
Abstract
Abstract
Background:
The Trauma Infectious Disease Outcomes Study (TIDOS) cohort follows military personnel with deployment-related injuries in order to evaluate short- and long-term infectious complications. High rates of infectious complications have been observed in more than 30% of injured patients during initial hospitalization. We present data on infectious complications related to combat trauma after the initial period of hospitalization.
Patients and Methods:
Data related to patient care for military personnel injured during combat operations between June 2009 and May 2012 were collected. Follow-up data were captured from interviews with enrolled participants and review of electronic medical records.
Results:
Among 1,006 patients enrolled in the TIDOS cohort with follow-up data, 357 (35%) were diagnosed with one or more infection during their initial hospitalization, of whom 160 (45%) developed a trauma-related infection during follow-up (4.2 infections per 10,000 person-days). Patients with three or more infections during the initial hospitalization had a significantly higher rate of infections during the follow-up period compared with those with only one inpatient infection (incidence rate: 6.6 versus 3.1 per 10,000 days; p < 0.0001). There were 657 enrollees who did not have an infection during initial hospitalization, of whom 158 (24%) developed one during follow-up (incidence rate: 1.6 per 10,000 days). Overall, 318 (32%) enrolled patients developed an infection after hospital discharge (562 unique infections) with skin and soft-tissue infections being predominant (66%) followed by osteomyelitis (16%). Sustaining an amputation or open fracture, having an inpatient infection, and use of anti-pseudomonal penicillin (≥7 d) were independently associated with risk of an extremity wound infection during follow-up, whereas shorter hospitalization (15–30 d) was associated with a reduced risk.
Conclusions:
Combat-injured patients have a high burden of infectious complications that continue long after the initial period of hospitalization with soft-tissue and osteomyelitis being predominant. Further research on the long-term impact and outcomes of combat-associated infection is needed.
I
Patients and Methods
Study population and design
Data from the TIDOS population specific to U.S. military personnel with injuries sustained during combat between June 1, 2009 and May 31, 2012 were evaluated. Full details on the TIDOS population and study design are available in Tribble et al. [16]. In brief, patients were eligible for inclusion in the cohort if they were active-duty personnel or DoD beneficiaries, at least 18 years of age, sustained a combat-related injury during the study period requiring medical evacuation to Landstuhl Regional Medical Center (LRMC) in Germany before transfer to a participating U.S. hospital, and were able to provide informed consent (or surrogate consent through a legally authorized representative). The participating U.S. hospitals were Walter Reed Army Medical Center and National Naval Medical Center in the National Capital Region (Walter Reed National Military Medical Center after September 2011) and Brooke Army Medical Center in San Antonio, Texas (San Antonio Military Medical Center [SAMMC] after September 2011). The study was approved by the Infectious Disease Institutional Review Board of the Uniformed Services University of the Health Sciences in Bethesda, Maryland.
Recruitment occurred during the initial trauma hospitalization period at participating U.S. hospitals after clinical providers and/or nursing staff had determined that a patient was interested in speaking with study staff. Patients who enrolled and consented to follow-up were contacted at specific intervals after their initial discharge (i.e., 1 mo, 3 mo, 6 mo, 12 mo, 18 mo, 24 mo, and then annually for a minimum of 5 y after discharge). Methods used to obtain follow-up information included telephone interviews with participants. For all enrolled patients, including those not reached for interviews, follow-up data were also obtained through review of the DoD's electronic medical record (EMR).
Information on trauma history, injury patterns, and surgical care was obtained from the U.S. Department of Defense Trauma Registry (DoDTR) [17]. Shock index was documented at the initial support hospital and is defined as the heart rate divided by systolic blood pressure. Traumatic amputation data were collected from LRMC prior to admission in the United States. Fracture information was collected from all levels of care and digit-only fractures were excluded from the analysis. Injuries were categorized using Injury Severity Score (ISS), which is an overall measure calculated for each patient based on the top three maximum Abbreviated Injury Scale anatomic region values [18,19]. Blood transfusion data within the first 24 hours of injury was missing for many subjects; however, the missing data were not randomly distributed. Patients with missing blood data were characterized by lower injury severity scores and shock indices. Furthermore, the majority of patients with missing blood data did not sustain a traumatic amputation and were not admitted to the LRMC intensive care unit.
