
Abstract
Abstract
Background:
Worldwide, both acute kidney injury (AKI) and sepsis are significant clinical complications, particularly in critical care patients. Sepsis is an important cause of AKI, and AKI is a common complication of sepsis.
Methods:
We reviewed the literature, including current practice guidelines, on sepsis-associated AKI.
Results:
We assessed causes of renal failure, potential mechanisms of sepsis-associated acute kidney injury, current practice guidelines, diagnostic criteria and methods, prevention strategies, treatment options, and outcomes.
Conclusion:
In patients with sepsis-associated AKI, appropriate fluid resuscitation and maintenance of blood pressure are important to prevent further kidney damage. Despite multiple clinical trials, the mechanisms of sepsis-associated AKI and the best treatment options remain unclear.
A
In general, AKI is a sudden decline in renal function with resultant azotemia [8]. Given this vague definition, as well as the difficulty of diagnosing AKI accurately across diverse patient populations, attempts have been made to create a unified and consistent definition and to standardize the diagnostic criteria [8]. Some consensus has been reached through the Acute Kidney Injury Network (AKIN) criteria [9]; the Risk, Injury, Failure, Loss, and End-stage kidney disease (RIFLE) classification [10]; and the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines [11], all of which are described below under “Diagnostic Criteria.”
Sepsis also is a global problem. Currently, it affects about 10% of critical care patients, and the incidence is increasing [12,13]. It can be defined as the body's dysregulated systemic response to infection, ranging from organ dysfunction to septic shock with hypotension and multisystem organ failure. The definition of sepsis was recently refined: It is no longer based on multiple systemic inflammatory response syndrome criteria [14] but rather on changes in the Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score, per the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) [15]. This Sepsis-3 definition, published in February 2016, uses a combination of values to determine the SOFA score, namely, partial pressure of arterial oxygen, fraction of inspired oxygen, platelet count, Glasgow Coma Scale score, bilirubin concentration, blood pressure, and kidney function assessment. Additional factors in the identification of septic shock include the need for vasopressors to maintain the mean arterial pressure (MAP) ≥65 mm Hg or a serum lactate concentration >2 mmol/L despite fluid resuscitation [15].
The treatment of sepsis is resource intensive and expensive [13]. Mortality rates from sepsis remain high, ranging from 20% to 60% in patients with severe sepsis [13,16]. However, with improved sepsis guidelines and better critical care [17], the mortality rate is improving.
Acute kidney injury and sepsis are inextricably connected in many patients: Sepsis is a leading cause of AKI, and AKI is a common complication of sepsis [18]. Acute kidney injury is frequent among patients requiring critical care. The Finnish Acute Kidney Injury (FINNAKI) study demonstrated that AKI affects 40% of patients in the intensive care unit (ICU) [19]. In critically ill patients, AKI is associated with worse outcomes [20] and is particularly prevalent and detrimental in older patients [21]. Sepsis-associated AKI is common: Some studies have demonstrated that about 50% of patients with AKI meet the criteria for sepsis [22].
Sepsis-associated AKI carries a particularly high mortality rate. One multicenter, international study involving an observational cohort of ICU patients demonstrated a 70% in-hospital mortality rate in those with sepsis-associated AKI, compared with about 50% for patients with AKI alone [22]. The patients in that study with sepsis-associated AKI also had more severe illness, more labile changes in vital signs and inflammatory markers, and a higher rate of non-renal organ failure [22].
Another multicenter study highlighted the prevalence of sepsis-associated AKI, which accounted for 12% of critical care admissions. In this study, 32% of the patients with AKI met the criteria for sepsis, and 42% of the patients with sepsis met the criteria for AKI [5].
Comparative studies of patients with sepsis-associated AKI (vs. AKI alone) suggest that the acuity of sepsis-associated AKI is more pronounced, the physiologic changes more drastic, and the mortality rate higher.
In this review, our aim is to highlight the proposed mechanisms of sepsis-associated AKI, as well as its diagnosis, prevention, and treatment.
