
Abstract
Abstract
Background:
Surgical site infections (SSIs) are among the most common complications after definitive treatment for intestinal fistulae. Serum inflammatory markers including white blood cell count (WBC), C-reactive protein (CRP), interleukin-6 (IL-6), as well as procalcitonin (PCT) have been used to help diagnosis post-operative complications.
Objective:
The goal of this study was to assess the clinical value of inflammatory markers, specifically IL-6, in predicting SSIs after intestinal fistulae resection.
Methods:
A total of 184 consecutive patients who underwent elective intestinal fistula resection were enrolled prospectively. All patients were screened to exclude patients with existing clinical infection. Plasma IL-6 concentrations, serum PCT, and CRP concentrations were measured pre-operatively and on post-operative days one, three, and seven. The predictive value of each laboratory marker for SSI was calculated.
Results:
The incidence of SSI after elective intestinal fistula resection was 26.7%. Interleukin-6, PCT, and CRP concentrations were higher in patients with SSIs compared with patients without. In contrast, there was no statistical difference for WBC counts between the two groups. Receiver operating characteristic curves demonstrated that IL-6 had the highest diagnostic effectiveness for post-operative SSI on post-operative day one, with an area under the curve of 0.77, and a sensitivity of 85.7% and specificity of 63.9%.
Conclusion:
A concentration of IL-6 above 95.6 ng/L on post-operative day one and 52.5 ng/L on post-operative day three, and a concentration of PCT exceeding 0.61 mcg/L predict the occurrence of SSI after definitive operations for gastrointestinal fistulae.
S
Resection of intestinal fistulae, similar to many operations involving the bowel, are often associated with gross contamination to some degree. Subsequently, these patients have a higher risk of developing SSIs compared with patients in whom the gastrointestinal tract is not violated. More specifically, patients with gastrointestinal fistulae have a heightened inflammatory environment that may contribute to the increase occurrence of SSI in this patient population subset [2]. Therefore, early detection and management of SSI after fistula resection are important.
The process of incision healing is a well-studied subject, involving numerous inflammatory markers and cytokines guiding an orchestra of cellular machinery with each contributing a vital role. A number of studies have investigated these inflammatory biomarkers to improve the early diagnosis of post-operative infection. Several serum inflammatory markers have been used for the diagnosis of SSI, including serum white blood cell count (WBC), C-reactive protein (CRP), interleukin 6 (IL-6), and procalcitonin (PCT) [3–5]. The ability of IL-6 to diagnosis post-operative SSI accurately has been studied repeatedly and appears to be superior to tumor necrosis factor (TNF)-α, CRP, and WBC [6].
Interleukin-6 is produced by activated macrophages, monocytes, and T-lymphocyte cells during the inflammatory response and induces production of acute phase proteins including CRP [7]. During an acute inflammatory reaction, IL-6 reaches maximal peak concentration and subsequent normalization faster than CRP [8], which may potentially provide a more sensitive indication of an inflammatory state [8]. Recent evidence has considered IL-6 as a valuable marker of infection after major surgery [9]. However, the significance of IL-6 and it ability to serve as a diagnostic marker specifically in the context of gastrointestinal fistulae remains to be determined.
The aim of this study was to analyze the utility of IL-6 as a screening tool for SSI in comparison with serum PCT, CRP, and WBC. We hypothesized that IL-6 would be more sensitive than other traditional inflammatory markers.
Patients and Methods
This study took place at the Jinling Hospital Gastrointestinal Fistulae Center, in the Department of Surgery in Nanjing, China. A total of 184 consecutive patients who underwent definitive operation for gastrointestinal fistula were enrolled prospectively from December 2015 to July 2017. Our study was approved by the Institutional Review Board of Jinling Hospital. All participants enrolled in the study were over the age of 18 years with radiologic imaging confirming a diagnosis of gastrointestinal fistula. Exclusion criteria included patients undergoing emergency surgery, existing clinical infection, chronic kidney disease, or hepatic insufficiency. Pre-operative mechanical bowel preparation and oral antibiotic agents, including levofloxacin, metronidazole, and voriconazole, were used routinely before surgery. Ceftazidime and ornidazole were given to gastrointestinal fistula patients by intravenous injection 30 minutes before surgery, and the antibiotic protocol (ceftazidime and ornidazole) would continue until three to four days after surgery.