Data on inpatient infectious disease events were collected from the TIDOS infectious disease module [16]. Infections during the inpatient hospitalization were identified using a combination of clinical findings and laboratory test results, and classified in accordance with standardized definitions from the National Healthcare Safety Network (NHSN). In the absence of meeting a priori criteria, an infectious disease event was included in the analysis if there was a clinical diagnosis associated with directed antimicrobial treatment that was continued for at least five days for SSTIs and 21 days for osteomyelitis (unless surgical cure performed with amputation). Infections were excluded if an alternate diagnosis was documented along with discontinuation of antimicrobial therapy [16,20].
The NHSN-based infection syndromes were utilized to capture infection events documented in the DoD EMR during cohort follow-up. In addition, injury narratives were reviewed comprehensively to determine if site-specific infections were likely related to the initial trauma. Specifically, SSTIs and osteomyelitis required evidence of severe injury to the affected extremity. Urinary tract infections were counted during follow-up if the patient had a traumatic injury to the pelvic/genital region or a severe head or spinal injury leading to use of a catheter. Follow-up intra-thoracic infections were included if the patient had a penetrating injury to the thoracic region (e.g., pneumothorax) or had a severe head injury resulting in use of mechanical ventilation. Last, intra-abdominal infections during follow-up required a penetrating injury to the abdominal region.
Statistical analysis
Characteristics of patients who did and did not enroll in TIDOS, as well as who did and did not provide an interview in the first year of follow-up, were compared using χ2 testing for categorical indicators and two-sample t-test for continuous characteristics. Predictive factors for TIDOS enrollment were examined in univariable and multivariable logistic regression models. Risk factors for the development of CEWIs were assessed using log binomial regression to calculate relative risk. Covariates with a p value ≤0.2 from univariable models were considered in the initial full multivariable models. Covariates that might be sources of confounding were examined for interactions (e.g., amputation, shock index, first 24-h blood transfusion, and ISS) and first hospitalization characteristics (e.g., hospital admission unit) were examined in the multivariable models. Stepwise, backward, and forward model selection strategies were used to choose the final predictive factor and relative risk factor models for TIDOS enrollment and development of CEWIs, respectively.
Results
Study population
Overall, 3,304 military personnel were admitted to LRMC between June 2009 and May 2012 with combat-related injuries. Among this population, 3,149 were transferred to a hospital in the United States, of whom 1,826 (58%) were admitted to one of the TIDOS-participating hospitals and eligible for enrollment in the cohort. A total of 1,014 (56%) patients enrolled in the TIDOS cohort, of whom 652 (64%) and 362 (36%) were admitted to hospitals in the National Capital Region and SAMMC, respectively.
The predominant mechanism of injury was blast regardless of enrollment status (Table 1). Although patients who enrolled in TIDOS had a higher proportion of traumatic amputations (excluding digits; p = 0.032), the patients who did not enroll in the cohort had significantly higher ISS (p = 0.017). Furthermore, a greater proportion of patients who did not enroll in TIDOS were admitted to the intensive care unit at LRMC (p = 0.003) and required mechanical ventilation (p < 0.001).
Percentages are based upon total number minus missing. Missing values are not included in p value calculation.
The operational theater is missing for 20 TIDOS enrollees.
Other non-blast mechanisms include burns, motor vehicle crashes, and falls. Mechanism of injury information missing for 19 enrollees.
The score is missing for 20 subjects (19 enrolled and 1 who did not enroll).
Amputation data missing from 19 TIDOS enrollees and 2 patients not enrolled in TIDOS.
Blood transfusion data are missing for 465 TIDOS enrollees and 394 patients who did not enroll in TIDOS.
Admission unit data missing for one TIDOS enrollee and three patients who did not enroll.
Mechanical ventilation data missing for one TIDOS enrollee and two patients who did not enroll.
TIDOS = Trauma Infectious Disease Outcomes Study; IQR = interquartile range; IED = improvised explosive device; LRMC = Landstuhl Regional Medical Center; MDRO = multi-drug–resistant organisms.