Causes of Renal Failure
Renal failure can be categorized into pre-renal, intrinsic, and post-renal disease (Fig. 1). Pre-renal disease is the result of reduced renal perfusion, which decreases the glomerular filtration rate and, after a time, can result in cellular damage. Important mechanisms of pre-renal disease include hypotensive disease, low cardiac output, systemic vasodilation, and increased vascular resistance.
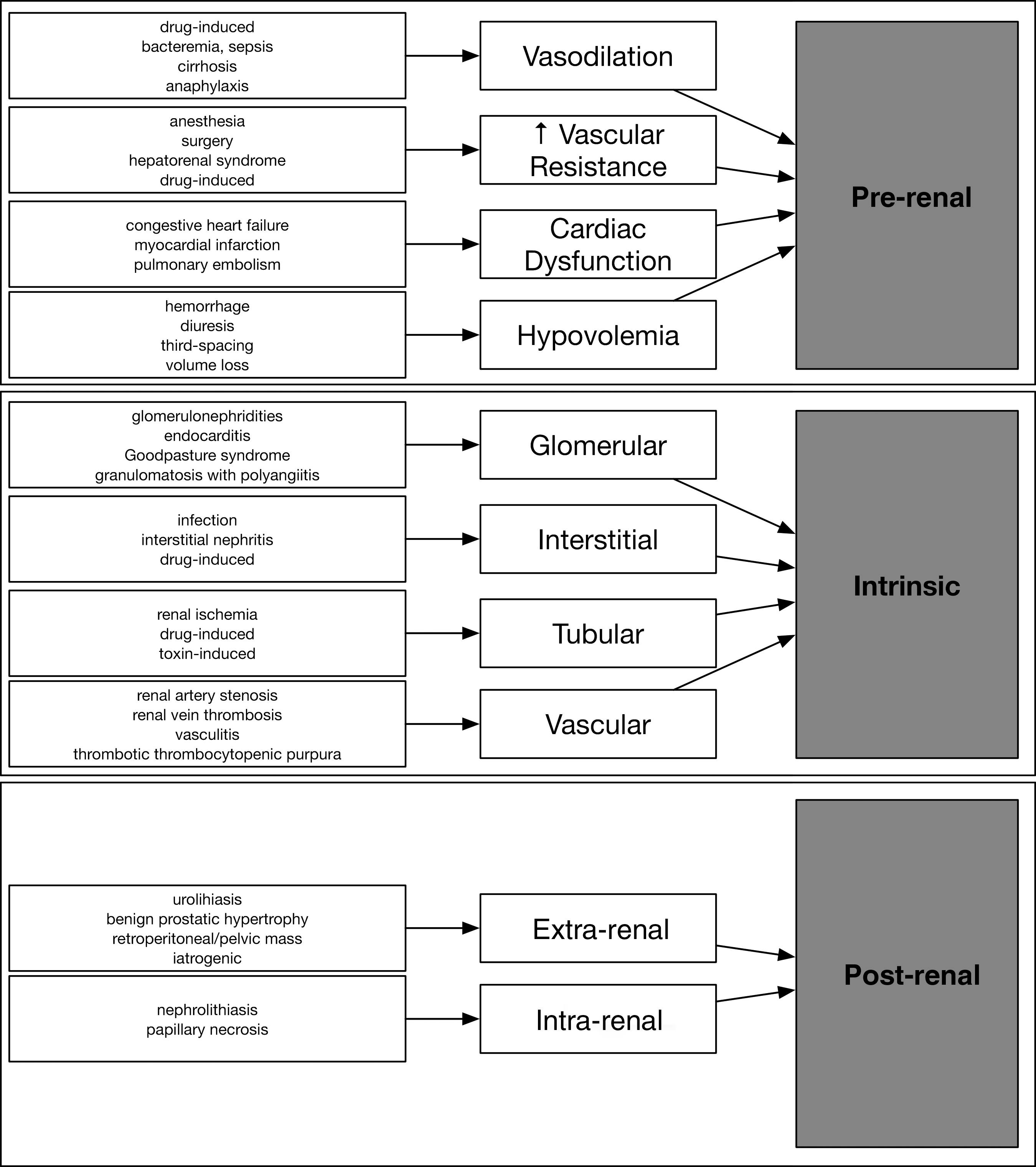
Causes of renal failure.