Patient demographics recorded included gender, age, body mass index (BMI), etiology, and type of gastrointestinal fistulae, American Society of Anesthesiologists (ASA) class, operative time, estimated blood loss, types of fistulae and surgery, and post-operative complications. Peri-operative serum IL-6, WBC, PCT, and CRP concentrations were drawn. Blood of patients with gastrointestinal fistulae was drawn pre-operatively at 5:00
The primary outcome of interest in this study was the occurrence of SSI. Post-operative SSI was defined using the U.S. Centers for Disease Control and Prevention [10] criteria. The diagnosis was made if patients met one of the following requirements: purulent drainage from the surgical site; an organism isolated from a culture of fluid from the surgical site; physical examination demonstrating incisional pain, tenderness, localized swelling, redness, or heat and opening of the wound, or diagnosis of SSI by the surgeon or attending physician. In the present study, anastomotic leakage or intra-abdominal abscess after surgery was considered as an organ/space SSI.
Statistical analyses were performed using SPSS 19.0 statistical software (SPSS Inc., Chicago, IL). Categorical parameters were expressed as absolute numbers with percentages, and continuous data were presented as mean with standard deviation. Categorical parameters were compared by the χ2 test or Fisher exact test when appropriate. Student t-test (normal distribution) or Mann-Whitney U test (abnormal distribution) was used for comparisons between groups. Receiver operating characteristic (ROC) curve was used to performed effectiveness of WBC, PCT, CRP, and IL-6 concentrations in predicting the occurrence of SSI. All p values were two-sided, and p < 0.05 was considered statistically significant.
Results
Patient demographic data and overall post-operative complications for the 184 patients who underwent definitive fistula resection are summarized in Table 1 and Table 2. One hundred twenty-eight male and 56 female patients were enrolled, with a mean age of 44.5 years and a range from 18 to 78 years. Post-operative SSIs occurred in 49 patients (26.7%). Incisional SSIs were observed in 26 patients, deep incisional SSI in 9 patients, and organ/space SSI in 14 patients. Fifty-six patients (30.4%) underwent laparoscopic surgery and 128 (69.6%) patients underwent laparotomy. One-hundred thirty-six patients (73.9%) had a pre-operative diagnosis of only one gastrointestinal fistula whereas 40 patients (26.1%) had multiple fistulae. Patients with multiple gastrointestinal fistulae were more likely to develop SSI than those with a single fistula. As showed in Table 1, surgical patients with SSI had a longer length of hospital stay than the non-SSI group (36.2 ± 10.1 vs. 26.2 ± 8.7 d, p < 0.001).
Data are reported as number of patients (%) or mean ± SD.
ASA class = American Society of Anesthesiologists Physical Status Classification; BMI = body mass index; Non-SSI = non-surgical site infection; SSI = surgical site infection; SD = standard deviation.
There was no statistically significant difference in pre-operative concentrations of IL-6, PCT, CRP, or WBC between the SSI and non-SSI cohorts. Post-operatively, the inflammatory marker concentrations between patients with and without SSI were most pronounced for IL-6 and PCT.
Comparing patients with and without SSI, IL-6, PCT, and CRP were all higher on days one and three (Fig. 1, Supplementary Table S1 [see online supplementary material at http://www.liebertpub.com/sur]). White blood cell concentrations were similar at all times for patients with and without post-operative SSI. There were no statistical differences for any of the four biomarkers between the SSI and non-SSI groups on post-operative day seven (Fig. 1, Supplementary Table S1).

Inflammatory markers before surgery and on days one, three, and seven depending on the development of a post-operative SSI.
