
Abstract
Abstract
Background:
Skin and soft tissue infections are common problems dealt with in emergency departments and medical offices. It is routine practice to prescribe antibiotic agents after incision and drainage of cutaneous abscesses. However, current evidence does not support prescribing oral antibiotic agents after surgical debridement. The aim of the present study was to determine the actual role of antibiotic agents after drainage of cutaneous abscesses.
Patients and Methods:
This was a prospective study of patients undergoing incision and drainage (I&D) of a subcutaneous abscess. Patients were randomly assigned either to receive antibiotic agents (group 1) or placebo (group 2) after I&D. The primary end point was resolution rate of the abscess at the seventh day. Secondary end points were pain at the seventh day and total time to full healing of the wound. P value <0.05 was considered statistically significant.
Results:
One hundred sixty-five patients were included for analysis. Age, gender, body mass index (BMI), and comorbidities did not differ substantially between groups. Chest and peri-anal abscesses were statistically more frequent in group 2, whereas neck abscesses were more frequent in group 1 (p = 0.02). Leukocyte count was also statistically higher in group 1 (p = 0.005). Resolution rate was 96% in group 1 and 93% in group 2, with no statistical difference between both (p = 0.28). Neither pain at seventh day nor time to full healing differed statistically between groups.
Conclusions:
Antibiotic agents are not necessary for uncomplicated subcutaneous abscesses after I&D. These cases can be managed safely on an outpatient basis without any increase in morbidity.
S
Most SSTIs result from infections with gram-positive cocci, particularly Staphylococcus aureus and group A streptococci [6–8]. Despite these bacteria being typical skin flora, they can cause infections when a disruption of the skin barrier has occurred. Gram-negative bacilli can also infect the skin and soft tissues, most often in gluteal and axillary regions [9]. Anaerobic bacteria typically are absent in cases of cellulitis. They are, however, responsible for severe cases of necrotizing fasciitis, in which they act as co-infecting organisms in conjunction with Staphylococcus aureus or group A streptococci [4–10].
It is common practice to prescribe antibiotic agents after incision and drainage (I&D) of cutaneous abscesses. However, current evidence suggests that there is no actual benefit of such practice and does not support prescribing oral antibiotic agents after surgical debridement [11]. Moreover, this raises the question as to whether antibiotic abuse or misuse in this setting might promote bacterial resistance. Perhaps a large, rigorous, and randomized clinical trial might be able to demonstrate that this practice causes more harm than benefit to patients. Even so, many authors continue to recommend the routine use of “simple” empiric antibiotic agents based on the most probable organisms causing SSTIs [12]. Empiric antibiotic coverage may be warranted in patients who are severely immunocompromised, those having a large area of cellulitis, lymphangitis, or those exhibiting signs and symptoms of systemic toxicity [13]
Patients and Methods
The study was conducted from November 2014 through May 2016 at General Zone Hospital (HGZ) No. 11 of the Mexican Institute of Social Security in Delicias, Mexico when authorization by the Local Ethical and Health Research Committee was granted. The study complied with the policies of Mexico's General Law of Health Research, as well as the Declaration of Helsinki, and written informed consent was obtained from all participants or legal representatives.
Eligible patients included only those older than 15 years affiliated with the institute, who were diagnosed with subcutaneous abscess and had not received antibiotic agents by any route in the recent past (up to 15 days prior) to I&D. Patients with history of malignancy, hematologic diseases, human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), splenectomy, necrotizing fasciitis, Fournier gangrene, diabetic foot, toxic shock syndrome, extensive cellulitis 5 cm or more, abscesses with peritoneal fistulization, bone/joint involvement, severe circulatory insufficiency, and patients likely to die in the short term were excluded.
Study design
In this single-blinded, randomized, placebo-controlled study, the patients admitted in the emergency department of HGZ No. 11 with a diagnosis of subcutaneous abscess were randomly assigned to receive or not to receive oral antibiotic treatment after undergoing I&D. Two study arms were designed as follows. Patients in group 1 (study group) were given analgesics and antibiotic treatment after I&D, whereas patients in group 2 (control) received analgesics and placebo. Analgesic treatment was provided by dipyrone 1 g and acetaminophen 1 g orally three times a day, as needed. Antibiotic coverage with ciprofloxacin 250 mg orally twice daily for 7 days was given to patients in group 1. Placebo pills were also prescribed every 12 hours for 7 days.