Independent predictive factors related to an increased likelihood of enrollment were lower extremity severity scores classified as moderate, serious, or critical; greater number of operating room visits after injury; and SAMMC admission (Table 2). Variables independently associated with a reduced likelihood of enrolling in the cohort were branch of service (U.S. Marine Corps, Navy, and other service compared with Army), being on mechanical ventilation at U.S. hospitals, and having an ISS ≥16.
Variables examined in univariable model but not shown include gender, age, military rank, operational theater, injury severity measures, fractures, blood transfusion volume, and duration of hospitalization.
Variables entered into initial multivariable model but not retained in final model include age, operational theater, mechanism of injury, traumatic amputation, shock index, admission unit at U.S. hospitals, colonization with MDRO at U.S. hospital,, and duration of hospitalization.
Values for shock index determined by lowest quartile, interquartile range, and highest quartile
CI = confidence interval; IED = improvised explosive device; MDRO = multi-drug–resistant organisms.
Cohort follow-up
Based on the number of enrollees, 4,024 interviews were predicted for the first 12 months of follow-up; however, the actual number of interviews was 2,446 (61%). Overall, 903 (89%) enrolled patients provided at least one follow-up interview during the first year, whereas the remaining 111 (11%) were never reached for interview. Seven enrollees withdrew from the cohort prior to follow-up data capture and one enrollee did not provide data until the three-year follow-up interval. Among the subjects who did and did not provide interviews in the first year, there was no difference in their severity or pattern of injuries or occurrence of one or more infections during their initial hospitalization (data not shown). The proportion of enrolled participants that provided incremental follow-up interviews remained constant for the first year (ranging from 59% to 64%); however, starting with the 18-month interviews, the proportion of subjects who were interviewed declined to 57% and then to 44% for the two-year interview. All enrollees had EMR data collection during the study period. A total of 12 enrollees withdrew from the cohort (1%) in this two-year period.
Trauma-related infection rates
Among the 1,006 enrolled patients with data available for at least two years of follow-up (up to six years), 357 (35%) experienced at least one trauma-related infection during their initial hospitalization. Specifically, 158 (16%) had one infection, 84 (8%) had two infections, and 115 (11%) had three or more infections. The most common types of inpatient infections were CEWIs (e.g., SSTIs and osteomyelitis), which were diagnosed in 237 patients (24% of enrolled patients; 66% of enrolled patients with one or more infection during initial hospitalization).
Of these 357 patients, 160 (45%) experienced a new trauma-related infection during the follow-up period, resulting in an incidence rate of 4.2 per 10,000 person-days (95% confidence interval [CI]: 3.6–4.9). The incidence of infections observed in the follow-up period increased based on the number of infections incurred during the initial hospitalization period. Specifically, 37% of patients with one inpatient infection developed an infection after their initial discharge (incidence rate of 3.1; 95% CI: 2.3–3.9). In comparison, 44% of patients with two inpatient infections developed at least one infection during follow-up (incidence rate of 4.0; 95% CI: 2.7–5.3), whereas it was 57% of patients with at least three inpatient infections (incidence rate of 6.6; 95% CI: 5.0–8.2). When patients with at least three inpatient infections were compared with those with only one inpatient infection, the incidence density ratio was 2.4 (95% CI: 1.8–3.1; p < 0.0001). Among the 657 patients who did not experience any infections during their inpatient period, 158 (24%) developed an infection after discharge for an incidence rate of 1.6 (95% CI: 1.4–1.9). When patients with at least one inpatient infection were compared to those with no inpatient infection, the incident density ratio was 3.3 (95% CI: 2.8–3.9; p < 0.0001).
Overall, 318 (32%) patients had at least one trauma-related infection event after their initial discharge. Of these patients, 183 (58%) had only one infection, 76 (24%) had two infections, 32 (10%) had three infections, and 27 (8%) had four or more infections. The median number of days after their initial hospitalization to the occurrence of any post-discharge infection was 133 (range, 1–1,699). The total days of patient observation was 1,342,089. An infection incidence rate of 0.2 first infections per 1000-person-days (95% CI: 0.2–0.3) was observed. Among patients with infections (135 with multiple infections), the majority were diagnosed with SSTIs (242 patients, 76%), osteomyelitis (74 patients, 23%), and urinary tract infections (35 patients; 11%). For patients with available information, 23% were hospitalized and 40% required surgery as a result of the infection.