Receiver operating characteristic curve analysis demonstrated a reasonable diagnostic effectiveness for predicting the development of SSI using the inflammatory markers measured on post-operative day one and three (Figs. 2 and 3). The area under the curve (AUC) of IL-6 was 0.77 and 0.70 on post-operative day one and three, with a sensitivity of 85.7% and specificity of 63.9% on post-operative day one a sensitivity of 67.4% and specificity of 68.6% on post-operative day three. The AUC for PCT was 0.71 on post-operative day three with a sensitivity of 72.9% and specificity of 69.1%; CRP showed little diagnostic value in occurrence of SSI. In order to investigate whether the combination of IL-6 and PCT in clinical practice improved the prediction of SSIs, we performed binary logistic regression analysis including both parameters. However, combining IL-6 and PCT did not improve the diagnostic accuracy of SSI (data not shown).
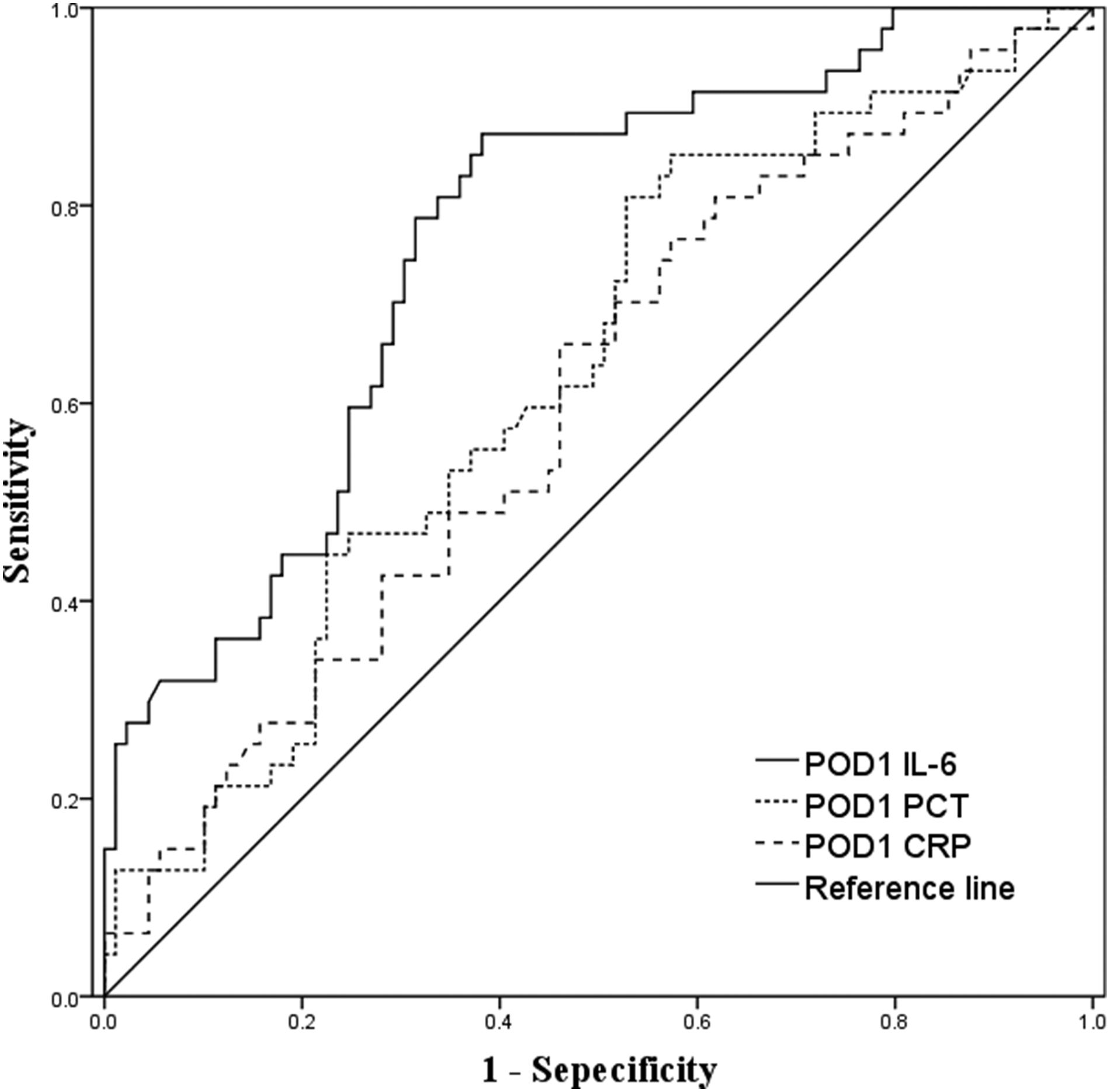
Receiver operating characteristic (ROC) curves for inflammatory markers on post-operative day one. Interleukin-6 has the best AUC (0.77), better than PCT and CRP (0.63 and 0.60, respectively). AUC = area under the curve; PCT = procalcitonin; CRP = C-reactive protein; POD = post-operative day.

