
Abstract
Abstract
Burns are a common form of trauma that account for more than 300,000 deaths each year worldwide. Survival rates have improved over the past decades because of improvements in nutritional and fluid support, burn wound care, and infection control practices. Death, however, remains unacceptably high. The primary cause of death has changed over the last decades from anoxic causes to now predominantly infections and sepsis. Sepsis and septic complications are not only major contributors to poor outcomes, but they further result in longer hospital stay and higher healthcare costs. Despite the importance of infections and sepsis, the diagnosis and prediction remain a major challenge. To date, no clear diagnostic criteria or predictive formula exist that can predict reliably the occurrence of sepsis and infections. This review will highlight and discuss current definitions and criteria for diagnosis as well as predictive biomarkers of sepsis in patients with burns. It will also present the diagnostic tools employed, such as procalcitonin, C-reactive protein, and cytokines. We will discuss the benefits and shortcomings of different treatment modalities in the context of sepsis prevention. Last, we identify new therapeutic strategies for sepsis prediction and present future considerations to prevent sepsis in patients with burns. Minimizing and preventing septic complications through early detection would significantly benefit patients and necessitate continued research to unravel new biomarkers and mechanisms. Subsequent studies need to take a fresh perspective and consider the implementation of patient-centered therapeutic strategies.
B
Sepsis is defined as the host's systemic inflammatory response to an infection with associated biochemical and physiologic abnormalities [8]. This includes fever, increased fluid requirements, and multi-organ dysfunction [7]. These complications increase risk of post-operative death and result in longer hospital stay and higher healthcare costs [9]. Minimizing and preventing septic complications through early detection would benefit patients. The current lack of diagnostic markers to predict sepsis, however, hinders the ability of clinicians to identify when sepsis occurs in burn patients and when to initiate antibiotic treatment.
This review will highlight the definition and criteria for diagnosis and prediction of sepsis in patients with burns. It will also identify the importance and occurrence of sepsis in patients with burns. We will present further the established diagnostic tools that are currently used and discuss the benefits and shortfalls of the different burn treatment modalities in the context of sepsis prevention. Last, we identify future considerations and introduce new therapeutic strategies to prevent sepsis in patients with burns.
Definition and Criteria for Predicting Sepsis in Patients with Burns
It is well documented that patients with burns are hyper-inflammatory, hyper-metabolic, and profoundly stressed leading to a catabolic response in organs and a plethora of dysfunction in nearly every organ system [10–12]. The failure and catabolic response of these organs is associated with poor outcomes. Specifically, one organ that has shifted into focus is the immune system. Over the last decade, various discoveries have been made in the area of the immune and inflammatory responses to burns and have delineated further why patients with burns are profoundly susceptible to not only bacterial but also to fungal and viral infections. The importance of this is that infections did not significantly contribute to morbidity or death in the 1970s and 1980s [13]. Because of multi-resistant organisms and invasive pathogens, however, infection and sepsis are now the main contributors to death [14–16].
At present, more than half of the patients with burns succumb to their injuries because of infections and sepsis [4]. Therefore, they play an essential role in the outcomes of patients with burns. Unfortunately, the current lack of prediction, definitions, and antibiotic regimens did not seem to really improve the outcomes. Therefore, new treatment modalities or even prediction of sepsis is essential to improve burn outcomes.
Another current challenge when treating thermally injured patients is that burn sepsis is not well defined. It is known that all patients with burns are colonized and that this population is at high risk for infections [17]. Infections and sepsis in burns mimic the symptoms of systemic inflammatory response syndrome (SIRS) and inflammation that accompanies the sterile inflammatory response to burns. Elevation of cytokines, resting energy expenditure (REE), and stress are ubiquitously present because of the nature of the injury [18]. Therefore, it is very challenging to define sepsis or infection in patients with burns.
In 2007, the American Burn Association (ABA) had a consensus conference led by Dr. Greenhalgh who published subsequently a consensus definition for sepsis [19]. This definition is based on various parameters and was updated recently to be more specific (Table 1). In 2013, Mann-Salinas et al. [20] published that the ABA definition was not accurate in predicting or identifying sepsis in patients with burns and came up with a different definition, which they found had higher sensitivity and specificity. These novel sepsis predictors were recommended by their group to be implemented. Both these formulas and predictions are associated with their own inherent challenges.