All medications were previously stored in plain bottles labeled as “Analgesic 1,” “Analgesic 2,” “Antibiotic 1, and “Antibiotic 2,” with the latter being the placebo pills. All patients were discharged immediately after I&D and follow-up visits were scheduled at 7, 14, and 21 days in the outpatient clinic. Patients were instructed to return to the emergency department as soon if they noticed continued signs and symptoms of ongoing infection after 48 hours of their initial treatment. Such signs and symptoms included malaise, intense local pain and hyperthermia, fever, induration, and redness (i.e., ongoing cellulitis). In such cases, the patients were admitted to the surgical ward and received broad-spectrum antibiotic agents until culture/antibiogram results were available to adjust to the specific drugs.
Randomization
After providing written informed consent, patients were randomly assigned to one group by means of closed envelopes in blocks of 10. The process was done by one of the researchers in all cases.
Data collection
Data were obtained prospectively and recorded, and included demographic information (age, gender, BMI, and comorbid conditions), volume of abscess cavity, resolution of the abscess at the seventh day, pain at the seventh day, and time to complete healing.
Surgical procedure
Abscess sites were prepped with iodine povacrylex (0.7% available iodine) and isopropyl alcohol, 74% w/w (DuraPrep™; 3M™, St. Paul MN) or 0.8% iodopovidone (GERMISIN Espuma; Farmacéuticos Altamirano de México S.A. De C.V., Ciudad De Mexico, Mexico), as available. Local anesthesia was achieved using 2% xylocaine, and a skin incision was made with a scalpel blade number 21 over a length of at least half the diameter of the abscess as estimated clinically. The incision was deepened as necessary to access the abscess cavity. The content was then evacuated completely and the cavity debrided thoroughly with several iodopovidone-soaked gauze pads. Next, the volume of the abscess cavity was estimated by infusing normal saline until the cavity was full. Finally, the incision was packed with gauze soaked in 0.5% hypochlorite solution and draped. Dressing changes twice daily were prescribed during the first seven days, with re-packing of the incision as described. On the first follow-up visit, dressing changes were modified to once per day if an appropriately granulated incision bed was observed.
Study end points
The primary end point was the rate of resolution of the abscess at the seventh day (first follow-up visit) in the two randomized groups. Resolution of abscess was defined as the presence of three or more of the following criteria: no local hyperthermia; no redness; no induration; and adequate granulation on incision bed. Resolution or failure to resolve at the seventh day was determined by a non-blinded researcher. Secondary end points were local pain on the seventh day and time to complete healing. Local pain was evaluated by means of the visual analogue scale (VAS). Time to complete healing was defined as the time elapsed from I&D to full epithelialization of the incision.
Statistical analysis
An analysis with intention-to-treat was done. Normality of data distribution was first determined by Kolmogorov-Smirnov test. In normally distributed data, continuous variables appear as mean ± standard deviation (SD), and were analyzed for homogeneity by using unpaired samples t-test, whereas non-normal continuous data are expressed as median ± interquartile range (IQR) and were tested for differences between two groups by Mann-Whitney U test. Categorical variables are expressed as N with percentage and were tested with χ2 or Fisher exact test, as appropriate. Statistical significance was defined as p < 0.05. Statistical analyses were performed using SPSS 20.0 for OSX (IBM SPSS Inc., Armonk, NY).
Results
From November 2014 through May 2016, 280 patients were admitted to the emergency department because of a diagnosis of subcutaneous abscess. Of these, 86 patients were excluded before randomization for the following reasons: age 15 years or younger (n = 5); ongoing malignancy (n = 6); HIV/AIDS (n = 2), Fournier gangrene (n = 4); necrotizing fasciitis (n = 3); diabetic foot (n = 43); wound abscess plus evisceration (n = 2); or refused to participate (n = 21). The remaining 194 patients were randomly assigned to I&D plus antibiotic (group 1; n = 101) or I&D plus placebo (group 2; n = 97). In group 1, one patient was subsequently excluded because no pus was evacuated after I&D (i.e., cellulitis without abscess), whereas in group 2, three patients were excluded for the same reason. Furthermore, seven patients were subsequently excluded in group 1 and five patients in group 2 because they took additional non-prescribed medications in the forms of pills, creams, ointments, or dry powders in the recent past prior to their abscess treatment. Thirteen patients did not attend the outpatient clinic for follow-up revision. A total of 165 patients remained suitable for outcome analysis (Fig. 1).