Intrinsic or intrarenal disease is caused by direct cellular injury to the kidney and can be categorized further by the location of the cellular damage: Glomerular, interstitial, tubular, or vascular [10,23,24].
Post-renal disease is often caused by obstructive uropathy, which can decrease the glomerular filtration rate and cause cellular damage via higher pressure in the collecting system [23]. Post-renal disease can be caused by extrarenal or intrarenal stimuli.
Mechanisms of Sepsis-Associated AKI
The traditional hypothesis has been that AKI in sepsis is caused by hypoperfusion and a subsequent deleterious ischemia–reperfusion mechanism. However, macrocirculatory changes, such as decreased renal blood flow and renal vasoconstriction, are not always present in patients with sepsis-associated AKI, so other hypotheses have been considered.
Renal blood flow
In patients with acute sepsis, the most common etiology of renal disease is pre-renal [25]. Systemic hypotension and renal vasoconstriction also can play a role [26], but the entire picture is significantly more complex. Animal models have demonstrated that renal blood flow is maintained, or actually increases, in sepsis-associated AKI. Confusingly, both renal vasoconstriction and renal vasodilation have been observed [27].
Human renal blood flow measurements are difficult and invasive, and only one study has explored such abnormalities [28]. That study, completed in 1990, evaluated renal blood flow changes with a thermodilution method in eight critically ill patients in which a catheter was inserted percutaneously into the renal vein. In that small cohort, renal blood flow numbers were difficult to correlate with other hemodynamic parameters, and one patient developed renal failure despite high renal blood flow [28].
Another study attempted to use the resistive index of the renal artery, as assessed by Doppler ultrasound imaging, to measure the effects of norepinephrine on renal blood flow in patients with septic shock. The study was limited by its small sample but seemed to demonstrate that an increase in MAP correlates with a decrease in the renal artery resistive index [29].
Changes in renal blood flow in human patients with sepsis-associated AKI are yet to be deciphered completely. It is believed that sepsis-associated AKI can occur despite maintained or increased renal blood flow, but close monitoring of the labile hemodynamic changes in patients with sepsis is still recommended. Hypotension should be avoided, and vasopressor requirements and their potential effect on the renal vasculature should be assessed carefully [29,30].
Sepsis-associated AKI
Multiple hypotheses aim to explain why sepsis results in AKI. Generally, it is accepted that there is some ischemic injury to the kidney. This is thought to be secondary to microcirculatory changes, rather than to a decrease in renal blood flow. Microcirculatory changes can cause shunting and redistribution of blood within the kidney, leading to renal damage and to reduced glomerular filtration pressure [31–34]. In a study in sheep, sepsis and AKI were induced, which preserved oxygenation and perfusion of the renal cortex, but decreased oxygenation and perfusion of the renal medulla [33]. No similar human studies have been conducted.
Most investigators agree that sepsis-associated AKI is complex and poorly understood. Per their “unified theory of sepsis-induced acute kidney injury,” Gomez et al. posited that a combination of mechanisms brought on by sepsis causes AKI, including inflammation and oxidative stress, microcirculatory dysfunction and blood flow mismatch, changes in bioenergetics, tubular cell adaptations, and dysfunctional tubular–glomerular feedback [35]. Wan et al. proposed that the pathophysiology of sepsis-associated AKI involves alternating pro-inflammatory and anti-inflammatory changes that, in turn, result in microcirculatory changes, endothelial dysfunction, thrombosis, cytokine release, and an inflammatory response [36].