We recently conducted a study to compare the ABA definition, the Mann-Salinas definition, and the new Sepsis-3 consensus definition [8] applied to critically ill patients. In this study, we looked at our prospective, documented sepsis criteria in which the burn team identified sepsis on the basis of various clinical symptoms. In doing so, we are able to have a true sensitivity of sepsis by having a true positive event. When we applied our definition and then compared it with the sensitivity of the sepsis criteria from the ABA, Mann-Salinas, and Sepsis-3, we found that Sepsis-3 is superior by having 85% sensitivity over the ABA (60%) and Mann-Salinas (20%). This indicates the major advantage of Sepsis-3, even though Sepsis-3 was designed to target critically ill patients.
When looking at the ideal predictors, temperature variation, tachypnea, and tachycardia have the greatest predictive power according to the ABA definition. Extending this analysis to the other criteria, we found that use of vasoactive agents for Mann-Salinas, and respiratory rate over 22, altered mental status and systolic blood pressure under 100 for Sepsis-3 were the best predictors of sepsis. Therefore, it is an ongoing challenge to accurately diagnose sepsis. At present, however, we believe that the Sepsis-3 definition is superior to ABA and Mann-Salinas.
Importance of Sepsis in Burns
The importance of a well-defined definition and criteria for sepsis in burns is that sepsis or severe infections are the main contributors to death. In a study conducted by Williams et al. [21], the authors found that 55% of males and 54% of females are now dying because of sepsis and infections. The question really is, why is this? Numerous reports have ubiquitously demonstrated and delineated the pathophysiologic response to burns, which encompasses various changes in stress hormones, cytokines, metabolic alterations, and augmented organ response and function [10,12,18]. Collectively, these manifestations predispose patients toward the development of sepsis.
Metabolically, we know that patients with sepsis are more hypermetabolic than regular burn patients, who are hypermetabolic themselves. Profound or substantially elevated hypermetabolism then drives the catabolic response. Burn patients with sepsis have more than twice the level of catabolism than those with burns alone as measured by stabilized isotope infusions [11].
The authors also found that lean muscle mass is substantially lost with the presence of sepsis. The consequence of significant muscle loss is also well documented and has been described as follows: 10% muscle loss is associated with an impaired immune function leading to increased risk of death, 20% lean body loss results in decreased wound healing capacity and a 30% death rate, 30% lean body mass loss leads to pneumonia, pressure sores, and a 50% death, and a 40% loss in body mass results in death [22]. Therefore, sepsis is not only induced by the hypermetabolic state, but it also worsens the outcome of patients with burns.
Sepsis Occurrence in Burns
The incidence of sepsis in patients with burns varies anywhere from 3% to 30% for burns over 20% total body surface area (TBSA) [23,24]. The variability in occurrence supports the notion that the greatest challenge lies within the definition itself. It is not entirely clear when sepsis in burns peaks, what the modality is, or even which bacteria are contributing. Recent studies, however, indicate that sepsis has an onset as early as one week after burn, peaks during the second week, then descends beyond the third week with subsequent peaks occurring in some cases [25]. Interestingly, the early onset of sepsis within the first two weeks is usually associated with a greater survival rate, and the opposite is true for late onset [25,26]. Therefore, it seems evident that outcomes differ between early and late onset sepsis, and burn care providers would benefit from a predictor indicating patients at risk for sepsis and further differentiating the respective onset. We therefore will discuss diagnostic tools to predict sepsis in the following paragraphs.
Diagnostic Tools to Predict Sepsis: Established and Novel Approaches
Unfortunately, as described previously, burns and SIRS overlap substantially, creating challenges to differentiate whether the inflammation is because of the burn or because of bacteremia. At this time, there are various biomarkers that are now being studied to help identify sepsis and are summarized in Table 2. The following section will identify some of these biomarkers and further establish that none is suited ideally to predict sepsis.
PCT = procalcitonin; CRP = C-reactive protein; IL-6 = interleukin-6; mHLA-DR = monocyte human leukocyte antigen DR; TNF-α = tumor necrosis factor α; TLR-9 = Toll-like receptor-9; PMN CD11b = polymorphonuclear cluster of differentiation 11b.
