
Abstract
Abstract
Background:
The skin bacterium Propionibacterium acnes has been reported to be responsible for surgical site infections (SSIs). Skin disinfection before surgery therefore is of the utmost importance in the prevention of SSIs caused by skin bacteria.
Methods:
We assessed the susceptibility of clinical isolates of two skin bacteria, P. acnes and Staphylococcus epidermidis, to disinfectants.
Results:
The range of chlorhexidine digluconate (CHG) minimum inhibitory concentrations (MICs) for P. acnes isolates was 0.25–1 mcg/mL. Furthermore, the minimum bactericidal concentrations (MBCs) for a range of disinfectants were determined to evaluate their rapid bactericidal activity. The MBC range of CHG against the P. acnes isolates was 4,096–>32,768 mcg/mL (MBC80 16,384 mcg/mL) after one minute of exposure and 1,024–32,768 mcg/mL (MBC80 8,192 mcg/mL) after five minutes, indicating that some strains required a CHG MBC higher than the commercial concentration of 2% (20,000 mcg/mL). In contrast, the MBCs of glutaraldehyde, sodium hypochlorite, povidone–iodine, ethanol, benzalkonium chloride, and olanexidine gluconate were all sufficiently lower than their commercial concentrations. In S. epidermidis, the MBC range of CHG was 128–1,024 mcg/mL at one minute of exposure and 4–8 mcg/mL at five minutes.
Conclusions:
Different skin bacteria have different susceptibilities to disinfectants. To prevent SSIs, the selected disinfectant agent and the disinfection time should have bactericidal activity toward all the bacteria that pose a risk of infection.
P
Povidone–iodine and chlorhexidine digluconate are frequently used as skin disinfectants. Alcoholic chlorhexidine; i.e., chlorhexidine digluconate combined with alcohol, also is used and has the advantages of having a higher bactericidal activity and being fast drying. For example, Darouiche et al. reported that alcoholic chlorhexidine is significantly better than 10% povidone–iodine at preventing SSIs [8]. In contrast, Lee et al. found that P. acnes can persist on the skin after disinfection with 2% chlorhexidine digluconate [9]. Disinfection activity can be estimated by measuring the susceptibility of each bacterium to each disinfectant. Currently, there are no reports describing the susceptibility of P. acnes isolates to disinfectants. Therefore, in this study, we examined the susceptibilities of isolates of two skin bacteria, P. acnes and S. epidermidis, to disinfectants. These data will indicate the appropriate disinfectant to use against skin bacteria to prevent SSIs.
Materials and Methods
Bacterial strains
Twelve P. acnes and seven S. epidermidis isolates were obtained from acne patients at our hospital in Japan [10]. In addition, 15 P. acnes isolates were obtained from inpatients in various departments of the Tokyo Medical University Hachioji Medical Center (Table 1). The P. acnes isolates were grown for 48 h on modified GAM agar (Nissui Pharmaceutical, Tokyo, Japan) at 35°C under anaerobic conditions. Staphylococcus epidermidis was grown for 24 h on tryptone soy agar (TSA) at 35°C under aerobic conditions [10].
CVP = central venous pressure monitor; IVH = intravenous hyperalimentation.
Analysis of minimum inhibitory concentration (MIC) of disinfectants
The MIC against P. acnes was determined by an agar dilution procedure using modified GAM agar under anaerobic conditions for 48 h [10]. The disinfectant agent used was a 20% chlorhexidine gluconate solution (Wako Pure Chemical Industries, Osaka, Japan).
Analysis of minimum bactericidal concentration (MBC) of disinfectants
The MBC analysis was performed by a broth microdilution method according to the Clinical Laboratory Standard Institute [11]. Bacteria were suspended to a concentration of 1010 colony-forming units (CFU)/mcL in test solution containing each concentration of disinfectant. Subsequently, 1 mcL of the test solution was added to 100 mcL of neutralization solution (3% TWEEN® 80 [Sigma-Aldrich Co., St. Louis, USA], 0.3% soybean lecithin [Wako], 0.5% sodium thiosulfate [Wako], 0.1%
Analysis of bactericidal time course
The bactericidal activities of chlorhexidine digluconate and olanexidine gluconate at different exposure times were determined against P. acnes ATCC11828 and S. epidermidis ATCC14490. The bacteria were resuspended at approximately 106 CFU/mL in phosphate-buffered saline and were inoculated with each disinfectant independently at 100 mcg/mL. The bacterial suspensions were spread on modified GAM agar and TSA plates after addition of the neutralization solution. The colonies of the two organisms were counted after incubation for 72 h under anaerobic conditions or 48 h under aerobic conditions, respectively. Furthermore, the bactericidal activity of the disinfectants in the presence of 5% inactivated fetal bovine serum (FBS) was measured to mimic the reduced activity of disinfectants when used on the human body.
