
Abstract
Abstract
Background:
The purpose of this study was to establish compliance with guidelines published by the American College of Obstetricians and Gynecologists (ACOG) regarding prophylactic antibiotic use in gynecologic surgery at our institution, and define areas of improvement to promote antibiotic stewardship.
Patients and Methods:
This was a retrospective cohort study at a single, large tertiary care and teaching hospital in Kansas. Patients who underwent inpatient or outpatient gynecologic surgery during 2013 were included. Based on published guidelines for prophylactic antibiotic agents for gynecologic surgery by ACOG, procedures were classified as antibiotic-indicated or antibiotic-not-indicated. Chi-square and Fisher exact test analysis were used to identify factors associated with antibiotic use.
Results:
Of the 1,735 cases eligible for inclusion, 1,045 (60.2%) had antibiotic agents recommended per guidelines, and appropriate antibiotic agents were given in 1,031 (98.7%) of those cases. In 690 (39.8%) cases, prophylactic antibiotics were either not recommended or the guidelines are not well defined. Of the 690 cases without indication for antibiotic agents, 394 (57.1%) received prophylactic antibiotic agents. Agreement with guidelines varied substantially based on patient age, race, insurance status, area of residence, and if the procedure was a resident case (p < 0.05). Myomectomy, laparoscopy, and ectopic pregnancy procedures received antibiotic agents against recommendations 96.3%, 75.6%, and 45.5% of the time, respectively.
Conclusions:
Peri-operative antibiotics are often administered inappropriately to women undergoing gynecologic surgeries for which published guidelines are not well defined. Future studies need to identify strategies to reduce antibiotic use in surgical procedures unlikely to benefit from prophylaxis.
T
Antibiotic prophylaxis is not recommended for laparoscopy, because it is classified as a clean procedure and evidence from a single randomized control study failed to demonstrate a reduction in SSIs [3,12]. Laparoscopic procedures for sterilization or ectopic pregnancies fall within this recommendation. Prophylaxis is also generally not recommended for hysteroscopy, hysterosalpingography, or chromotubation. However, there are situational conditions in which prophylaxis is reasonable, mainly in the setting of a history of pelvic inflammatory disease or dilated fallopian tubes [13]. Furthermore, there is no prospective evidence for antibiotic prophylaxis in uro-gynecologic procedures, such as mid-urethral slings or vaginal colporrhaphy [3,13]. These procedures are generally considered clean-contaminated and would therefore receive antibiotic prophylaxis based on wound classification [3]. In general, guidelines for non-hysterectomy gynecologic surgery are more nuanced, have not been as well defined, and are understudied compared with hysterectomy procedures.
The percentage of women undergoing hysterectomy who receive prophylactic antibiotics has been proposed and adopted as a performance measure [3,13,14]. Whereas there are some data on actual adherence to recommendations for antibiotic prophylaxis in women undergoing hysterectomy, little is known on compliance with peri-operative antibiotic use with non-hysterectomy gynecologic procedures. It is not clear if published guidelines on antibiotic prophylaxis for non-hysterectomy gynecologic procedures have been adopted widely or are being adhered to.
The only large, population-based analysis of peri-operative antibiotic use in gynecologic surgery demonstrated a trend in un-indicated use of antibiotic agents for non-hysterectomy procedures [15]. The study analyzed the Perspective database and used surrogate markers to estimate antibiotic prophylaxis for hysterectomy (all routes) and a few other non-hysterectomy gynecologic procedures. Wright et al. [15] reported peri-operative antibiotic agents were administered in 40.2% of women undergoing a gynecologic procedure without an indication for prophylaxis. A review published in 2012 highlighted the paucity of data investigating antibiotic prophylaxis in non-hysterectomy gynecologic surgeries [16]. In January 2017, a study by Joyce et al. [17] reported inappropriate prophylactic antibiotic use in gynecologic procedures was as high as 54% (175 of 326 cases reviewed). However, their study only reviewed gynecologic surgeries for which antibiotic agents were not recommended, and the authors grouped gynecologic procedures using procedure codes into three main categories: laparoscopic procedure, trans-cervical procedures, and open procedures [17]. We are unaware of any other studies examining prophylactic antibiotic use in gynecologic surgeries.