C-reactive protein (CRP)
A biomarker that has been investigated extensively and utilized clinically is C-reactive protein (CRP). CRP is a well-known marker of inflammation, and the elevated proportion of interleukin (IL)-6 after burn stimulates its production in the liver [27,28]. Its acute phase properties have established CRP as a good predictor of sepsis [29]. Follow-up studies in severely burned patients, however, have shown that, in fact, it is not a good predictor of infection or sepsis [30]. Therefore, CRP in patients with burns serves as an adjunct in situations of limited information but is not a very reliable predictor in burns.
Procalcitonin (PCT)
Procalcitonin (PCT) entered the clinical focus because of the inability of CRP to predict sepsis in patients with burns effectively. Smaller studies demonstrated that PCT could predict sepsis at later time points using its temporal changes and have indicated that it can somewhat predict sepsis with weak power [7]. Other studies have demonstrated no difference in PCT concentrations between confirmed and unconfirmed cases of sepsis [31]. A meta-analysis, however, conducted by Cabral et al. [32] indicated that PCT studies have increased and emerged to indicate accurately and time-effectively the presence of infection in patients with burns. These findings were confirmed in a subsequent, retrospective study conducted by the same authors and further proposed to be implemented by burn units as a biomarker for antimicrobial stewardship [33]. Collectively, these conflicting reports indicate that PCT may not be an ideal biomarker of sepsis prediction.
Cytokines
The hope for prospectively predicting sepsis in patients with burns has revolved around using traditional immune modulators—namely, cytokines. Major players in the cytokine detection area have included IL-6, IL-10, monocyte chemoattractant protein (MCP)-1, IL-1, tumor necrosis factor (TNF)-α and FMS-like tyrosine kinase 3 ligand (FLT-3L) [26,34]. These early markers are associated with the initial inflammatory (acute phase) response after burn.
Even these common immune mediators that are consistently responsive after thermal injury have limitations and restrictions in terms of single time point measurement, however. Two of the most controversial include IL-6 and TNF-α, which consistently generate conflicting reports in the realm of sepsis prediction [26,35]. Despite showing some promise in identifying non-survivors in patients with burns [34,36], cytokines are very limited in the capacity to consistently predict sepsis, and time courses are paramount. There are various new biomarkers that are available, and the subsequent section will discuss a few.
Novel biomarkers
A recent study by Hampson et al. [37] investigating neutrophil dysfunction, immature granulocytes, and cell-free deoxyribonucleic acid found that these are able to serve as early biomarkers of sepsis in patients with burns. Using the neutrophil extracellular trap (NET), the authors found that prolonged neutrophil dysfunction was present in patients with burns and to a greater extent in patients with sepsis. This elegant study successfully delineated a biomarker profile able to predict sepsis with high sensitivity and specificity.
Another approach that was investigated recently was the use of genomics in identifying patients susceptible to multiple infections. Yan et al. [38] conducted a prospective cohort study of 459 patients with burns to look at the genomic pattern and found that the genomic and clinical models were highly predictive of multiple infection episodes with a sensitivity of 0.9 and specificity 0.83. They were able to delineate that hypersusceptible patients had early alterations in immune signaling pathways and chromatin remodeling and epigenetic modulation. Moving forward, this approach may provide new therapeutic approaches to identify patients susceptible to sepsis using similar genomic signatures.
Another important acute phase immune mediator of inflammation of interest is the nucleotide-binding domain, leucine-rich family (NLR), pyrin-containing 3 (NLRP3) inflammasome. On exposure to an invading pathogen, the NLRP3 inflammasome activates and results in the maturation and production of IL-1β and IL-18 [39]. The major function of the NLRP3 is to perform cytoplasmic detection of pathogen- (PAMP) and danger- (DAMP) associated molecular patterns [40]. Previous work from our group has demonstrated that the NLRP3 inflammasome (an acute phase mediator and cytoplasmic surveillance sentinel) has increased expression in white adipose tissue of adult burned patients [40]. Subsequent studies also demonstrated that the NLRP3 inflammasome increases in gene expression as a function of increasing burn injury severity [41].
Extending these findings, we investigated recently whether we can utilize the NLRP3 inflammasome and its major byproducts to delineate patients susceptible to sepsis. Flow cytometric analysis of excised white adipose tissue of burned patients was used to determine the proportion of macrophage (CD14hi CD16lo cells) and IL-1β (CD14+ IL-1β+ cells) production [25]. We found that adult burned patients with high levels of pro-inflammatory IL-1β and decreased macrophages at the site of injury are susceptible to sepsis. As recapitulated in Figure 1, the left panel represents an adequate response in non-sepsis burn patients characterized by several macrophages producing IL-1β. Compared with the right panel, patients with burns who are susceptible to sepsis will mount an insufficient immune response that includes a small portion of macrophages producing large amounts of IL-1β. This scenario will result eventually in immune exhaustion and sepsis onset. Unlike other approaches, the Septic Predictor Index prospectively identifies patients susceptible to injury within 96 hours post-injury using a platform that does not rely on systemic biomarkers of undecipherable origin.
