
Abstract
Abstract
Background:
The high mortality rate of patients suffering from severe trauma is based not only on the mechanism of injury, but also on the higher risk for development of subsequent infections. Therefore, the early recognition of infection after severe trauma is of particular importance for patient outcome. However, early diagnosis is often masked by the consequences of the sterile, damage-triggered immune response. Our study sought to analyze the course of soluble CD14-subtype (sCD14-ST, presepsin) compared with clinically established inflammatory and infectious biomarkers in a cohort of patients with severe trauma.
Patients and Methods:
Between January 2015 and February 2016, 50 patients suffering from severe trauma (Injury Severity Score [ISS] > 16) were enrolled and followed up for seven consecutive days after intensive care unit (ICU) admission. Clinical routine data, signs of infection, and the inflammatory biomarkers presepsin, C-reactive protein (CRP), procalcitonin (PCT), and interleukin-6 (IL-6) were assessed.
Results:
Regarding the well-established biomarkers CRP, PCT, and IL-6, we observed trauma-associated alterations (day 1: CRP 13 mg/L, interquartile range [IQR] 0–129; PCT 1.1 μg/L, IQR 0–13; IL-6 108 pg/mL, IQR 29–795), which did not correlate with the clinical development of systemic inflammatory response syndrome (SIRS), whereas elevated plasma concentrations of presepsin in the clinical course were associated with the presence of SIRS (presepsin: no-SIRS vs. SIRS p = 0.03).
Conclusion:
Our study investigates systematically the kinetic of presepsin compared with established inflammatory and infectious markers after severe trauma. Presepsin is neither affected by the early post-traumatic nor the delayed immune response over seven days after trauma, making it a possible option as a diagnostic biomarker of infection worth further evaluation.
S
Tissue hypoperfusion during shock and subsequent cell death as well as the direct physical damage result in the release of immunogenic damage-associated molecular patterns (DAMPs), capable of triggering a systemic inflammatory response syndrome (SIRS) [2,3]. Damage-associated molecular patterns (DAMPs) are recognized by a variety of pattern recognition receptors (PRRs) [4]. Among these receptors, especially the activation of toll-like receptors (TLRs) leads to the release of pro-inflammatory and anti-inflammatory mediators, which can trigger excessive inflammation, sepsis, and multiple organ failure (MOF) [5,6].
Currently the development of infection and sepsis after severe trauma represents a major challenge to modern intensive care medicine. Despite continuous progress in antibiotic therapy, surgical source control, and adjuvant therapies, sepsis remains one of the most common disease entities in intensive care units (ICUs) and is reported as a main cause of death among critically ill patients [7–9].
The high mortality rate of patients with severe trauma is based not only on the trauma mechanism, but also on the higher risk for the development of infections [10]. An epidemiologic study reports an incidence of 4% of trauma-associated infectious complications, especially blood stream infections [11]. Therefore, the early diagnosis of infection and immediate administration of anti-infective therapy is of particular importance for the severely injured patient's outcome. However, early and rapid diagnosis of infection is often impeded by the physiologic reactions of sterile damage-triggered immune response [12]. In order to differentiate post-traumatic SIRS from nosocomial infections, the predictive value of intensive care scoring systems such as Acute Physiology And Chronic Health Evaluation (APACHE II) score or Injury Severity Score (ISS) have been validated [13], but are still discussed controversially [14]. Biomarkers are seen as a supplemental approach within this context, whereas the acute phase proteins C-reactive protein (CRP), procalcitonin (PCT), and interleukin 6 (IL-6) are the most commonly used biomarkers for early assessment of infection in daily clinical routine [14]. The new biomarker soluble CD14 subtype (sCD14-ST, presepsin) exhibits a high diagnostic value of detecting patients with sepsis within different clinical contexts [15,16]. Furthermore, plasma presepsin levels indicate a more specific infectious origin of inflammation among different cohorts of patients in comparison to the established infectious biomarkers CRP, PCT, and IL-6, which regularly show alterations resulting from non-infectious origins [15,17–22]. In a pilot cohort study, Hoshino et al. [23] found no trauma-associated elevation of presepsin in patients 24 hours after severe trauma. This study sought to analyze the course of presepsin compared with established inflammatory biomarkers (CRP, PCT, IL-6) in patients suffering from severe trauma.