Receiver operating characteristic (ROC) curves for biomarkers on post-operative day three. Interleukin-6 and PCT had better AUCs (0.70 and 0.71, respectively) than CRP (0.66). AUC = area under the curve; PCT = procalcitonin; CRP = C-reactive protein; POD = post-operative day.
Discussion
This study evaluated the diagnostic utility of perioperative WBC, serum CRP, PCT, and IL-6 as markers for SSI after definitive operation of gastrointestinal fistulae. The results demonstrate that patients with high IL-6 concentrations on post-operative day one had a nearly three-fold increased rate of SSI. Furthermore, concentrations of IL-6 allowed earlier risk stratification than concentrations of PCT or CRP.
It is widely accepted that gastrointestinal fistulae can achieve spontaneous closure through conservative therapy. However, patients with enteroatmospheric or multiple fistulae may eventually need definitive digestive tract reconstruction should medical treatment fail [7,11]. Hostile intra-operative conditions such as extensive adhesions, severe inflammation, and fecal contamination increase the risk of post-operative complications and SSI [12]. In this study, 69 patients had post-operative complications and 49 patients developed SSIs. Surgical patients with SSI have longer length of hospital stays and total cost of hospitalization than the non-SSI group. Therefore, it is plausible that early recognition of post-operative SSI may optimize patient outcomes and has the potential to reduce financial burden on an already overwhelmed system.
Utilizing inflammatory cytokine concentrations is one way to enhance the early detection of SSI [13]. C-reactive protein has been used to predict the occurrence of SSI before clinical symptoms become apparent. One meta-analysis evaluated CRP as a predictor of post-operative complications during the first five days after surgery. The ability of CRP to predict post-operative infectious complications was worse on day one (AUC = 0.64) and highest on day 4 (AUC = 0.84) [14]. In another meta-analysis involving more than 1,900 patients who underwent abdominal surgery, 577 (29.1%) had at least one post-operative complication and the serum CRP concentration on day four after surgery facilitated the reliable exclusion of post-operative infectious complications [15]. Silvestre el al. [16] conducted a prospective study to investigate the predictive value of CRP and PCT on early detection of SSI after elective colorectal surgery. They reported that CRP demonstrated superior predictive value in identifying patients with early SSI [16]. Another prospective study also obtained similar results, suggesting that CRP was more accurate than PCT and WBC in the detection of post-operative SSI after colorectal surgery and before clinical evidence of infection [17,18].
The ability of PCT to detect infectious complications is documented in the literature. Takakura et al. [19] conducted a prospective observational cohort study to determine the role of PCT in predicting SSI in patients undergoing elective colorectal cancer surgery. They suggested that PCT was a more reliable laboratory marker for the early diagnosis of SSI compared with CRP and WBC. Varetto et al. [20] also demonstrated that PCT could be considered a better biomarker of infectious complications compared with other routinely used parameters. More specifically, PCT was a more reliable marker on post-operative day three for intra-abdominal infection compared with CRP and WBC [19]. However, the diagnostic accuracy of PCT as a predictor of SSI in type 3 and 4 wounds requires further research.