The current study aimed to assess the utilization of peri-operative antibiotic prophylaxis in all gynecologic surgeries performed at a tertiary care hospital, with an emphasis on non-hysterectomy procedures. We report a quality initiative aimed to define areas of improvement for proper antibiotic use for all gynecologic surgery performed at a single institution. We hypothesized that compliance with published guideline-based recommendations was poor for non-hysterectomy surgical procedures. We report suggestions on how potentially to improve peri-operative antibiotic utilization while maintaining adherence to published guidelines.
Patients and Methods
A retrospective cohort study was performed of women who underwent inpatient or outpatient gynecologic procedure from January 1, 2013 through December 31, 2013 at a single teaching hospital in Wichita, Kansas. Exclusion criteria included non-gynecologic procedures performed by gynecologists and gynecologic procedures performed by non-gynecologic surgeons, women less than 18 years of age, and incomplete medical records. A local Institutional Review Board approved the study.
The institution maintains a surgical database that captures demographic and surgical variables. Operating room staff entered data during each case after verifying diagnosis and procedures with the surgeon. Variables included age, date of surgery, insurance status, primary diagnosis, post-operative diagnosis, procedure, operation start time, operation finish time, primary surgeon, secondary surgeon, elective versus non-elective procedure, and zip code. The remaining variables were collected through chart review, including: type of case (resident physician, private clinic) date of admission, date of discharge, race/ethnicity, body mass index (BMI), estimated blood loss (EBL), methicillin-resistant Staphylococcus aureus (MRSA) history, allergies, type of antibiotic agents administered prophylactically, dose and time of administration of antibiotic agents, and emergency department visit or re-admission within 30 days of discharge.
Variables were further collapsed into fewer categories to facilitate the data analysis including type of procedure (hysterectomy, laparoscopy, hysteroscopy, sterilization, uro-gynecologic, general laparotomy, cervical procedures, vulvar/vaginal, gynecologic oncology laparotomy, myomectomy, ectopic pregnancy, other), EBL (less than 500 mL, greater than 500 mL), length of procedure (< 60 min, 60–179 min, >180 min), length of hospital stay (< 2 d, 2 or more days). Patients who tested positive for the Clostridium difficile toxin were identified in the institutional infectious disease registry. The institution protocol for testing Clostridium difficile is fecal samples initially screened by rapid polymerase chain reaction testing. If the patient screened positive, the specific toxin testing is performed.
The principal investigator and senior author reviewed all gynecologic procedures performed at the institution and determined whether antibiotic prophylaxis were recommended based on published guidelines (Supplementary Table S1; see online supplementary material at http://www.liebertpub.com/sur). Before data were collected, procedures were classified as antibiotic-indicated or antibiotics-not-indicated according to published practice guidelines for prophylactic antibiotic use for gynecologic surgery by ACOG [3], similar to Wright et al. [15]. Antibiotic-indicated procedures were operations in which antibiotic agents were recommended routinely and antibiotic-not-indicated procedures were operations for which antibiotics were not recommended routinely by the aforementioned guidelines.
Data were collected and managed using Microsoft Excel (Microsoft, Redmond, WA). All statistical analyses were conducted using the SAS software for Windows, version 9.3 (SAS Institute, Cary, NC). Descriptive statistics were presented as frequencies and proportions for categorical variables. Chi-square analyses were conducted to identify the associations between patient characteristics and the administration of antibiotic prophylaxis for procedures for which they were recommended and not recommended, respectively. Fisher exact test was used if the expected cell count was less than 5. All statistical analyses were two-sided. P value <0.05 was deemed statistically significant.
Results
A total of 1,779 women underwent gynecologic surgical procedures during the study period. Of these, 1,735 cases were eligible for inclusion in the analysis and were stratified into two cohorts based on guidelines suggesting the use or non-use of prophylactic antibiotic agents (Fig. 1). The first cohort included 1,045 (60.2%) cases in which antibiotic prophylaxis was recommended according to ACOG guidelines. The second cohort included 690 (39.8%) cases in which antibiotics were either not recommended or the guidelines are not well defined.