On a per infection event basis, 562 unique trauma-related infections occurred during the follow-up period after the initial discharge from the U.S. hospitals. The SSTI events were most common, accounting for 370 (66%), followed by 88 (16%) osteomyelitis, 47 (8%) urinary tract infections, 19 (3%) intra-cranial infections (e.g., sinusitis), 17 (3%) intra-thoracic infections (e.g., pneumonia and tracheobronchitis), 15 (3%) blood stream infections, and 6 (1%) intra-abdominal infections. The median number of days after discharge to development of an infection ranged from 10 weeks with intra-abdominal infections to 36 weeks with intra-cranial infections (Fig. 1). Osteomyelitis and SSTIs occurred a median of 107 days (interquartile range: 45–245) and 126 days (interquartile range: 37–287), respectively, after discharge.
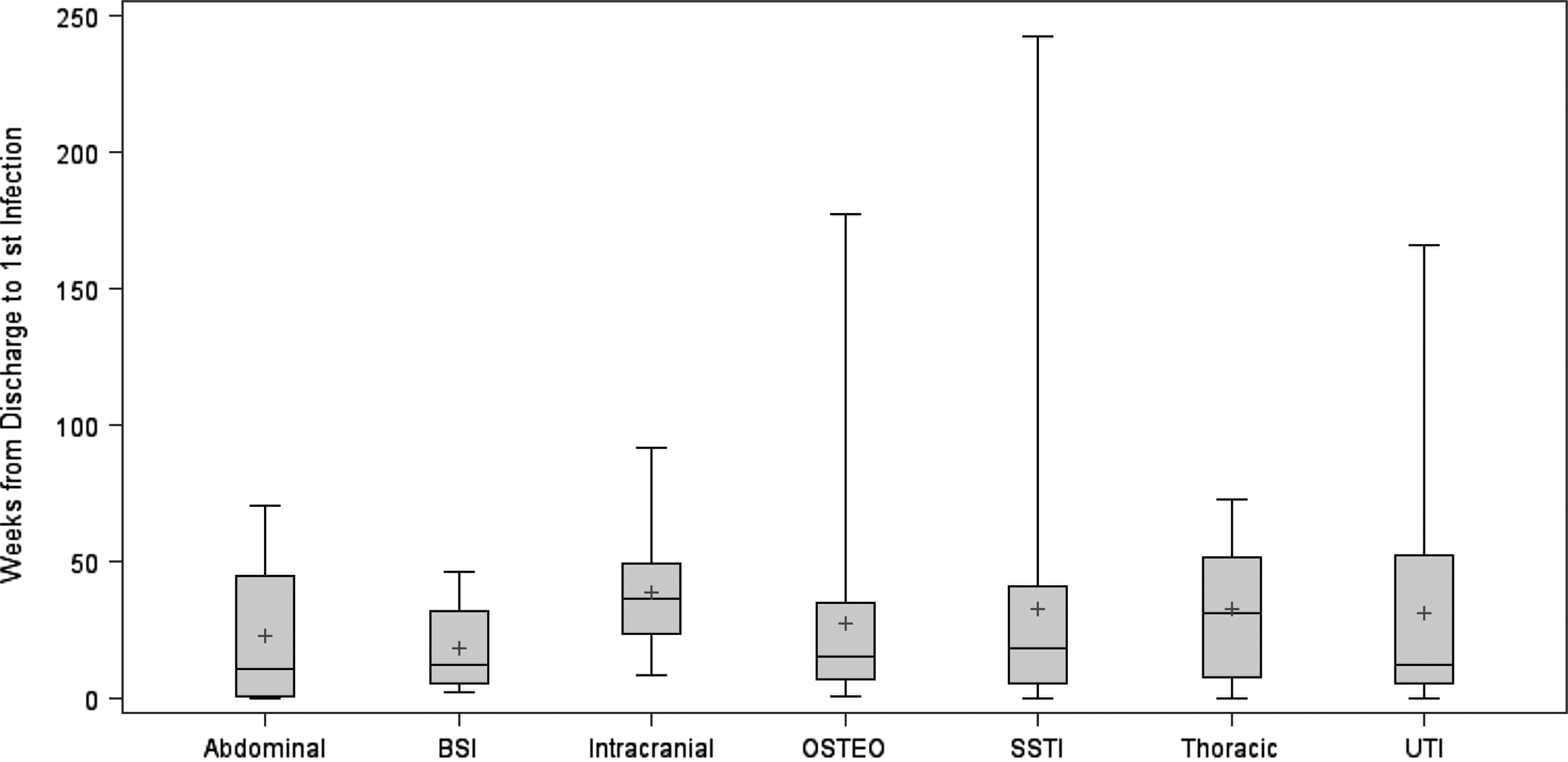
Time from initial trauma hospital discharge to first infection. Only the first infection per patient is considered and data are presented on a per patient basis. Diamond inside of the interquartile range box represents the mean weeks to first new infection, and the line represents the median weeks to first infection. BSI = blood stream infection (n = 11); Osteo = osteomyelitis (n = 74); intra-abdominal infections (n = 4); UTI = urinary tract infections (n = 35); SSTI = skin and soft-tissue infections (n = 242); intra-cranial infections (n = 15); and intra-thoracic infections (n = 16).