Patients and Methods
Study Design
After approval by the local ethics committee (No. 164/14), we performed a prospective observational study (German Clinical Trials Register, Trial registration: DRKS00010991). Between January 2015 and February 2016, 50 consecutive trauma patients were enrolled at the surgical intensive care unit (ICU) of the University Hospital of Giessen (Germany). All enrolled patients gave written informed consent or written informed consent was obtained from the nominated legally authorized representative on behalf of participants in accordance with ethical standards. Inclusion criteria were defined as at least 18 years of age, severe trauma (ISS >16), and admission to the surgical ICU. Patients were excluded in cases of positive history of chronic viral diseases (human immunodeficiency virus [HIV], hepatitis B/C). Patients were observed for seven consecutive days after ICU admission and screened for signs of infection and SIRS according to the criteria of the Society of Critical Care Medicine (SCCM) and the American College of Chest Physicians (ACCP) [24].
Management of blood samples
Blood samples were collected at study inclusion and in the morning on the seven consecutive days in the ICU. Quantification of presepsin was performed with 7.5 mL heparinized blood at each time point of extraction using a point-of-care analyzer (PATHFAST™ Presepsin, Mitsubishi Chemical, Tokyo, Japan) according to the manufacturer's instructions. Additional laboratory data were obtained from clinical routine blood analysis and contained inflammatory parameters PCT, CRP, IL-6, and leucocyte count. For CRP, PCT, and IL-6 quantification lithium heparin plasma samples were used. C-reactive protein was measured with the Siemens ADVIA® system (Siemens, Erlangen, Germany) using the manufacturer's reagent, whereas PCT was quantified by the Siemens Centaur® system and Thermo Fischer Scientific Brahms reagent (Brahms, Henningsdorf, Germany). Interleukin-6 was measured by the Siemens Immulite® system using the Siemens reagent.
Data management and statistical analysis
Clinical routine data were extracted from an electronic patient data management system (ICUData®, Imeso GmbH, Giessen, Germany) and included patient's baseline data, vital signs, and relevant intensive care therapy information. For multiple group comparisons, an initial global Kruskal-Wallis test was performed, followed by Mann-Whitney U test for pairwise comparisons in case of rejected global null hypothesis (p < 0.05). Correlation analysis included non-parametric Spearman ρ testing; SPPS (version 23, IBM, Armonk, NY) was used for statistical analysis.
Results
Study population
During the recruitment period, we included 50 adult patients suffering from severe trauma. A first blood sample was taken after initial resuscitation and, if necessary, after damage control surgery. The maximum elapsed time between hospital admission and first blood sample was 15 hours. The cohort consisted mainly of male patients (72%) with a median age of 47 years (interquartile range [IQR] 19–83 y; Table 1). The patients presented with a median body mass index (BMI) of 24.7 kg/m2 (IQR 20.2–32.9 kg/m2) and the high severity of injuries was reflected by a median ISS of 22 (IQR 17–34).
Values are given as number (% total) or median (interquartile range) for age, BMI, clinical scores, and durations.
APACHE II = Acute Physiology And Chronic Health Evaluation Score; BMI = body mass index; COPD = chronic obstructive pulmonary disease; ICU = intensive care unit; ISS = Injury Severity Score; NISS = New Injury Severity Score; RISC = Revised Injury Severity Classification Score, SOFA = Sequential Organ Failure Assessment Score.
In the majority of cases, patients presented with thoracic injuries (90%), followed by injuries to the external tissue (86%) and limbs (70%). Three patients (6%) died during the 30-day observation period from a trauma-related non-infectious cause, of whom one patient (2%) died within the first 24 hours of treatment. The median length of ICU stay was six days (IQR 2–34 d) and the overall median hospital stay was 18 days (IQR 3–46 d). Thirty patients (60%) developed SIRS at some point during their hospital stay. One case of sepsis was observed within our study cohort during the subsequent seven-day clinical observation period. We registered two cases of acute kidney failure and one hemostasis dysfunction based on liver injury. There was no chronic liver or kidney disease in the patient's medical history.