Flow diagram of patient selection. HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome.
Patient characteristics
Patient demographics, peri-operative data, and abscess characteristics are shown in Table 1. No difference was observed regarding the number of patients allocated to each study group (group 1, n = 84; group 2, n = 81). Other demographic and peri-operative data such as age, gender, BMI, comorbidities, and volume of the abscess were also comparable between both groups (Table 1).
Independent samples t-test.
Pearson χ2 test.
Statistically different as shown by χ2 post hoc testing.
SD = standard deviation; BMI = body mass index; DM2 = type 2 diabetes mellitus; SAH = systemic arterial hypertension; ESRD = end-stage renal disease.
There was, however, statistically significant differences with regard to abscess location (p = 0.02). Post hoc testing revealed that chest and peri-anal abscesses were statistically more frequent in the placebo arm, whereas neck abscesses were more frequent in the antibiotic group. Leukocyte count also was found to be higher in patients assigned to group 1 after I&D (p = 0.005).
End points
Resolution rates of the infectious/inflammatory process were not statistically different when testing both study arms (p = 0.28). Resolution rate in group 1 was 96% (n = 81), whereas it was 93% (n = 75) in group 2 (placebo). Overall, seven patients returned to the emergency department for revision after 48 hours because they noticed no improvement of the incision. After a thorough examination, no signs of ongoing infection or worsening were found in any of these patients, who were reassured and encouraged to continue with the treatment.
Assessment of pain by VAS revealed no statistical difference at the seventh day, nor did the time to full healing of the incision (Table 2). Eighty-eight percent of patients in group 1 and 90% of patients in group 2 achieved full epithelialization by the 21-day follow-up visit.
Pearson χ2 test.
Independent samples t-test.
VAS = visual analogue scale; SD = standard deviation.
Discussion
A cutaneous abscess is defined as focal, confined purulent infection with a well-defined cavity surrounded by an inflammatory process involving deep subcutaneous tissues. On physical examination, fluctuation suggests the presence of pus in the abscess cavity. Cellulitis, however, is a pyogenic infection of the skin without an organized cavity and is typically located in the epidermis, dermis, and shallow subcutaneous tissues [14]. Because cellulitis constitutes the acute phase of an SSTI, it is the only setting in which antibiotic agents are truly indicated. An already developed abscess, however, is the result of the body's defense mechanisms. In addition, pus consists of a build-up of serum, dead neutrophils, necrotic tissue, cholesterol and glucose. Most importantly, infective micro-organisms do not always contribute to the pus composition.
In this regard, we believe that there is a misunderstanding of the natural process of the development of an abscess, leading physicians to believe that the presence of pus within subcutaneous tissues constitutes the infectious material itself, and consequently, to administer antibiotic agents. Also, we have noted that medical staff at our institution prefer to “prevent” by admitting and prescribing broad-spectrum antibiotic agents to patients with peri-anal abscesses or surgical site infections (SSIs) because they are concerned about the medical and legal consequences that may arise should those infections progress to Fournier gangrene or necrotizing fasciitis. According to the results of this study, however, this premise is not only unnecessary but also exaggerated because we managed every single patient on an outpatient basis and observed no adverse outcomes (Fig. 2).