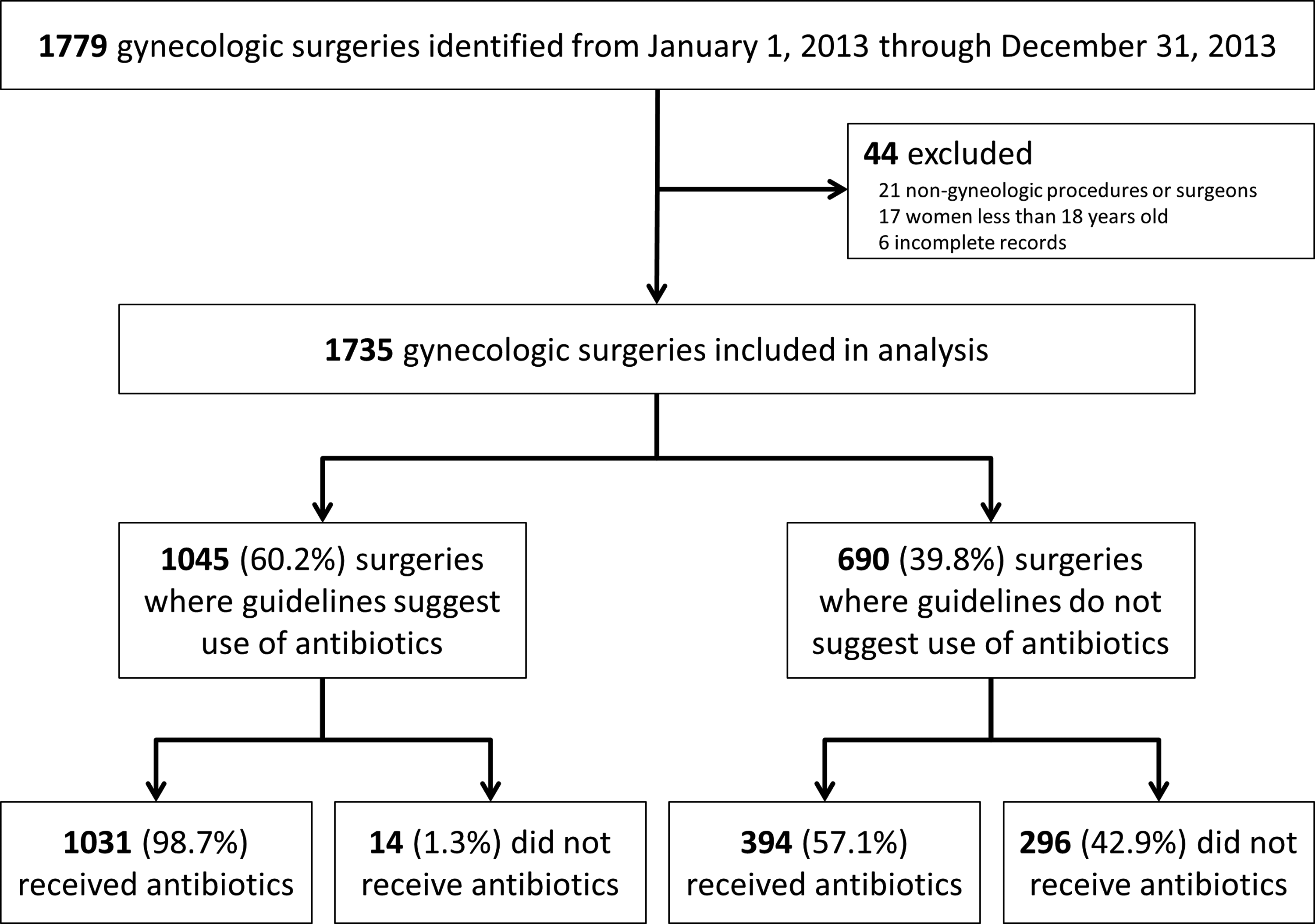
Flow diagram showing patients included in the study and prophylactic antibiotic use according to published guidelines.