Time course of presepsin, PCT, CRP, and IL-6 after trauma
Presepsin, IL-6, and PCT were measured daily over a period of seven days after hospital admission (Fig. 1). We observed initial presepsin concentrations of 487 pg/mL (IQR 123–1901) with no obvious kinetic over time (Fig. 1A; p = 0.746). On day 6, the concentrations of presepsin were highest within the observation period (802 pg/mL, IQR 100–4298). In contrast, IL-6 values were increased early after trauma (108 pg/mL, IQR 29–795) and gradually decreased over time until day six (36 pg/mL, IQR 0–364; Fig. 1B; p < 0.001). We also found PCT concentrations above the local hospital cutoff (> 0.5 μg/L) during the first three days after admission, with highest concentrations on day one (median: 1.1 μg/L, IQR 0–13) and an average decrease below pathologic concentrations at day four (Fig. 1C; p = 0.002). Lowest CRP values were found at hospital admission (13 mg/L, IQR 0–129), peaking on day 2 (166 mg/L, IQR 65–351) (Supplementary Fig. S1A; p < 0.001; see online supplementary material at http://www.liebertpub.com/sur), whereas leucocytes increased late on day six and later (Supplementary Fig. S1D; p < 0.001).

Course of biomarkers during the observation period. Course of median presepsin (
Presepsin, PCT, and IL-6 at hospital admission according to the severity of trauma
Baseline values of presepsin, IL-6, and CRP at hospital admission were clustered into three groups according to trauma severity (reflected by the ISS; Fig. 2A–2C). An ISS <20 is a predictor for lower mortality [25] and an ISS >30 indicated approximately 10% worst-injured patients in our study cohort. Regarding presepsin or PCT, we did not observe differences between the groups (Fig. 2A and 2C). In contrast, we found differences in IL-6 between patients of the lowest (ISS 16–20) and highest ISS (ISS >30; p = 0.05) as well as between the population of moderate (ISS 21–30) and highest ISS (p = 0.022; Fig. 2B). Median IL-6 values at hospital admission were considerably elevated in all three groups (local hospital cutoff value ≥50 pg/mL) (ISS 16–20: 66 pg/mL, IQR 0–550; ISS 21–30: 105 pg/mL, IQR 29–795; ISS >30: 435 pg/mL, IQR 165–1203).
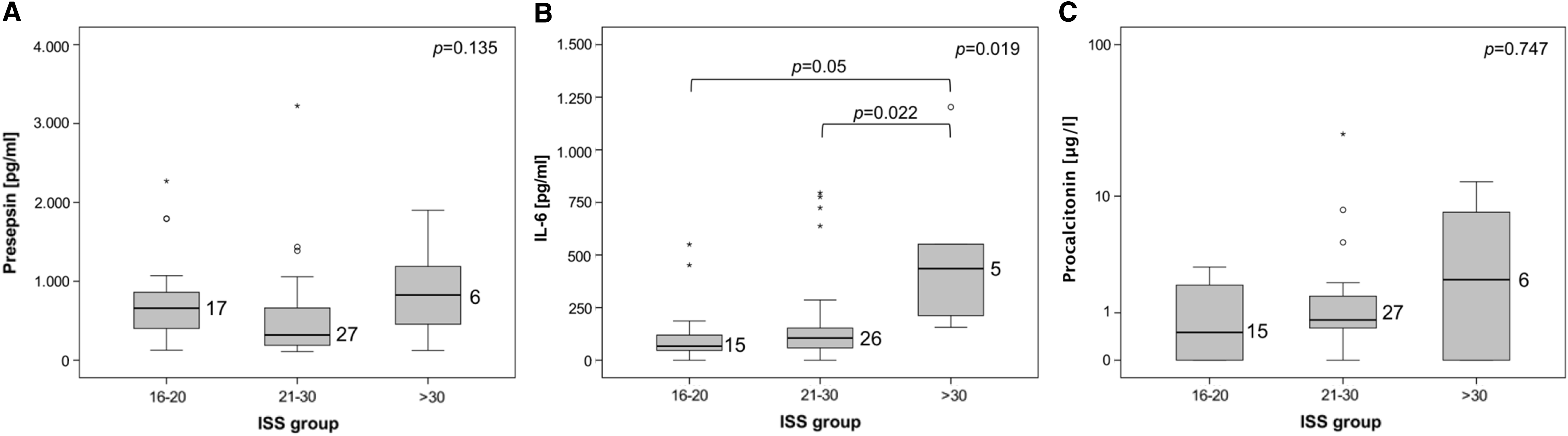
Biomarker values according to severity of illness at hospital admission. Median presepsin (
Association of biomarkers with the clinical presence of SIRS
To evaluate the association of biomarker plasma concentrations with the presence of SIRS, all available samples were stratified by the occurrence of SIRS or no-SIRS. Changes between presepsin and IL-6 were identified (presepsin: no-SIRS vs. SIRS p = 0.03; IL-6: no-SIRS vs. SIRS p = 0.03; Fig. 3A and 3B). In contrast, PCT values did not differ between SIRS and no-SIRS patients (p = 0.504; Fig. 3C).