The predominant organism isolated from patients with infections diagnosed during follow-up was Staphylococcus aureus, which was linked to 39% of osteomyelitis and 26% of SSTI events, of which 24% and 31% were methicillin-resistant Staphylococcus aureus, respectively. Coagulase-negative Staphylococcus spp. was also recovered from both osteomyelitis (20%) and SSTIs (5%). Escherichia coli was linked with six (7%) osteomyelitis events (17% multi-drug–resistant) and 10 (3%) SSTIs (10% multi-drug–resistant). Pseudomonas aeruginosa was recovered from 7 (8%) osteomyelitis and 13 (4%) SSTI events with one isolate from an osteomyelitis event being multi-drug–resistant. Enterobacter aerogenes was only isolated from one (multi-drug–resistant) osteomyelitis and one (susceptible) SSTI event. Last, Acinetobacter baumannii was isolated from one (susceptible) SSTI event, but was not recovered from any osteomyelitis cases.
Combat-related open extremity wound infections
Among the 318 patients with an infection observed during follow-up, 234 (74%) had a CEWI (i.e., SSTIs and osteomyelitis). Overall, there were a total of 212 (26%) incident CEWIs observed during follow-up among the 826 enrolled patients with combat-related open extremity wounds (34% and 22% among patients with and without CEWIs during their initial hospitalization, respectively; Fig. 2). Moreover, 19% of patients with a CEWI during their initial hospitalization experienced a recurrent CEWI during follow-up (i.e., infection at same side and site as their initial infection). In particular, 6% of the 826 enrolled patients developed an incident osteomyelitis during the follow-up.
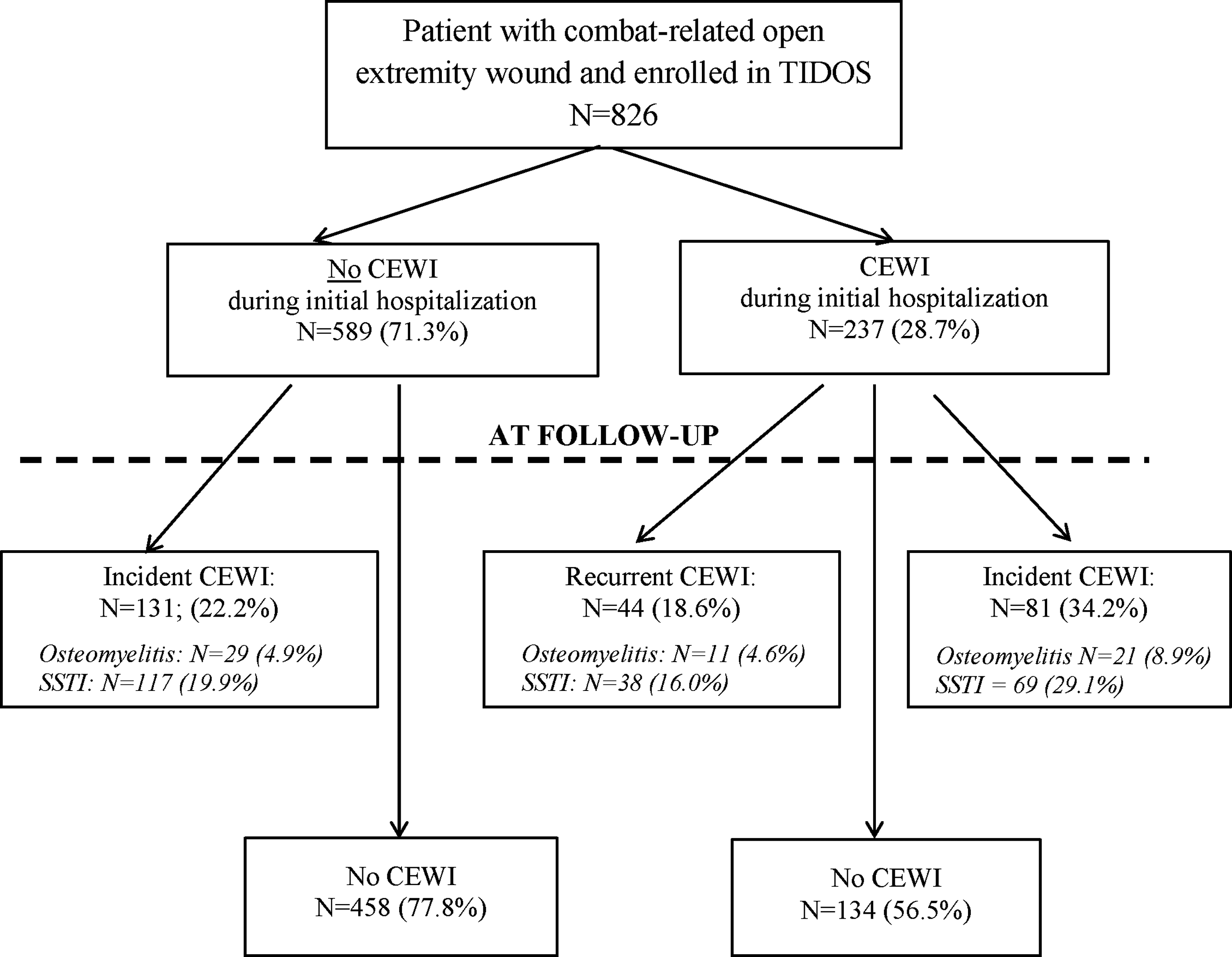