Results
Chlorhexidine digluconate MICs against P. acnes isolates
The MICs of chlorhexidine digluconate against the different P. acnes isolates were measured, and the data are shown in Fig. 1. The MICs ranged from 0.25–1 mcg/mL, and there was no difference in the MICs against P. acnes isolated from acne patients and inpatients.
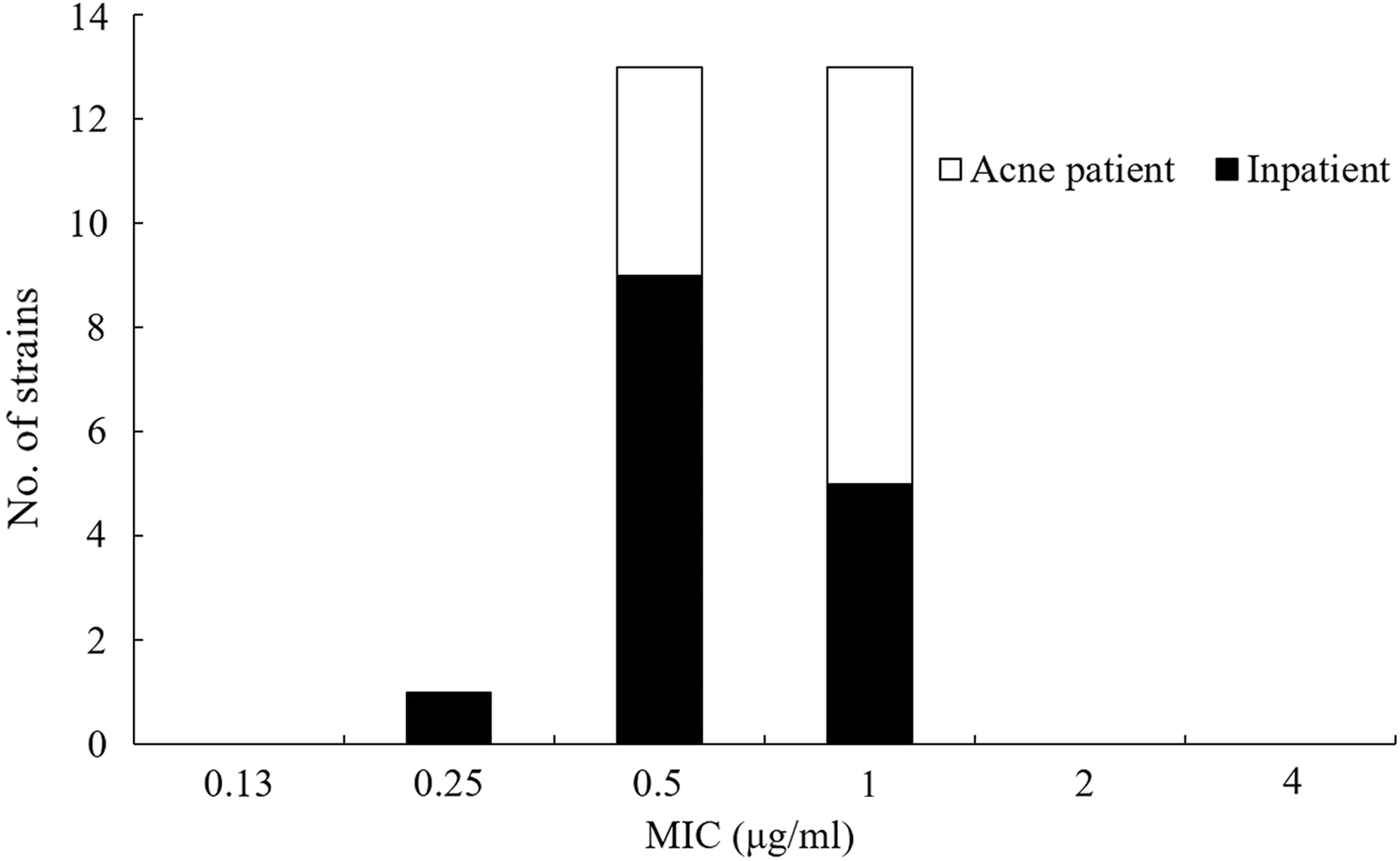
Distribution of minimum inhibitory concentrations for chlorhexidine digluconate in Propionibacterium acnes isolates.