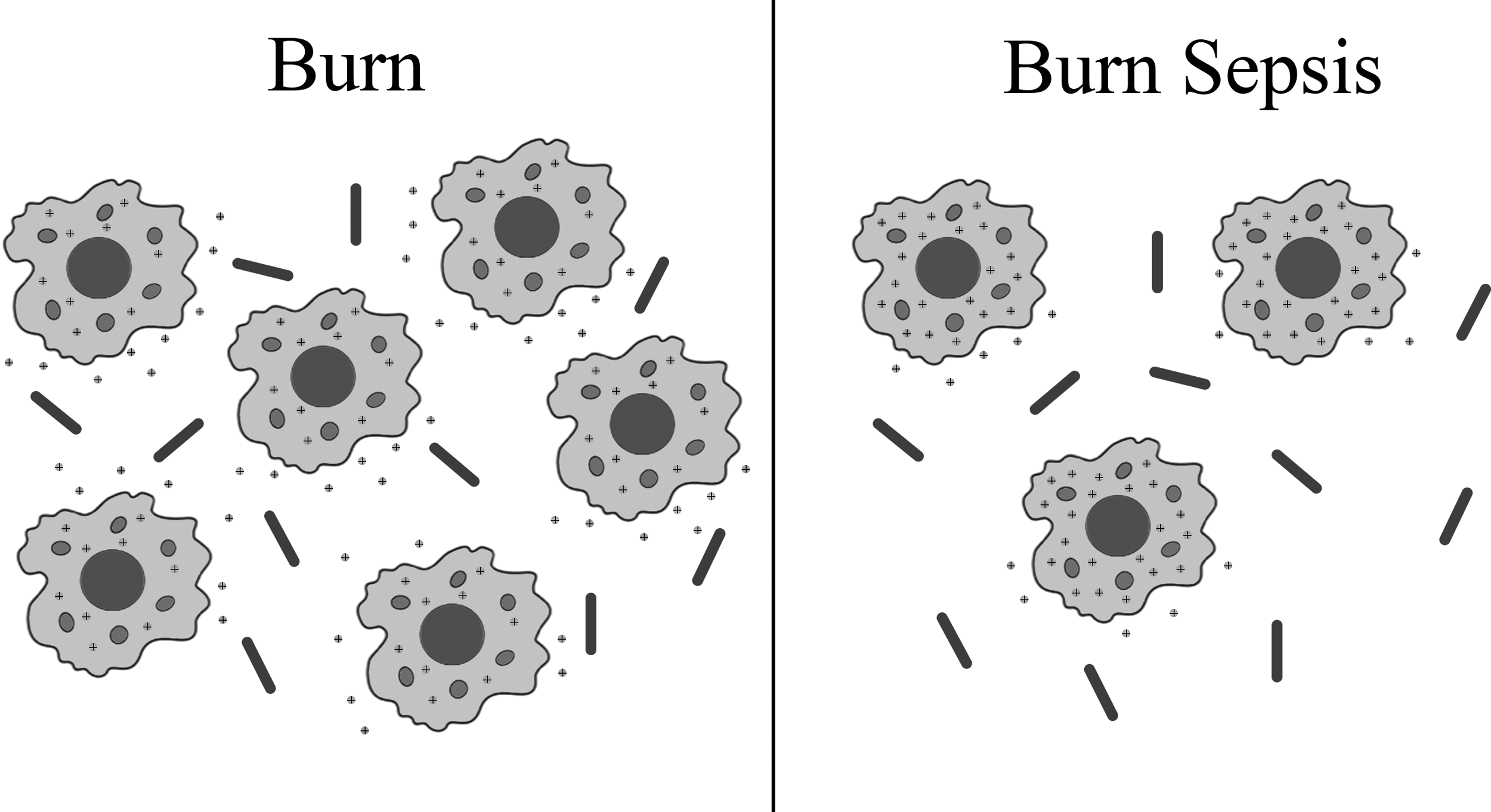
Comparing the immune response to pathogenic challenge in non-septic and septic burn patients.