Flow chart for the occurrence of combat-related open extremity wound infections (CEWI), specifically osteomyelitis and skin and soft-tissue infections (SSTI), during the inpatient period and following initial discharge. Among patients that had a CEWI during their initial hospitalization, recurrent CEWIs are defined by the infection occurring on the same site/side, while incident CEWIs occur on a different site/side. Patients may have both an SSTI and osteomyelitis, as well as both an incident and recurrent CEWI, so numbers may add to more than the indicated totals. The total number of patients with a CEWI during initial hospitalization who had a CEWI during follow-up is 103.
Improvised explosive device blast mechanism of injury, sustaining an amputation or open fracture, injury severity, blood transfused within 24 hours post-injury, occurrence of an inpatient infection, admission to the intensive care unit, use of vancomycin or anti-pseudomonal penicillin for at least seven days during inpatient hospitalization, being discharged with hardware after the initial hospitalization, and duration of initial hospitalization were associated with risk of developing a CEWI in the follow-up period in the univariable model (Table 3). After assessment in the multivariable model, variables associated independently with an increased risk of developing CEWIs after the initial trauma hospitalization were sustaining an amputation or open fracture, having an infection during initial hospitalization (CEWI or other type), and receipt of anti-pseudomonal penicillin for at least seven days during the initial hospitalization period (Table 3). Duration of initial hospitalization of 15 to 30 days was associated with a reduced risk of developing a CEWI.
Population is restricted to patients who sustained combat-related open extremity wounds (n = 826)
Patients with multiple types of injury patterns were classified by most severe injury.
