not find them to be risk factors [8,9]. Although the need for surgical intervention in patients with TOA has been shown to occur at an older age than those who respond to medical treatment [4,15–17], there are also studies claiming that there is no difference [8,9]. In our study, the age of the patients in the surgical treatment group was significantly higher. In our clinic, if the patients in the older age group do not have fertility desires, the decision to have surgical intervention can be made more easily.
Some studies have reported that IUD usage doubles the PID probability [18], and IUDs were detected in 20% to 50% of patients with TOA [19]; however, IUD persistence was not reported to increase the risk of surgical intervention [4,8]. In our study, we found that the IUD was used by 25.16% in patients with TOA. In addition, we found that although the presence of an IUD did not increase the risk of surgical treatment, the longer duration of IUD use increased the risk of surgical intervention by 1.308. Similar to the study by Gungorduk et al. [8], there were no differences between medical and surgical treatment groups in terms of body mass index, tobacco and alcohol use, number of gravidity and parity, history of tubal ligation, condom use, and previous pelvic surgical procedures. The number of patients with diabetes was higher in the surgical intervention group and, as in the literature [4,8], the number of patients with fever was higher in the surgical treatment group. This result indicates that fever at admission is associated with poor prognosis for medical treatment in patients with TOA.
TOA is a relatively rare entity in the post-menopausal period and has been reported in the literature to number 1% to 12% of patients with TOA [15,20]. In the present study, 35 (11%) of the patients with TOA were found to be in the post-menopausal period. It has been reported that the frequency of malignant pelvic tumors in post-menopausal women with TOA increased to 33% [20]. Some researchers, however, have not found pelvic malignancy in these women [9,21]. In this study, the pathology findings of 9/35 post-menopausal patients with concomitant malignancy were compatible with findings of TOA in addition to pelvic malignancy. Because of an increased risk of pelvic malignancy in patients with TOA, a complete pelvic examination must be performed to exclude a concomitant pelvic malignancy.
Pelvic USG has been used as a first choice by gynecologists in the evaluation of pelvic masses, although there is no specific finding for TOA diagnosis. With USG, the appearance of TOA may be confused with hemorrhagic cyst, endometrioma, benign-malignant ovarian tumors, and gastrointestinal stromal tumors [3]. To receive a diagnosis of TOA, the image detected by pelvic USG should be supported by clinical findings (pelvic pain, cervical or adnexal tenderness on vaginal examination) and laboratory test outcomes. In contrast to poor blood flow in TOA, pelvic masses show a rich blood flow on the Doppler USG [22]. Transvaginal USG was the most preferred method for pelvic imaging in this study.
If the image was suspicious on the pelvic USG, patients underwent a pelvic CT or pelvic MRI. Kinay et al. [4] classified USG images into three categories as a thickened unilocular cyst (34.1%), a complex multi-cyst (44.5%), and pyosalpinx (21.3%) and claimed that these USG images did not predict TOA treatment and were inadequate to show the success of medical treatment. When we grouped patients similarly, we found thickened unilocular cysts in 37.7% of patients, a complex multi-cyst in 34.6%, and pyosalpinx at 27.7%, and we observed that the appearance of a complex multi-cyst on USG increased the risk of surgical intervention by 3.652-fold, which was statistically significant. This may be because pyosalpinx inhibits the passage of pathogen micro-organisms to the peritoneal cavity and the easy access of antibiotics to the unilocular cyst that, in appearance, resembles an abscess.
Several researchers investigated the impact of abscess size on the outcome of TOA treatment such as medical treatment result in the need for surgery and its complications. They found that as the abscess size increases, the success rate of medical treatment decreases, with an increased rate of surgical intervention and complications and different cutoff values of abscess size [4,8,9,14]. We found that an abscess size of more than 6.5 cm predicted the surgical decision, with a sensitivity of 84.9% and a specificity of 74.7%.
Although no specific antibiotic treatment is used for TOA, broad-spectrum IV antibiotherapy is the first choice as medical treatment. It is quite effective (67%–75%), but sometimes if there is no clinical improvement within 72 hours or a rupture of TOA occurs, surgical interventions must be considered [4,19,23]. In our study, 29.25% of the patients with TOA required surgical interventions in accordance with the literature.
There are many laboratory tests, including inflammatory markers, used in the diagnosis, treatment, and follow-up of PID and TOA. Leukocytosis and increased ESR and CRP levels are known to occur in patients with PID and TOA [14]. In a recent study, it was suggested that NLR, PLR, and RDW are the predictive parameters of TOA [12]. The ESR and CRP may also predict the severity of acute PID [24]. It has been claimed that an ESR of more than 50 mm/h is the best diagnostic marker for TOA diagnosis [25]. In another study, combined ESR and CRP (ESR >19.5 mm/h and CRP >11.5 mg/dL) are good markers for PID severity [26]. In contrast to the above-mentioned studies, there are other studies showing that these laboratory results do not increase in patients with PID and TOA [9,14].
There are also studies investigating many laboratory tests that can predict the need for surgical interventions in patients with TOA. Kinay et al. [4] and Gungorduk et al. [8] investigated the relationship between TOA and inflammatory markers as to who required surgical treatment. Kinay et al. [4] found that CRP does not change, but ESR does increase. Gungorduk et al. [8] showed that both CRP and ESR increased, and they found that the ESR with a threshold level of 63.0 mm/h (AUC = 0.836), a sensitivity of 82.7%, and a specificity of 73.7% were related to the need for surgical intervention; on the other hand, CRP with a cutoff point of 21.0 mg/dL (AUC = 0.836), had a sensitivity of 65.8%, and a specificity of 82.3%. We found ESR with a cut-off level of 61.0 mm/h (AUC = 0.946), a sensitivity of 80.6% and a specificity of 90.8% is related to the need for surgical intervention; on the other hand, CRP with a threshold level 24.5 mg/dL (AUC = 0.811), had a sensitivity of 67.7% and a specificity of 76.4%. We also evaluated NLR, PLR, and RDW in patients with TOA, but these markers are unfavorable for predicting a surgical intervention.
While the most important limitation of our study is its retrospective design, the major strength of our study is that we were able to investigate the parameters in a single study, at the same time, and were able to conclude with a result.
Conclusion
Predicting which patients with TOA will require surgical intervention at an early stage is very important when considering morbidity and death. In the present study, we found that abscess size (>6.5 cm), a complex multi-cyst image, and laboratory parameters (ESR >61.0 mm/h and CRP level >24.5 mg/dL) can aid in the decision to perform surgical interventions. The USG-guided drainage procedure, which is less invasive with fewer complications, should be the first choice in surgical treatment.
Footnotes
Acknowledgment
An abstract of this article was presented at the European Society for Gynaecological Endoscopy 26th Annual Congress, October 18–21, 2017, Antalya, Turkey.
Author Disclosure Statement
No competing financial interests exist.