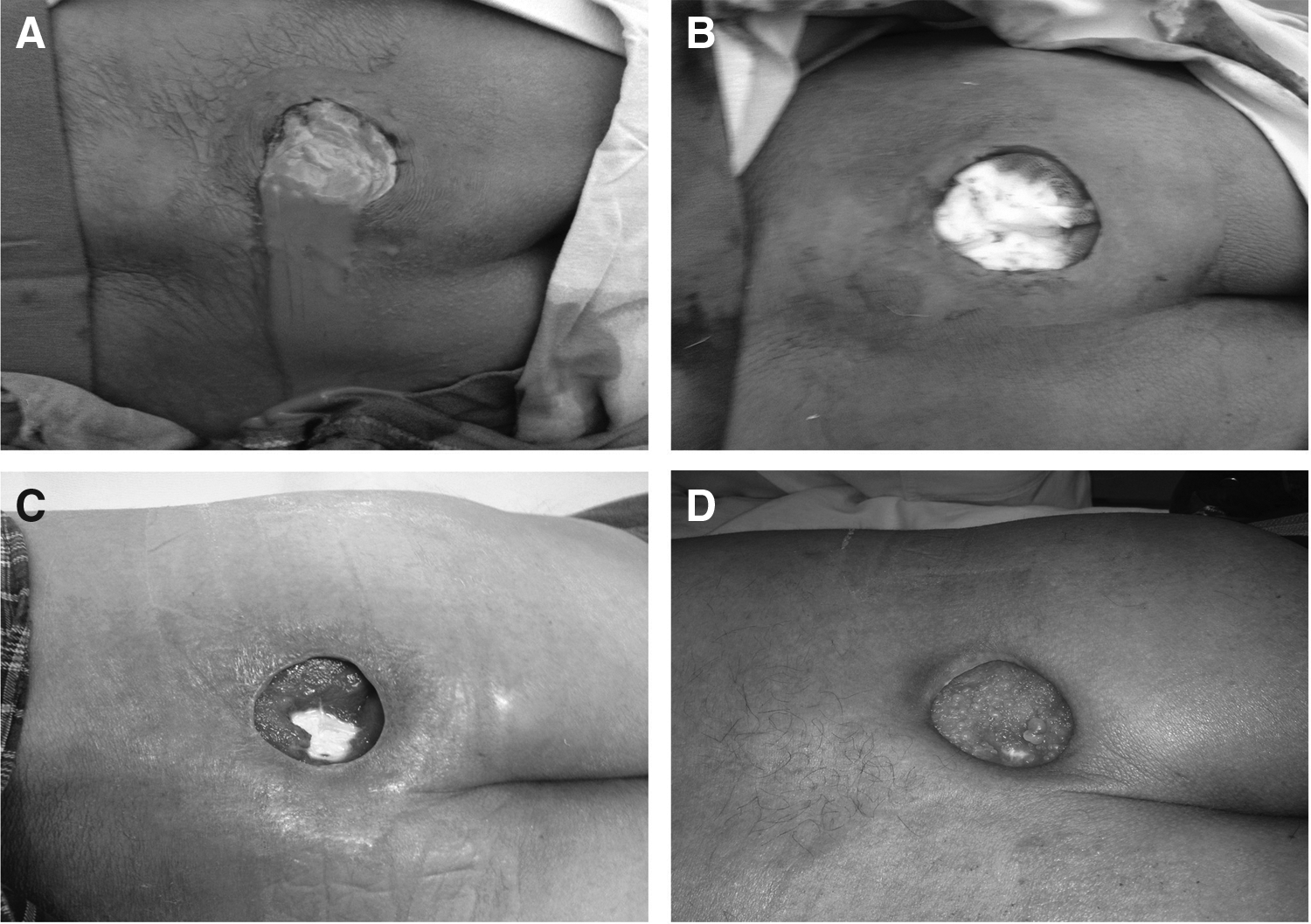
Image depicting resolution of infective process in a patient allocated to the placebo arm after incision and drainage (I&D). (
Although simple cases of cutaneous cellulitis and abscesses are caused by gram-positive pathogens, it is common for physicians to use broad-spectrum antibiotic agents against gram-negative and anaerobic micro-organisms [15–18]. Medical staff must remain aware that exposing patients to unnecessary, lengthy, and unwarranted broad-spectrum antibiotic treatments is unacceptable in the current era of progressive antimicrobial resistance [19–21] as well as the incidence and severity of infection by Clostridium difficile [22,23].