CEWI = combat-related open extremity wound infections; CI = confidence interval; IED = improvised explosive device; IQR = interquartile range; LRMC = Landstuhl Regional Medical Center; MDRO = multi-drug–resistant organisms.
Discussion
Infectious complications continue to impact wounded military personnel long after their initial period of hospitalization; however, there is limited information on the longitudinal follow-up of combat casualties. As reported from the TIDOS project [5], high rates of early-onset infections occur during the inpatient period (35%). This report further documents the substantial high rates of delayed trauma-related infections with onset after initial hospital discharge (32%), demonstrating an additive burden of infectious complications with a prolonged duration. Our analysis is restricted to direct infectious complications at the site of battlefield injuries. These findings likely represent only one aspect of the infection burden as these patients are also at risk for health-care–associated infections (e.g., urinary tract infections and pneumonia), resulting from invasive devices and other treatments (e.g., catheters and mechanical ventilation).
The TIDOS cohort is unique in the amount of detailed information captured prospectively from this battlefield trauma population regarding injury characteristics, inpatient treatment, and microbiology. Patients admitted to TIDOS-participating U.S. hospitals from the U.S. military hospital in Germany (LRMC) were more severely injured than those who transferred to non-participating hospitals. Specifically, patients were more likely to have been injured via an explosive blast mechanism and have a higher ISS, so patients eligible to enroll in the cohort cannot be generalized broadly to all combat casualties from the recent wars [5]. In addition, there are notable differences between patients who did or did not choose to enroll; however, cohort enrollment was successful in more than 50%. Enrolled individuals, overall, had moderately severe injuries compared with those who did not enroll; however, the cohort is well represented for severe injuries (for example ISS ≥16 in 38%, mechanical ventilation required in 34%).
As with infections during the initial trauma hospitalization, CEWIs represent the most common type of delayed infection among patients with battlefield trauma. Factors found to increase the risk or be protective against the development of CEWIs after discharge may support clinical decisions regarding treatment during both the initial hospitalization and follow-up, particularly among complex blast injured patients. The finding of the open fracture and amputation injury pattern being a significant predictor for the development of a CEWI during follow-up is not unexpected as open fractures are recognized as a risk factor for infection and often result in infection recurrence or relapse [10,14,21,22]. The association of receipt of anti-pseudomonal penicillin for at least seven days is likely a surrogate for injury severity (78% of patients who received antipseudomonal penicillin had an ISS ≥25; p < 0.0001). Moreover, the shorter duration of hospitalization (15–30 d) associated with a reduced risk of infection during follow-up. A longer period of hospitalization is presumably the result of a patient being more severely injured or experiencing complications from the trauma, resulting in greater morbidity and requirement of additional surgical treatment, antimicrobial therapy, or both. An extended hospitalization also provides greater opportunity for acquisition of bacterial organisms, including multi-drug–resistant organisms. Last, the impact of inpatient CEWIs on long-term morbidity and burden of disease is apparent: 43% of patients in our cohort who had a CEWI during their initial hospitalization developed an SSTI or osteomyelitis during follow-up (19% had recurrent infections and 34% had incident infections). Specifically, the occurrence of an inpatient CEWI was determined to be an independent predictor for risk of developing a delayed CEWI during follow-up (relative risk ratio: 2.25; 95% CI: 1.23–4.13). Nevertheless, it is also important to note that 22% of patients with an extremity wound who did not have an early onset CEWI during their initial hospitalization, still developed a delayed CEWI during follow-up (Fig. 2). Furthermore, 36% of the patients who were diagnosed with a delayed CEWI had a non-extremity wound infection during their initial hospitalization, which was also found to be an independent predictor of CEWI risk (relative risk ratio: 2.35; 95% CI: 1.30–4.27).