Most of the research on the mechanisms of sepsis-associated AKI has been in animals; and some investigators question the translatability of animal models to human physiology, especially given the inconsistent results of some of these animal studies [32]. Theories regarding renal blood flow changes in sepsis-associated AKI remain controversial. Despite the complex theories offered for the causes of sepsis-associated AKI, management of the disorder remains supportive, and little has changed regarding the treatment in some time.
Diagnosis
Diagnostic criteria
The diagnosis and staging of AKI are based primarily on two key parameters: Serum creatinine concentration and urinary output (UO). Until 2004, there was no consensus definition of AKI in critically ill patients. The RIFLE classification, developed in 2004 at the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI), marked the first cohesive definition of AKI [10]. Also in 2004, the AKIN was tasked with facilitating an internationally agreed-on consensus definition of AKI, which gave rise to the AKIN criteria in 2007 [37]. In 2012, the RIFLE and AKIN definitions were merged into the KDIGO guidelines, which are the current consensus definition of AKI. Acute kidney injury is now defined according to three KDIGO stages based on serum creatinine concentration, UO, and the need for renal replacement therapy (RRT) [38]. For a comparison of the three definitions, see Table 1.
AKI = acute kidney injury; AKIN = Acute Kidney Injury Network; GFR = glomerular filtration rate; KDIGO = Kidney Disease: Improving Global Outcomes; RIFLE = Risk, Injury, Failure, Loss, and End-stage kidney disease; RRT = renal replacement therapy.
One criticism of these diagnostic criteria is that the markers measure only the kidney's excretory function, neglecting its important metabolic and endocrine roles. Additionally, the primary use of serum creatinine concentration and UO as markers of excretory function has come under fire. Criticisms of the use of serum creatinine include its decreased production during critical illness, its interactions with drugs, and the influence of the volume status of individual patients on the measurements. Criticisms of the use of UO include the facts that it is not renal specific and that it is influenced significantly by hormonal changes (e.g., antidiuretic hormone), changes that can result from trauma, surgery, pain, and nutritional status. In light of these criticisms, a robust search for novel diagnostic biomarkers of renal function persists.
Biomarkers
Prediction and more accurate diagnosis of AKI were thought to be possible with biomarkers, often used in attempts to detect early injury before loss of organ function. Novel biomarkers have been created in attempts to detect AKI, which is notoriously difficult to diagnose in patients with clinical confounders, such as sepsis and critical illness [39]. Interleukin-18 (IL-18), in particular, has been found to be useful in diagnosing sepsis-associated AKI [40]. Biomarkers have been studied as adjuncts to the current methods of AKI diagnosis, which are criticized for their late detection of injury and their inconsistency among different patient physiologies [41]. Other major biomarkers of interest in AKI are neutrophil gelatinase-associated lipocalin (NGAL), cystatin-c (cys-c), kidney injury molecule-1 (KIM-1), and liver-type fatty acid-binding protein (L-FABP) [39–41, 43–52]. For a summary of their characteristics, see Table 2.
AKI = acute kidney injury; cys-c = cystatin-c; IL = interleukin; KIM-1 = kidney injury molecule-1; L-FABP = liver-type fatty acid binding protein; NGAL = neutrophil gelatinase-associated lipocalin.
Biomarkers have not yet made a significant difference in the clinical management of AKI, but perhaps further research will increase their utility [41,42].
Pre-renal disease workup
Once AKI is identified, determining the causative factor, with the aid of several adjunctive tests, is important. Initial workup of patients with sepsis-associated AKI should include rapid evaluation for the causes of pre-renal and post-renal disease, conditions that typically can be corrected rapidly. Traditionally, fractional excretion of sodium (FENa) has been measured to distinguish pre-renal disease from acute tubular necrosis (ATN). With the presence of renal hypoperfusion, the kidney will hold on to sodium and urea, and urine osmolarity will increase, thereby decreasing FENa. The following equation is used to calculate FENa, where U = urinary, Na = sodium, S = serum, and Cr = creatinine:
A FENa value <1% is indicative of pre-renal disease; >2%, ATN. Note that those cutoffs apply only to patients with a diagnosis of AKI. In healthy patients, FENa should not be used to evaluate volume status.