Current guidelines of the American Society of Infectious Diseases (ASID) and the U.S. Centers for Disease Control and Prevention (CDC) state that uncomplicated cutaneous abscesses are amenable to I&D alone, whereas in cases of recurrent or refractory abscesses the presence of methicillin-resistant Staphylococcus aureus (MRSA) should be suspected and treated accordingly [24]. Recent studies, however, reported that the outcomes of SSTIs treated with antibiotic agents were much the same regardless the activity of the prescribed drug against the infecting organism as confirmed by culture/antibiogram [25,26]. When cultures of patients with SSTIs reported the presence of MRSA, all of those infections improved even when β-lactamic antibiotic agents, ineffective against this micro-organism, were administered [6,27]. However, in a trial involving 1,265 patients with a drained cutaneous abscess, Talan et al. [28] found that patients who received trimethoprim-sufamethoxazole (at doses of 320 and 1600 mg, respectively, twice daily, for 7 d) had a higher cure rate than those who received placebo. The researchers also found that many secondary outcomes were better in the trimethoprim-sulfamethoxazole group than in the placebo group, including fewer subsequent surgical drainage procedures, new skin infections, and infections among household members six to eight weeks after the end of the treatment period.
Our study challenges the current recommendations of the Clinical Practice Guidelines of Mexican Institute of Social Security (IMSS-074-08) for the medical management of SSTIs and SSIs. Both guidelines endorse the administration of a variety of oral/intravenous antibiotic agents for such types of infections [29]. The results of this study may well serve for future updates in the aforementioned guidelines.
In this study we sought to determine any possible role of antibiotic agents as adjunct treatment in the management of subcutaneous abscesses. No such a role could be identified. Patients undergoing I&D resolved their infectious process at a similar rate and time whether or not antibiotic agents were prescribed. This was true even in patients with diabetes mellitus and those older than 70 years. We also wanted to determine whether antibiotic agents help decrease pain or accelerate healing by acting synergistically with the immune system. Such benefits were also ruled out according to our results.
We have to recognize that ciprofloxacin was not the most appropriate choice, even though it has activity against gram-positive as well as gram-negative bacteria and one (not the preferred) of their indications is soft tissue infections. As we mentioned in the introduction, emergency department physicians in our hospital often prescribe antibiotic agents and admit patients to the surgical ward for diagnosis of subcutaneous abscess. By doing a little research, we identified ciprofloxacin as one of the antibiotic agents most frequently prescribed by our emergency department colleagues. The reason why we decided to use it in our study was in part to demonstrate that the same incorrectly prescribed antibiotic (ciprofloxacin) is also unnecessary. Regarding the dose used, the recommended therapeutic range of ciprofloxacin is 500–1,500 mg/d. Because we excluded patients with complicated disease or with conditions likely to lead to a complicated outcome (necrotizing fasciitis, Fournier gangrene, diabetic foot, etc.), we considered it appropriate to use the minimum effective dose of the drug. Because evidence does not support routine swabbing for culture in immunocompetent individuals [30], we did not send samples of pus for culture/antibiogram at first I&D and reserved this measure only for those patients who failed to progress satisfactorily. As stated previously, no patient had to be admitted because of failure of initial treatment.
Among the limitations of this study it should be noted that: it was not properly powered and thus no methodologically correct sample of patients was set for representativeness of the population; it was single-blinded only, with the medical consultant who performed follow-up revisions being aware of the arm to which the patient had been allocated after randomization; and it was a single-institution study, so theoretically, the results might not be widely applicable. There is an inherent risk of bias as a result of these drawbacks. The strengths of the study are: it was randomized and placebo-controlled; it was a straightforward intervention, easily applicable in every institution; and its results may lead to a better use of clinical resources and important savings for health care institutions.
Conclusions
According to our results, I&D is the sole procedure required for patients with uncomplicated subcutaneous abscess. Antibiotic agents do not confer any benefit to I&D and, in general, are not warranted unless cellulitis without pus is present. Multi-institutional, properly sized, and well-designed clinical trials are needed to corroborate these results.
Footnotes
Acknowledgments
We declare that this manuscript has neither been published nor being to be published elsewhere. Each author has made important scientific contributions to the manuscript. All authors listed have agreed to submit in present form and declare that there are no conflicts of interests.
Author Disclosure Statement
No competing financial interests exist.