MBC of other disinfectants against P. acnes and S. epidermidis isolates
Disinfectants need to have rapid bactericidal activity. Therefore, measurement of MIC, which evaluates activity over a long period of time (P. acnes was incubated for 48 h for example), might not evaluate disinfectant activity appropriately. When the MBCs, which evaluate activity over a short period of time, were measured, there was no difference in the MBCs for any of the tested disinfectants against P. acnes isolated from acne patients or from inpatients (Table 2). After one minute of exposure, glutaraldehyde, which is used for instrument disinfection, and NaClO, which is used for floor disinfection, showed MBCs that were lower than their recommended use concentrations (i.e., 2.0% [20,000 mcg/mL] and 0.1% [1,000 mcg/mL], respectively) [12]. After one minute of exposure, ethanol and benzalkonium chloride, which are both used for skin disinfection, also showed MBCs that were lower than their recommended use concentrations (i.e., 80% [800,000 mcg/mL]) and 0.2% [2,000 mcg/mL], respectively). After one minute of exposure, povidone–iodine and olanexidine gluconate, which are used for pre-operative disinfection, showed MBCs that were lower than concentrations recommended for use (i.e., 10% [100,000 mcg/mL] and 1.5% [15,000 mcg/mL, respectively]) [13]. In contrast, after one minute of exposure, the MBC80 of chlorhexidine digluconate for P. acnes isolated from acne patients and inpatients was 8,192 and 16,384 mcg/mL, respectively. It should be noted that four P. acnes strains, including a strain isolated from one acne patient and strains 21, 22, and 26, isolated from inpatients, required chlorhexidine digluconate MBCs of 32,768 mcg/mL or more, which are higher than the recommended use concentration (2% [20,000 mcg/mL]) (Fig. 2). For S. epidermidis isolates, after one minute of exposure, all the tested disinfectants had MBCs lower than their recommended use concentrations (Table 3).

Distribution of minimum bactericidal concentrations for chlorhexidine digluconate in Propionibacterium acnes isolates.
BKC = benzalkonium chloride: CHG = chlorhexidine digluconate; EtOH = ethyl alcohol; GA = glutaraldehyde; NaClO = sodium hypochlorite; OLG = olanexidine gluconate; PI = povidone–iodine.
BKC = benzalkonium chloride: CHG = chlorhexidine digluconate; EtOH = ethyl alcohol; GA = glutaraldehyde; NaClO = sodium hypochlorite; OLG = olanexidine gluconate; PI = povidone–iodine.
Bactericidal time course for chlorhexidine digluconate and olanexidine gluconate
The temporal bactericidal activities of both chlorhexidine digluconate and olanexidine gluconate also were measured in this study. For P. acnes, chlorhexidine digluconate had reduced the bacterial population to 10−2 and 10−4 after 5 and 10 min of exposure, respectively. Following this, P. acnes was undetectable 30 min after exposure (Fig. 3A). When 5% FBS was added, the number of surviving P. acnes increased, and complete sterilization could not be achieved even after 30 min of exposure. In contrast, olanexidine gluconate achieved complete sterilization of P. acnes within 10 min of exposure, and there was no decrease in bactericidal activity in the presence of 5% FBS (Fig. 3C). For S. epidermidis, chlorhexidine digluconate and olanexidine gluconate achieved complete sterilization within five minutes of exposure (Fig. 3B, D).