Although not as common as SSTIs, 7.4% of subjects with an open extremity wound developed a delayed incident or recurrent osteomyelitis during follow-up (Fig. 2). In a prior analysis of military personnel with combat-related injuries sustained in Iraq and Afghanistan, patients with osteomyelitis were followed for a period up to 36 months and 25% (28/110) developed a relapsed infection [10], which is higher than our proportion of 6% of post-discharge osteomyelitis recurrence (Fig. 2). The analysis also noted that the microbiology of the initial wound infections was different compared with the relapsed infections. Specifically, the initial wounds were commonly infected with gram-negative bacilli, whereas relapsed wounds more frequently recovered gram-positive cocci [10]. Similar to what has been reported previously [8], our analysis found that Staphylococcus aureus was the predominant isolated organism linked with post-discharge delayed infections (39% of osteomyelitis and 26% SSTIs).
Previous reports of trauma-related infection rates in selected populations during follow-up have also documented delayed impacts, such as recurrent/relapsed infections, new-incident infections, non-union of fractures, and late amputations. In one analysis of combat casualties from Iraq with lower extremity amputations, it was found that 16% required late revision surgery more than two months after definitive amputation closure and 2% of extremities required additional surgical procedures because of wound breakdown a median of 132 days after wound closure [6]. In another analysis, 16 combat casualties were evaluated at a military limb preservation clinic a median of 13 months post-injury. Ten patients required amputations, of whom six had chronic SSTI and/or osteomyelitis [23]. Among British military personnel with open femur fractures sustained in Iraq, 8.5% required surgical revision because of infections a median of 10 months after injury [9], whereas 31% of U.S. combat casualties with open proximal femoral fractures developed infectious complications requiring re-operations [13]. A similar high burden of disease was also observed on our analysis, with 23% of the 318 enrollees with a post-discharge infection requiring hospitalization and 40% needing surgery. Comparable results have also been reported in civilian patients with open bone fractures. In particular, deep infection or chronic osteomyelitis is also a morbid condition among these patients that generally results in non-union and requires multiple operative procedures, including late or secondary amputations [24–31].
There are limitations related to this analysis that should be considered. In particular, precise information related to early trauma management is incomplete or lacking for many of the subjects. Because early surgical and medical management is a critical component of trauma care, further assessment of the impact of these factors on delayed CEWI risk is warranted. Another limitation is the decline in the number of enrollees who provided follow-up interviews after one year. Nevertheless, it is important to note that only a fraction of the follow-up information is obtained through personal communications with the enrollees, whereas all subjects in the cohort had interval reviews of the EMR. An advantage of the EMR is that comprehensive information is available for medical encounters, whereas participants may remember having an infection, but do not recall pertinent details. Therefore, between personal communications and EMR reviews, the TIDOS project has maintained nearly complete follow-up with all of the enrollees.
Overall, the results of this unique cohort demonstrate that the morbidity from trauma-related infections continues past the initial hospitalization up to years later in the form of new or recurrent delayed infections, hospitalization, and further surgical procedures. The burden of disease after the initial hospitalization is apparent with an incidence rate of 4.2 infections per 10,000 person-days. Additional examination of outcomes related to CEWIs and other specific injury patterns is warranted, along with a comprehensive evaluation of health economics related to surgical and medical care received in order to provide support to optimize infection management. Furthermore, as part of our collaboration with the VA, data collected through abstraction of VA medical records are being analyzed to capture further detail regarding delayed infections in the follow-up period, as well as providing information related to mental health and social support among wounded veterans.
Footnotes
Acknowledgments
We are indebted to the Infectious Disease Clinical Research Program TIDOS study team of clinical coordinators, microbiology technicians, data managers, clinical site managers, and administrative support personnel for their tireless hours to ensure the success of this project.
This work (IDCRP-024) was supported by the Infectious Disease Clinical Research Program, a Department of Defense program executed through the Uniformed Services University of the Health Sciences, Department of Preventive Medicine and Biostatistics. This project has been funded by the National Institute of Allergy and Infectious Diseases, National Institute of Health (Inter-Agency Agreement Y1-AI-5072), and the Department of the Navy under the Wounded, Ill, and Injured Program (HU001-10-1-0014).
The views expressed are those of the authors and do not reflect the official views of the Uniformed Services University of the Health Sciences, Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., National Institutes of Health or the Department of Health and Human Services, Brooke Army Medical Center, Walter Reed National Military Medical Center, Landstuhl Regional Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of Defense or the Departments of the Army, Navy or Air Force. Mention of trade names, commercial products, or organization does not imply endorsement by the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.