Recent studies have questioned the accuracy of FENa in diagnosing pre-renal disease. For example, several non-pre-renal disease processes can cause a FENa value <1%, such as congestive heart failure, hepatorenal syndrome, post-ischemic ATN, contrast-induced nephropathy, and ATN associated with early sepsis [53,54]. Diuretics, dopamine, and high salt use (all of which increase the amount of sodium in the urine) can interfere with the accuracy of FENa testing. The opposite is true for norepinephrine and low-salt diets (which decrease the amount of sodium in the urine). One potential way to exclude any impact of diuretics on test results is by measuring fractional excretion of urea (FEUrea). Any FEUrea value <35% suggests pre-renal disease; >50%, ATN [55]. Unfortunately, many of the other criticisms of FENa testing also are valid for FEUrea testing.
Post-Renal Disease Workup
In patients with AKI, the most common initial test—and the initial test of choice to rule out obstructive uropathy—is two-dimensional gray-scale ultrasound scanning. This imaging modality yields positive results in 10% of patients with AKI [56]. Ultrasound can help identify and classify the degree of post-renal obstruction, as well as to pinpoint the cause. In addition to kidney size, echogenicity can measure cortical thickness to assist in the workup of AKI.
Prevention
Fluid resuscitation
In critically ill patients with sepsis, appropriate fluid management is essential to minimize the risk of pre-renal AKI. Patients with systemic sepsis suffer from reduced intravascular oncotic pressure, which promotes extravasation and hastens tissue edema. Thus, fluid administration must be judicious. Excess fluid promotes tissue edema and organ failure, specifically pulmonary failure. Alternatively, hypovolemia can decrease cardiac pre-load and renal perfusion, thus hastening AKI.
Unfortunately, no single objective marker of fluid volume exists to guide resuscitation. Historically, central venous pressure (CVP) has been employed as a marker of volume status in patients with sepsis; however, significant work by Marik et al. has disproven CVP as a valid marker of volume status [57,58]. Their work is reflected in the most recent 2016 Surviving Sepsis Campaign guidelines, from which the recommendation to target a CVP goal was removed [59]. Other methods of determining volume status and responsiveness include the straight leg-raise test, esophageal Doppler ultrasonography, hemodynamic transesophageal echocardiography (hTEE), serial transthoracic echocardiography (TTE), and inferior vena cava variation assessment [25,60–62]. We prefer using serial TTE in conjunction with inferior vena cava variation assessment to help guide fluid resuscitation in patients with acute sepsis.
As described above, the development of AKI in patients with sepsis is not related entirely to volume status and can occur even in the face of normal or increased renal blood flow. It therefore is important to minimize additional insults, such as reduced renal blood flow. We recommend resuscitation with Ringer's lactate solution for the initial care of patients with sepsis. Previous studies have shown that a balanced crystalloid infusion is associated with less AKI than infusion of 0.9% saline [63, 64]. Dextran and hydroxyethyl starch must be avoided in light of the overwhelming evidence of the harm those fluids can cause in patients with sepsis [65,66].
The use of albumin remains much more controversial. In the Saline versus Albumin Fluid Evaluation (SAFE) trial, 6,997 ICU patients were randomized to either albumin or saline; no significant differences were noted in the rates of all-cause death or new organ failure [67]. Of importance, only 40% of the patients had undergone surgery, only 18% had sepsis, and only 1% required RRT, so the applicability of the findings to patients with sepsis-associated AKI is not clear. However, on subgroup analysis, a (nonsignificant) trend toward a lower 28-day mortality rate was seen in the severe sepsis cohort receiving albumin (30.7%) rather than saline (35.3%; relative risk [RR] 0.87; p = 0.09). That trial was not powered to detect significant differences among subgroups.
A decade later, in the Albumin Italian Outcome Sepsis (ALBIOS) trial, 1,818 patients with severe sepsis and septic shock were randomized to resuscitation either with or without albumin [68]. No significant differences were noted in the rate of all-cause mortality at 28 and 90 days, in the development of AKI, or in the need for RRT. However, on subgroup analysis, the cohort with septic shock at enrollment had a better rate of survival with albumin (49.9%) than without (43.6%; RR 0.87; p = 0.03).