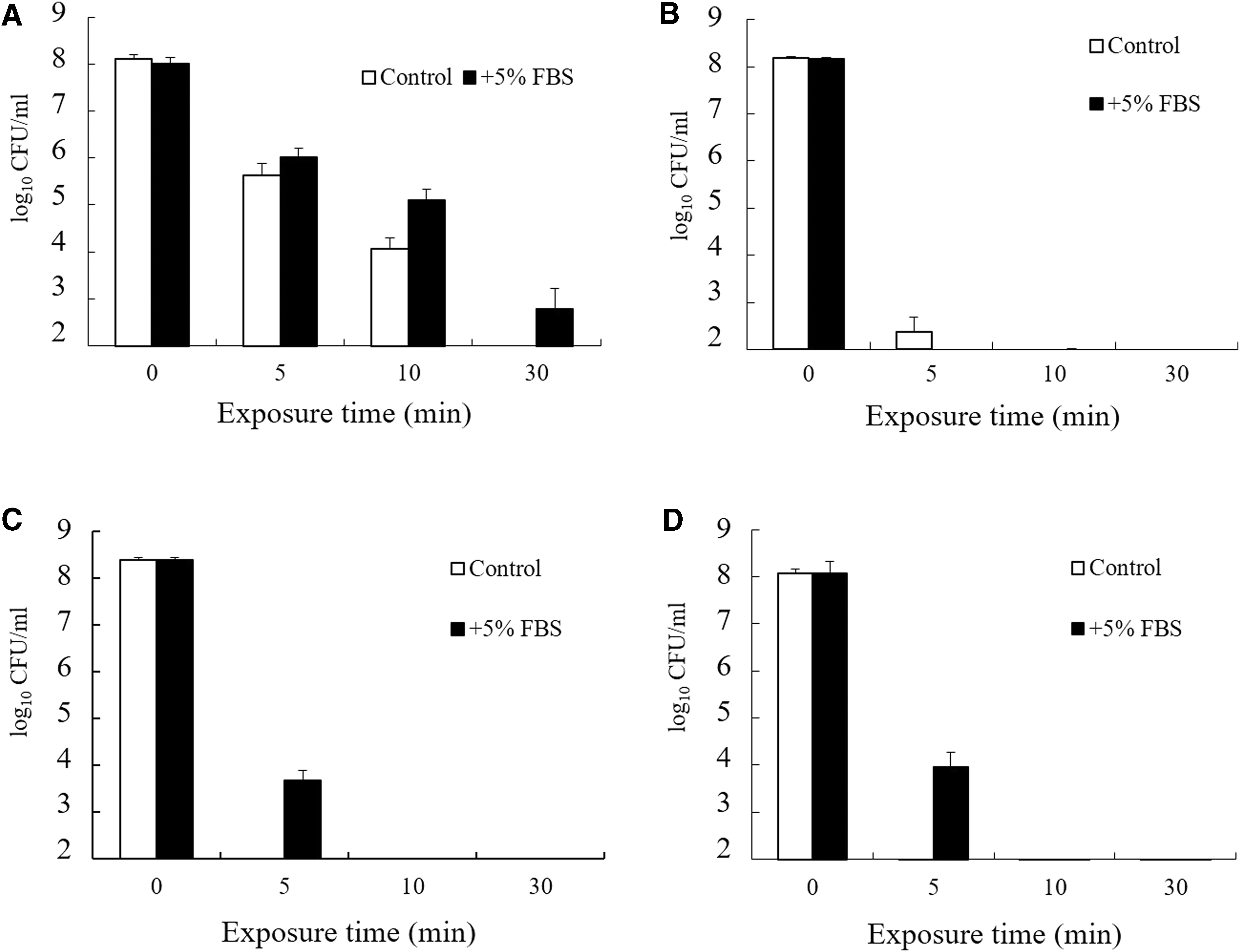
Activity of biguanide disinfectants. Bactericidal activity of chlorhexidine digluconate for
Discussion
In this study, we assessed the efficacy of a variety of disinfectants against P. acnes isolates. We concluded that the tested disinfectants, except for chlorhexidine digluconate, can kill P. acnes in a short period of time, because their MBCs after one minute of exposure were lower than their recommended use concentrations. In contrast, for some P. acnes isolates, chlorhexidine digluconate had MBCs of 32,768 mcg/mL or more after one minute of exposure, which is higher than its recommended use concentration of 2% (20,000 mcg/mL). Generally, chlorhexidine digluconate is combined with alcohol. According to this study, alcoholic chlorhexidine would be estimated to kill P. acnes in a short period of time because ethanol had a lower MBC against P. acnes. Saltzman et al. reported that the detection rates for P. acnes and coagulase-negative staphylococci (CNS) after treatment with 2% chlorhexidine gluconate +70% isopropyl alcohol were 12% and 4%, respectively [14]. These data suggest that P. acnes in the sebaceous glands is not well exposed to alcoholic chlorhexidine, although CNS could be killed readily on the skin surface. Therefore, although alcoholic chlorhexidine has both the ability to dry quickly and a high bactericidal activity, it cannot disinfect P. acnes completely if the exposure time is not sufficient.
In the clinical laboratory, the presence of P. acnes frequently is missed owing to its slow growth, and it often is considered a contaminant of the skin flora. In contrast, recently, the number of cases demonstrating the presence of P. acnes in SSIs in orthopedic and plastic surgery has increased [6]. Furthermore, a rapid detection method has been developed for P. acnes in clinical specimens. Thus, we estimate that the number of reported cases of P. acnes in SSIs will increase even further in the future [15].
In conclusion, this study demonstrated the susceptibilities of different P. acnes isolates to disinfectants. To prevent SSIs, the selected disinfectant agent and the disinfection time should have bactericidal activity toward all the bacteria that pose a risk of infection, and it is hoped that these data will contribute to the prevention of SSI caused by P. acnes.
Footnotes
Acknowledgments
The authors are grateful to Yutaka Nasu for providing the clinical isolates. This work was supported by the Matching Fund Subsidy for the Private Schools of Japan and was partially supported by a Pfizer Academic Contribution. The work was funded mainly by Otsuka Pharmaceutical Factory, Inc.
Author Disclosure Statement
No competing financial interests exist.