Treatment
Hydrotherapy
Hydrotherapy, which refers to water treatment using tub immersion or warm water showers, is implemented in burn management for early wound cleansing, rehabilitation, and scar treatment [42]. Use of hydrotherapy, however, has been a controversial topic. There are several advantages to hydrotherapy treatment, in particular when used in conjunction with physiotherapy. In terms of wound healing and scar prevention, it has been shown to enhance tissue sloughing and wound debridement [43]. It allows for draining of pus and cleaning of wound surfaces, while promoting healthy tissue formation and healing via improved circulation [43]. In addition, patients can perform certain movements and exercises under the guidance of a physiotherapist.
While it is an adjuvant to burn treatment, there are concerns that this procedure may increase the spread of infection [42]. Possible sources of transmission include person-to-person or via fomites. The common equipment employed, such as tubs and spray tables, are difficult to clean between patient uses, and organisms such as Pseudomonas aeruginosa have the ability to form resistant glycocalyx biofilms [44], thus allowing bacterial organisms to survive in water pipes, drains, and shower tables despite use of disinfectants, which is compounded by the fact that it is difficult to ensure adequate decontamination. Ideally, using sterile water, bathing once daily, and maintaining sterile conditions could minimize the risk of contamination, enabling safe implementation of this technique. Because of the increased time needed for dressing changes, higher costs, and potential to spread infection, however, burn centers limit use of hydrotherapy [45]. The latter is an important consideration, and dressing changes and antimicrobials are critical components of burn wound management.
Soaks/topical antimicrobials
Initial management of burn injuries includes cleansing and debridement, gauze or special dressings such as hydrocolloid or silicone-coated polyamide, and topical antimicrobials to microbes such as P. aeruginosa and Staphylococcus aureus [46]. There are several different options for topical antimicrobials chosen based on yeast, fungal, and gram-positive and gram-negative bacterial coverage. Widespread application of topical agents based on initial positive burn wound cultures reduces the microbial load and infection risk [47].
Because of the increased risk of bacterial resistance to antibiotic agents, topical silver preparations are used commonly as an alternative for prophylaxis and management of ulcers and wounds [47]. Silver sulfadiazine (SSD), which is a combination of silver nitrate and the antibiotic sodium sulfadiazine, is a common agent that has gram-positive, gram-negative, and fungal coverage. An alternative option is silver-based dressings such as Acticoat, which has been shown to result in less wound infections when compared with silver nitrate and SSD and is effective against methicillin-resistant S. aureus (MRSA) and vancomycin-resistant enterococci (VRE) [47]. One of the challenges of these antimicrobial agents, however, is poor deep tissue penetration and delayed wound re-epithelialization [48].
Topical antibiotics, selected based on wound culture results, are another option. These include mafenide acetate, which is effective against gram-negative bacteria, particularly P. aeruginosa. When treating patients with antibiotic-resistant bacteria, alternative options such as Dakin solution (0.25% or 0.5% sodium hypochlorite) may also be used. Dakin solution is broad-spectrum and cost-effective; however, it is toxic to fibroblasts and may impair wound healing, similar to the other aforementioned agents [48]. Despite these drawbacks, widespread use of topical agents could improve outcomes by reducing microbial load at the wound surface. Burn eschar avascularity may restrict distribution of systemic agents, highlighting the importance of topical agents in infection control [47].
Systemic antimicrobials
There are several guidelines for antibiotic therapy in wound management that depend on factors such as length of admission, microbial resistance, and suspected organisms. Initially, burn wounds are colonized primarily with gram-positive microbes, which are replaced by gram-negative, antibiotic-susceptible organisms [49]. Despite topical antimicrobial treatment, a delay in wound closure can result in subsequent infection necessitating broad-spectrum agents, which can lead to colonization by yeast, fungi, or antibiotic-resistant bacteria [50]. This demonstrates the importance of using appropriate antimicrobial agents when treating patients with infected burn wounds.