Few studies have verified the diagnostic utility of IL-6 in predicting post-operative complications, specifically SSI after abdominal surgery. In one prospective study that investigated the role of IL-6 in post-operative morbidity in patients with gastric cancer [20], patients were assigned to two groups according to IL-6 concentration on the first post-operative day: high (>279 pg/mL) versus low (≤279 pg/mL). Twenty-four (24.2%) patients developed a post-operative infectious complication within 30 days of surgery. They suggested that a high IL-6 concentration was independently associated with an increased risk of post-operative infectious complications. Rettig el al. [8] studied prospectively 137 patients undergoing elective major abdominal surgery. Patients who developed a post-operative complication had higher concentrations of IL-6 on post-operative day one compared with patients without complications (432 pg/mL vs. 432 pg/mL, p < 0.01) and before changes were observed in concentrations of CRP [8]. Although the number of patients with SSI between the two groups showed no statistical significance, patients with an elevated IL-6 concentration on the first post-operative day had a three-fold increased rate of SSI than low IL-6 group (6 [11.5%] vs. 3 [3.8%]). Additionally, they found that the diagnostic value of IL-6 concentrations on post-operative day one in predicting post-operative complications improved when combined with CRP concentrations on post-operative day three. Another study investigated whether PCT and IL-6 concentrations could be used as early markers for subsequent post-operative septic complications in patients undergoing major surgery for cancer. The diagnostic accuracy of IL-6 in predicting post-operative sepsis was highest with a cutoff point of 310 pg/mL. However, CRP demonstrated lower sensitivity in the early post-operative period. The above findings suggest IL-6 can play an important role in the early detection of infectious complications (SSI) after surgery, because this cytokine is expressed systemically in the hours after surgery [21].
In our study, the overall rate of SSI was 26.7%, substantially higher than the data reported for other abdominal or colorectal operations. Most post-operative infectious complications (including SSI) become clinically evident after post-operative day five [13]. Therefore, it is plausible with use of these inflammatory markers, SSI can be detected earlier before clinical signs become evident. In the present study, both IL-6 and PCT became elevated on post-operative days one and three, which is consistent with previous studies [5,8]. It should be noted, however, that the serum concentrations of the inflammatory marker in our study were substantially higher than values reported previously in the literature. One possible explanation is that operations involving enteric fistulae contain higher colony counts of bacteria within a contaminated field. Because our study noted these pro-inflammatory markers were elevated in patients who ultimately developed an infectious complication as early as post-operative day one, SSI and other intra-abdominal infections may begin to develop much earlier than surgeons once believed. These findings highlight the possibility that a robust inflammatory response secondary to contaminated operations may play a role in the pathogenesis of SSI because of impaired healing [13]. This hypothesis is consistent with previous studies showing that high pre-operative values of CRP and leukocytosis are related to a higher risk of post-operative infections [2, 22].
Our study has several limitations. First, our study enrolled a relatively small cohort of patients, and a large-scale multi-center study is needed to confirm the accuracy of IL-6 in predicting SSI. Some variability in time from operation to collection of specimens, particularly on post-operative day one, was noted because procedures ended at various times through the day and specimens were collected routinely in the morning. Second, anesthetic agents have been demonstrated to influence the secretion of serum inflammatory markers [23]. The influence of anesthetics and of the choice of anesthetic management technique on the peri-operative inflammatory response may have clinical implications. In addition, the degree of surgical contamination differed widely and may have resulted in some variability in the concentrations of inflammatory markers. Future studies needs to control for the extent of contamination and the choice of anesthetic management during surgery.
Conclusion
Our study investigated an association between peri-operative inflammatory cytokines and post-operative SSI in patients with gastrointestinal fistulae after definitive operation. Interleukin-6 on post-operative days one and three had the highest diagnostic effectiveness in predicting the development of SSI. Nonetheless, further investigation is required to establish an ideal threshold concentration. Additionally, further investigation into the pathophysiology of elevated concentrations of IL-6 relative to SSI and the ability to modify these concentrations to prevent complications are needed.
Footnotes
Acknowledgment
This study was supported by grants from National Natural Science Foundation of China (81571881 and 81772052).
Author Disclosure Statement
All authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.