Target MAP
Adequate MAP is essential to prevent AKI. Unfortunately, when renal autoregulation is exceeded and renal blood flow decreases, the appropriate MAP threshold is unknown. The Surviving Sepsis Campaign recommends resuscitation to a MAP of 65 mm Hg for patients with septic shock. However, that target is controversial, with some investigators claiming it is too low to maintain kidney function [69].
In an attempt to identify the optimal minimal MAP to prevent AKI, Badin et al. enrolled 217 critically ill patients in an observational study that evaluated four subgroups (presence or absence of AKI ± the presence of septic shock). In patients with septic shock and sepsis-associated AKI at randomization, a higher MAP (72 to 82 mm Hg) during the first day of treatment was associated with a lower incidence of AKI at 72 hours (p < 0.05). These results suggest that a MAP target >72 mm Hg in patients with acute septic shock and early sepsis-associated AKI might protect against the progression of renal disease [70].
The large multicenter Sepsis and Mean Arterial Pressure (SEPSISPAM) trial attempted to clarify a MAP target. Patients with septic shock were randomized to either a high (80 to 85 mm Hg) or a low (65 to 70 mm Hg) MAP target. No differences were found in the two primary outcomes in the high vs. low target groups: 28-day mortality rate (36.6% vs. 34.0%; p = 0.57) and 90-day mortality rate (43.8% vs. 42.3%; p = 0.74). In patients with a history of hypertension, a high MAP target was associated with less need for RRT (31.7% vs. 42.2%; p = 0.046) and with a lower rate of plasma creatinine doubling (38.9% vs. 52%; p = 0.02). One major criticism of this trial is that the low-MAP target group exceeded the target MAP by day two, so its range actually was 75 to 80 mm Hg [71].
The optimal blood pressure target to minimize AKI in patients with sepsis is still being debated, but the vasopressor of choice is less uncertain. Multiple studies have shown that norepinephrine should be the first-line vasopressor in such patients [72,73].
Treatment
Type of RRT
In the FINNAKI study, depending on the particular ICU, 3% to 36% of patients with septic shock who developed AKI were started on RRT [74]. At our institution, the practice is to begin such patients on continuous RRT (CRRT) instead of intermittent hemodialysis (iHD). Patients in shock are less likely to tolerate the large fluid swings of iHD; some evidence suggests that unstable patients treated with CRRT have higher renal recovery rates than those treated with iHD [75, 76]. Hybrid versions of RRT, such as sustained low-efficiency dialysis (SLED), are gaining popularity. The benefits include less downtime and a reduced anticoagulation requirement compared with CRRT. Data are limited regarding SLED's role in hypotensive patients with sepsis; further research is needed [77,78].
Timing of RRT
Our practice is to begin RRT when patients meet the absolute indications for it, which are often taught to students using the “AEIOU” mnemonic:
Despite the KDIGO guidelines, great controversy remains over the optimal time to begin RRT, as shown by the following four studies.
(1) A 2011 meta-analysis of 15 studies that examined the question of early vs. delayed RRT in critically ill patients with AKI found that early RRT was associated with a higher 28-day mortality rate (odds ratio [OR] 0.45; 95% confidence interval [CI] 0.28–0.72) [79]. But significant variation existed between the trials regarding the definition of early vs. late RRT. Of the 15 studies analyzed, only two were randomized; nine were retrospective, and only two included patients with sepsis. The overall methodologic quality among the 15 studies was low.