For the first cohort (n = 1,045) in which antibiotic agents were recommended, 1,031 (98.7%) received the appropriate, guideline-based antibiotic and 14 (1.3%) received no prophylaxis when indicated. Among the second cohort (n = 690) who underwent a procedure in which guidelines were not recommended explicitly, antibiotic agents were administered in 394 (57.1%) of the cases and withheld in 296 (42.9%) of the cases.
The characteristics of the study sample (n = 1,735) are displayed in Table 1. The majority of women were white (80.5%) with commercial insurance (62.7%) and lived locally (67.8%). Hysterectomy (n = 891; 51.4%) was the most common surgical procedure performed, followed by laparoscopy (n = 234; 13.5%). Overall 82.1% (n = 1,425) of gynecologic surgeries received a prophylactic antibiotic. The vast majority of procedures had an EBL less than 500 (n = 1,609; 92.7%), was shorter than 180 minutes (n = 1,529; 88.1%), and had a hospital length of stay less than 2 days (n = 1,420; 81.8%).
Patients identified in the urban group included Sedgwick and all immediately adjacent surrounding county zip codes. All other zip codes were included in the rural group.
D&C = dilation and curettage.
Table 2 illustrates antibiotic use among women for whom antibiotic agents are recommended according to ACOG guidelines. Prophylaxis for hysterectomy was compliant in 99.1% of cases. In contrast, antibiotic prophylaxis for vulvar/vaginal procedures was administered in only 86.7% of cases (p < 0.001).
Patients identified in the urban group included Sedgwick and all immediately adjacent surrounding county zip codes. All other zip codes were included in the rural group.
Table 3 displays antibiotic prophylaxis in gynecologic surgery for which antibiotics are not recommended or are poorly defined. Age, race/ethnicity, insurance status, area of residence, and if the surgery was a resident physician case all had observations that differed from expectations (p < 0.05). White women received antibiotic agents when not indicated in 60% of cases, compared with 46.6% and 38.7% of black and Hispanic women, respectively. Myomectomy, laparoscopy, and ectopic pregnancy procedures received antibiotic agents inappropriately 96.3%, 75.6%, and 45.5% of the time, respectively. Antibiotic agents were administered without recommendation in 31.1% of resident cases and 63.3% of private practice cases (p < 0.001).
Patients identified in the urban group included Sedgwick and all immediately adjacent surrounding county zip codes. All other zip codes were included in the rural group.
D&C = dilation and curettage.
Regarding re-admission rates, 1 of 14 patients (7.1%) who did not receive antibiotic agents when indicated was re-admitted within 30 days of the surgical procedure. However, there was no difference between receiving indicated prophylactic antibiotic agents and re-admission rates (p = 0.99). In addition, when antibiotic agents were not indicated per guidelines, re-admission rates comparing women who received and did not receive antibiotics did not differ significantly (p = 0.078). Finally, there were four cases of Clostridium difficile identified in our patient population during 2013, two in each cohort. We could not perform statistical analysis because of the small number of cases, and none of these cases were temporally related to prophylactic antibiotic administration or surgical procedure.
Discussion
Our study suggests compliance with guideline-based recommendations for the use of prophylactic antibiotics is high (98.7%). Only 8 of 891 (0.9%) patients undergoing hysterectomy did receive prophylactic antibiotics according to guidelines. In addition, we demonstrate peri-operative antibiotic agents are often administered to women undergoing gynecologic surgeries for which published guidelines are not as well defined.
Our study findings are consistent with the study by Wright et al. [15], which demonstrated a widespread trend toward un-indicated use of antibiotic agents after implementation of policies designed to reduce SSIs. Their study reported non-guideline–based antibiotic prophylaxis increased from 33.4% in 2003 to 43.7% in 2010. In comparison to the study by Joyce et al. [17], our study found that inappropriate use of antibiotic agents for gynecologic surgeries, in which antibiotic agents are not recommended routinely, was slightly higher. Our study found antibiotic agents were administered in 57.1% of the cases for which guidelines recommended against their use. Our study supports this trend in prophylactic antibiotic use and identifies specific surgical procedures during which antibiotic agents are administered when not indicated.