While systemic treatment should be directed by burn wound culture results, there are different guidelines for empiric antibiotic treatment. Generally, initial gram-positive infection involves organisms such as Streptococcus and Staphylococcus species, and early gram-negative infections are attributed to microbes such as Escherichia coli, Haemophilus influenza, and Klebsiella pneumonia [50]. Based on this, burned patients with sepsis in the early phase of admission are treated with a regimen of natural penicillins, such as penicillin G, aminopenicillins such as amoxicillin, or pencillinase-resistant antibiotic agents such as methicillin or cloxacillin. These antimicrobial agents function against gram-positive staphylococci and streptococci strains. Also, ceftriaxone and other third-generation cephalosporins can be administered to manage early gram-negative infections [51]. Most common pathogens in the late phase of patient admission (>5 days) are S. aureus, and P. aeuruginosa, which are managed with piperacillin-tazobactam and vancomycin or carbapenems such as meropenem for resistant organisms [52].
While prolonged use of these systemic antibiotics may increase organism resistance, short duration of administration and prudent selection based on burn wound culture and antibiotic susceptibility could mitigate this effect [49]. Previous work by Ergun et al. [53] on the benefit of systemic antibiotic prophylaxis demonstrated no significant decrease in burn wound infection rates. Based on these results and the increased risk of antibiotic resistance, systemic antibiotic treatment should be considered carefully in patients with burns.
Gut decontamination
Previous reports have suggested that the gut, a site of potentially pathogenic organisms, has a significant role in progression to multiple organ dysfunction after burns [54]. Selective gut decontamination (SGD) was used initially to prevent ventilator-associated pneumonia in critically ill patients. It was also an effective strategy to prevent aerobic gram-negative enteric bacilli infection, reducing death in severely ill patients [51]. Gut decontamination involves a course of parenteral antibiotic agents, such as cefotaxime, with the addition of a non-absorbable antimicrobial oral paste and digestive solution (e.g., polymyxin E, tobramycin, amphotericin B, or nystatin). The basis of this procedure is to eradicate oropharyngeal and gastrointestinal micro-organisms that are potentially pathogenic. The SGD has been shown to reduce infection and death without inducing microbial resistance [55].
Recent work by López-Rodriguez et al. [56] demonstrated that treatment of patients with TBSA greater than 20% decreased death by reducing rates of endogenous infections. This was attributed to decreased hematologic and respiratory dysfunction. Despite its well-supported benefits in critically ill patients, there are several drawbacks to using SGD as an infection prophylaxis in severely burned patients. Certain studies have shown no significant difference in the inflammatory response, rates of colonization or infection between treatment and placebo groups [57]. The discrepancy that exists in the literature may be a result of SGD treatment protocol adherence (or implementation); for example, using pre-operative antimicrobial prophylaxis, not administering systemic antibiotic agents, or the addition of an agent that covers MRSA, which is not typically covered in SGD. Overall consensus, however, indicates that SGD reduces rates of multiple organ dysfunction, often seen in burned patients in the setting of infection, with a survival benefit after treatment [58].
Conclusion
Prediction and diagnosis of sepsis or infection in burns represents an ongoing challenge. There are various studies and methods to detect or identify sepsis in patients with burns. None of these approaches, however, have reached clinical applicability. Various biomarkers have been studied, and the ongoing discovery of conflicting findings demonstrates a persistent challenge. Despite this uncertainty, what is known and consistent among these studies is the outcome, which is that sepsis and infection are the major contributors to death. Therefore, this scientific enterprise is of great importance to improve outcomes of patients with burns. Future work needs to take a fresh perspective and consider the implementation of innate immune cell priming and therapy to overcome pathogenic burden, which has shown promise recently in targeting tumors and differentially interacting to infection [59,60].
Based on current data and analyses, we believe it is very challenging to identify sepsis correctly based on definitions. To us, the best approach is for the burn team to assess sepsis and severe infections on a daily basis and document sepsis prospectively based on substantial clinical markers at that time. If a definition has to be applied for analysis or research purposes, however, Sepsis-3 appears to be the better definition to identify sepsis.
In terms of prediction, the data clearly demonstrate a lack of a reliable predictor for sepsis in patients with burns. The CRP seems ineffective, PCT has a mild predictive value, and cytokines are inconsistent. Newer biochemical tools and function may have a predictive power, but these need to be investigated further. Therefore, the conclusion is that sepsis is the major contributor to death in patients with burns, and identification, definition, and prediction of sepsis are all lacking power and efficacy. This makes sepsis treatment and hence the improvement of burn outcomes an ongoing challenge.
Footnotes
Author Disclosure Statement
No competing financial interests exist.