(2) A substudy of the FINNAKI trial results compared the outcomes of early vs. late RRT [19,80]. The authors defined classic RRT by the presence of at least one absolute indication before RRT began and pre-emptive or early RRT by the presence of no absolute indications. The crude 90-day mortality rate was 48.5% after classic RRT and 29.5% after pre-emptive or early RRT. Classic RRT was associated with a significantly higher mortality risk (OR 2.05; 95% CI 1.03–4.09). Furthermore, patients who met the criteria for classic RRT but did not undergo immediate dialysis had a significantly higher risk-adjusted 90-day mortality rate (68%) than those who underwent immediate dialysis (35%) (OR 3.85; 95% CI 1.48–10.22). One major criticism of the FINNAKI study is that it was observational with a significant risk for bias. Another major criticism is that all patients in both cohorts underwent RRT; it is possible that some patients in the classic arm would have recovered renal function and not required RRT, likely decreasing the mortality rate in that arm.
(3) The landmark Early versus Late Initiation of Renal-Replacement Therapy in Critically Ill Patients with Acute Kidney Injury (ELAIN) trial—a single-institution randomized, controlled study—compared early RRT (beginning within 8 hours after diagnosis of KDIGO stage 2 AKI) and delayed RRT (beginning within 12 hours after diagnosis of KDIGO stage 3 AKI or after development of an absolute indication for RRT) [81]. All patients had at least one of the following conditions: severe sepsis, vasopressor requirement, refractory fluid overload, or non-renal organ dysfunction. Only patients with an NGAL value >150 ng/dL were included (this was the first large AKI study using a renal biomarker to define its inclusion criteria). Patients in the early RRT group had a significantly lower 90-day mortality rate (39.3%) than those in the delayed RRT group (54.7%; p = 0.03; number needed to treat = 7). Patients in the early RRT group had a shorter duration of RRT, enhanced recovery of renal function at 90 days, a lower median duration of mechanical ventilation, and a shorter hospital length of stay (p < 0.05). One weakness of the ELAIN trial is its single-institution nature. Other major weaknesses include a low fragility index (3) and a high proportion of cardiac surgery patients [82].
(4) The Artificial Kidney Initiation in Kidney Injury (AKIKI) trial—a multicenter randomized, controlled trial involving 31 ICUs in France—compared early RRT (beginning within 6 hours after diagnosis of stage 3 KDIGO AKI) and delayed RRT (after development of an absolute indication for RRT) [83]. Importantly, 80% of the patients in each arm had a diagnosis of sepsis. No significant difference was noted in the primary outcome in the two groups: The 60-day mortality rate was 48.5% vs. 49.7% (p = 0.79). Only 51% of the patients in the delayed RRT group underwent RRT vs. 98% in the early RRT group. A significant weakness of the AKIKI trial was its use of iHD in more than 50% of the patients, many of whom required vasopressors when they began RRT.
All of those studies had relatively heterogeneous populations, which are difficult to compare. Much of the evidence points to potentially improved outcomes and a decreased mortality rate after early RRT; however, the AKIKI trial points to similar outcomes for the treatments. Further research is needed, specifically in patients with sepsis-associated AKI, because they have different physiologic effects and recovery trajectories than patients with AKI alone.
Outcomes
Unfortunately, sepsis-associated AKI is associated with a significantly worse prognosis than either sepsis or AKI alone [5,22,84]. Patients with sepsis-associated AKI have an in-hospital mortality rate >30%; moreover, depending on the AKIN stage, the rate differs, ranging from 35% for stage 1 to 64% for stage 3 [85]. Yet survivors of sepsis-associated AKI have a high rate of complete renal recovery (95.7%).
Conclusion
In patients with sepsis, AKI is a significant problem to consider. Nearly 50% of the cases of AKI in critically ill patients involve sepsis. Some recent research has shown promise, but the mechanisms of sepsis-associated AKI are complex and remain poorly understood. Clinicians and researchers continue to strive for an accelerated and more accurate diagnosis of AKI in patients with sepsis. The role of fluid resuscitation and RRT is still unclear in patients with sepsis-associated AKI; recent work has shown that the development of AKI in patients with sepsis is not attributable solely to pre-renal causes. More research is needed to resolve the uncertainty surrounding not only the treatment of sepsis-associated AKI but also its mechanisms and diagnosis.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors of this manuscript.