Our findings demonstrate the use of prophylactic antibiotic agents in resident cases align more closely with published guidelines compared with private practice, particularly when the ACOG guidelines recommended no antibiotic prophylaxis usage during the procedure. One explanation is resident physicians and staff attendings might be more aware of the current guidelines. Other studies have shown that teaching hospitals align more closely with published guidelines in regard to peri-operative prophylaxis against venous thromboembolism and SSIs compared with non-teaching hospitals [14,15,18–20]. Another explanation is resident cases may be easier and fall into a well-defined category compared with the cases of the private attendings. An unexpected, likely related, finding we identified was that white women received antibiotic agents when not indicated in 60% of cases, compared with 46.6% and 38.7% of black and Hispanic women, respectively. Interestingly, these findings suggest women who historically experience the greatest health disparities and inequalities, are receiving antibiotic agents that most align closely with published guidelines. The likely explanation is because clinics associated with resident physicians are treating a higher percentage of minorities relative to private attending physician clinics. Future research should be directed at understanding these relations.
Specific policies, such as the Surgical Care Improvement Project (SCIP) in 2003, formed quality measures to improve antibiotic stewardship for hysterectomy procedures [14]. These procedures are audited for use of prophylactic antibiotic agents and the results are reported publicly. In addition, hospital reimbursement is reduced when compliance for these core measures are not met [20]. This has likely led hospitals to implement policies to maintain high compliance with quality measures [21,22]. One of the unintended consequences appears to be a large percentage of women receiving antibiotic agents outside of current guidelines and recommendations. Recently, a national task force was created to prevent the emergence and spread of microbial resistance with one of the stated goals of reducing inappropriate antibiotic use by 50% and 20% in the outpatient and inpatient settings, respectively [23]. Our article highlights that quality improvement efforts need to be developed and implemented to improve antibiotic utilization in an effort to minimize microbial resistance.
A concern regarding the use of unindicated antibiotic prophylaxis is that the decision was made prior to the procedure by facility standing orders and often administered prior to the “Time Out” process in order to comply with SCIP measures. In our institution, and likely in others, a reminder system with computer prompts and laminated cards are posted in the pre-operative area and on all anesthesia machines to enhance on-time antibiotic administration. The high compliance rate with SCIP measures at our institution is likely a result of these processes. However, other safeguards need to be implemented to reduce the use of prophylactic antibiotic agents when not indicated.
Our study has limitations because of the retrospective design and institutional database. Classification of the surgical procedures according to published guidelines is a source of bias. However, the classification of the surgical procedures was performed prior to collection of the antibiotic utilization data, and the principal investigator and senior author attempted to adhere strictly to ACOG guidelines. The problem, and one of the main motivations for the study, is that the guidelines are not defined clearly and are vague in some circumstances. The uro-gynecologic procedures encompassed eight separate procedures in our analysis. However, an additional five procedures could have easily been classified under uro-gynecologic procedures by different reviewers, and likely would have. The classification of the other procedures was straightforward and would not significantly differ. Given the strength of our associations, it is unlikely that a modestly different classification would alter our conclusions. We were unable to match the scheduled procedure with the final procedure performed. It is unknown how often a patient starts in one cohort and migrates to the other after initiation of the procedure, although it is expected to be quite low. In addition, we report only the experience of a single, large teaching hospital in the Midwest and practice patterns are likely to differ in other parts of the country.
The increased utilization of prophylactic antibiotic agents in gynecologic surgeries that do not carry a recommendation has been documented to be widespread [11]. These results support that conclusion. The strength of our study is the detailed review of peri-operative antibiotic use in non-hysterectomy gynecologic procedures performed at our institution. Our large sample size allowed us to identify other factors associated with potential misuse of antibiotics. The goal is to decrease the use of peri-operative antibiotic agents in women who are unlikely to benefit from them while maintaining high compliance for prophylactic antibiotic agents in surgical cases in which evidence suggests a clear benefit. Strategies to improve antibiotic stewardship need to be implemented. Furthermore, clear recommendations from ACOG on antibiotic prophylaxis on non-hysterectomy procedures would likely reduce inappropriate antibiotic use.
Footnotes
Author Disclosure Statement
All authors report no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.