Association of biomarkers with the clinical presence of systemic inflammatory response syndrome (SIRS). Comparison of median presepsin (
Presepsin and PCT values in patients with or without abdominal trauma
Differentiating patients with or without abdominal injuries, higher median values of presepsin and PCT were observed during the clinical course after abdominal trauma. For presepsin, plasma levels between groups of patients with and without abdominal trauma began to increase from day five (not significant; Fig. 4A). In contrast, PCT was increased in patients with abdominal trauma from day two and persisted throughout the observation period (Fig. 4B).

Correlation analyses of the investigated biomarkers Comparison of median presepsin (
Correlation of investigated biomarkers
Upon stratification of the samples into four groups according to their PCT concentrations, a clear trend of increasing presepsin concentrations can be observed (Fig. 4C). Moreover, the plasma concentrations of the biomarker presepsin exhibited a positive and significant correlation to all examined classic biomarkers (IL-6: p < 0.001; PCT: p < 0.001; CRP: p = 0.003), but only with IL-6 and PCT to a moderate extent (p = 0.479 and p = 0.449, respectively; Fig. 4D).
Discussion
Our study sought to examine the kinetics of established and novel biomarkers of inflammation and infection in patients suffering from severe trauma to evaluate their usefulness in this context. Trauma patients are at high risk for developing infectious complications during their hospital stay. Therefore, early and accurate differentiation between sterile inflammation and infection might reduce delayed trauma-associated mortality [10,11].
Biomarkers are used for the prediction of inflammatory and infectious processes among different cohorts of patients. Previous studies have shown a trauma-associated elevation of routinely used biomarkers [26–28], rendering them not sensitive enough to detect infection among trauma cohorts with high values of trauma-associated sterile inflammation and increasing the need for novel markers. Former study data support presepsin as a powerful marker for the diagnosis of infection, especially sepsis among different cohorts of patients [15,29–31]. Hoshino et al. [23] found no trauma-associated elevation of presepsin in trauma patients 24 hours after severe trauma [23]. Our study also proves presepsin to be uninfluenced by the early sterile inflammatory response after trauma, whereas it still adheres to the clinical presence of SIRS.
The systemic immune response after major trauma has been shown to cause severe damage to multiple organs caused by the initial cascade of inflammation aggravated by subsequent infection—and in the worst case, sepsis—to which the body has become susceptible [32]. Among our study cohort, no initial trauma-induced increase of presepsin was detected, but a delayed increase of its plasma concentrations, especially on the third and fourth day after trauma. Regarding the results from earlier study cohorts, normal values for presepsin were reported as 517 pg/mL [33] and 58–339 pg/mL [34]. Investigating surgical patients with suspected abdominal sepsis, Vodnik et al. [35] observed higher presepsin values in patients with confirmed sepsis (1508.3 ± 866.6 pg/mL) compared with patients representing isolated SIRS (430.0 ± 141.33 pg/mL; p < 0.0001). Additionally, Zhang et al. [36] identified presepsin as an effective biomarker for the diagnosis of sepsis in a systematic meta-analysis. Among the 11 included studies, the threshold ranged from 317 to 729 pg/mL, the area under the curve (AUC) ranged from 0.70 to 1.00, sensitivity from 0.70 to 1.00, and specificity from 0.62 to 0.93. Regarding these findings, compared with the values observed in our study cohort (time of admission 487 pg/mL [IQR 123–1901] with no obvious change over time), we conclude that longitudinal marker assessment might be superior to single-point or cross-sectional assessment with a binary cutoff value in the discrimination between sterile SIRS and infection.
Grotz et al. [37] hypothesized that SIRS in patients presenting with severe abdominal trauma is based on the translocation of bacteria through the intestinal wall as a result of tissue hypoperfusion [38]. Activation of the gastrointestinal immune system results in an irritation of visceral nerves leading to a neuro-humoral mediated SIRS. Our data do not support presepsin as being sensitive for SIRS after abdominal trauma. This may be explained by the neurohumoral genesis of non-sterile SIRS after abdominal injury, which may alter the concentrations of presepsin. In contrast, PCT issued sensitivity for SIRS within the clinical course after traumatic abdominal injury. Nevertheless, patients with a high level of PCT presented a trend toward higher levels of presepsin (considering all time points). For PCT, we can observe a trauma-induced increase, which was according to our data, irrespective of the trauma severity or the presence of SIRS.
Among the established biomarkers of inflammation and infection, IL-6 is known to predict an early phase of inflammation before the increase of circulating CRP and fever occurs. It has been proven that during bacterial infections, IL-6 concentrations increase as early as within two hours after endotoxin administration and then gradually decrease [39]. Interleukin-6 is also useful as a negative prognostic marker in patients newly admitted to ICUs across the entire spectrum of SIRS severity [40]. For example, current guidelines for the diagnosis and treatment of sepsis among pediatric patients recommend the clinical use of IL-6 [41]. In contrast, in our study we were not able to identify an association of IL-6 with trauma patients experiencing a SIRS. In line with the study of Gebhard et al. [42], we showed an early increase of IL-6 after severe trauma. Moreover, consistent with previous studies, patients with the most severe injuries presented with the highest IL-6 plasma levels [42,43].
The available literature for the course of CRP after severe trauma reported near-normal serum CRP levels on admission (median 8.5 mg/L vs. 7.5 mg/L), reaching peak values (median 110 mg/L) three days after trauma [44], corresponding with our findings. Giannoudis et al. [44] reported no correlation between CRP and ISS in a trauma population, which is also in line with our current data.
Serum PCT levels increase in severe systemic infections but may also be elevated in non-infectious conditions [18,45]. Whereas only a minimal increase of PCT plasma levels is observed in cases of SIRS, significant elevation occurs in (gram-negative) sepsis [46]. PCT plasma re-induction indicates possible septic complication during SIRS after major trauma. In addition, high PCT concentration in trauma patients at ICU admission indicates an increased risk of septic complications [47]. Nevertheless, we are not able to demonstrate an association between PCT and the occurrence of SIRS after severe trauma.
This study has some limitations. With only 50 patients, the statistical power of the study is limited, but nevertheless, to our knowledge, this is the first prospective study that evaluates systematically the course of presepsin levels compared with clinically used biomarkers of inflammation and infection. Furthermore, the measured mortality among our study cohort (6%) seemed low. That might be because we did not include pre-hospital and trauma room deaths. Further studies enrolling a larger number of patients need to be conducted to clarify the usefulness of presepsin in this context.
Conclusion
Our study investigates systematically the kinetic of presepsin compared with established inflammatory and infectious markers following severe trauma. Presepsin is neither affected by the early post-traumatic nor the delayed immune response over seven days after trauma, making it a possible option as diagnostic biomarker of infection worth further evaluation.
Footnotes
Acknowledgments
The authors thank the staff of the surgical ICU at the University Hospital of Giessen for their assistance in identifying study members, for clinical advice, and Ilona Magel from the laboratory of experimental Anaesthesia for excellent technical assistance.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.