
Abstract
Abstract
Purpose:
Different biomarkers are useful in diagnosing infections. The aim of this work was to clarify the relation between different inflammatory biomarkers (white blood cell [WBC] count, C-reactive protein [CRP], procalcitonin [PCT], and C-reactive protein-to-albumin ratio [CAR]) and early infectious complications after colorectal surgery.
Methods:
This prospective single-center cohort study included 130 patients undergoing elective colorectal surgery. The WBC count, CRP, and PCT were measured at post-operative day one (POD1) and POD3 and albumin on POD3.
Results:
Patients with surgical site infections (SSI) exhibited significantly higher CRP concentrations on POD1 and CRP and CAR on POD3 than did patients without SSI. According to receiver operating characteristic analysis, the CRP concentration on POD1 and the CRP and CAR on POD3 showed the highest area under the curve (AUC) for predicting SSI (AUC 0.639, 0.736, and 0.729, respectively). Multivariable logistic regression analysis showed that CRP on POD1 and CRP and CAR on POD3 were independent predictors of SSI (odds ratio 7.355, 7.605, and 8.337, respectively).
Conclusions:
The CRP concentration on PO1 and CRP and CAR on POD3 can positively identify patients at low risk of SSI. They can be used as a prognostic tool to predict an uneventful post-operative period and therefore have been incorporate into our discharge criteria after elective colorectal resection, improving clinical decision-making.
R
Despite the importance of early diagnosis of infections in order to initiate the treatment as soon as possible, their diagnosis usually is difficult, delaying their resolution. Therefore, there is a clear necessity for early sensitive and specific markers for post-operative infections [2]. Several biomarkers of infection, namely white blood cell (WBC) count and C-reactive protein (CRP) and procalcitonin (PCT) concentrations, have proved useful in the diagnosis of infection in different clinical settings as well as in the assessment of its response to antibiotic therapy [2–4]. Also, a low serum albumin concentration is associated with post-operative complications [5, 6].
In the presence of inflammation, the liver synthesizes an acute-phase reactant called CRP, which can be found in the blood as a result of stimulation by interleukin-6 and tumor necrosis factor-alfa [7]. It probably plays an important role in innate immunity by assisting complement binding to foreign and damaged cells and enhancing phagocytosis by macrophages, thus acting as an early defense against infection [8]. Production of CRP is part of a nonspecific acute-phase response to most forms of infection, tissue damage, inflammation, and malignant disease [7].
Also, PCT is the inactive 116-amino-acid pro-peptide of the hormone calcitonin. Patients with sepsis or less severe bacterial and fungal infectiond show an increase in the concentration of PCT [9]. The concentration is a valuable marker for inflammation, and the central role of PCT as an early and reliable diagnostic and prognostic tool in contexts such as infection and sepsis and both infectious and non-infectious systemic inflammatory response syndrome (SIRS) has been demonstrated [9].
An early decrease in the post-operative serum albumin concentration is associated with adverse clinical outcomes and results from surgical insult [10]. The greater capillary leakage of albumin is one of the characteristics of SIRS, leading to a low plasma albumin concentration in patients undergoing major abdominal surgery [11].
The WBC count, CRP, and PCT have been studied by several authors as early predictors of infectious complications. However, there still is no consensus regarding the diagnostic accuracy of each one for early detection of complications in patients undergoing colorectal surgery [3,9,12,13]. However, the CRP-to-albumin ratio (CAR) has received almost no studies to determine its diagnostic accuracy for post-operative complications in patients undergoing colorectal surgery [5]. The aim of this work was to clarify the relation between different inflammatory biomarkers (WBC, CRP, PCT, and CAR) and early infectious complications of colorectal surgery.
Patients and Methods
Study design and selection of participants
This study was approved by the local ethics committee. It was a prospective single-center cohort study that included all patients with colorectal adenocarcinoma who underwent elective surgery in our institution from August 2015 to August 2016. Exclusion criteria were evidence of metastasis before or at surgery, synchronous tumors, and absence of colorectal adenocarcinoma in the surgical specimen.
Data collection
The range of data collected included baseline characteristics such as age and sex, co-morbidities such as arterial hypertension and dyslipidemia, and type of surgery (laparoscopy vs laparotomy). The laboratory data collected were WBC count, CRP (mg/L), and PCT (ng/mL) on post-operative day (POD) 1 and POD3 and albumin (g/dL) on POD 3.
All post-operative infectious complications were recorded according to the Surgical Site Infection (SSIs) Guidelines and were classified as superficial incisional (involves only skin and subcutaneous tissue of the incision), deep incisional (involves deep soft tissues of the incision such as fascial and muscle layers), and organ/space (involves any part of the body deeper than the fascial/muscle layers that is opened or manipulated during the operative procedure). In this study, SSIs were all confirmed by the same attending physician. The follow-up period was 30 days after surgery.
Data analysis
Statistical analysis was performed using the 2016 Statistical Package for the Social Science Program (SPSS) version 24 (IBM Corporation, Armonk, NY). Descriptive statistics are presented as frequencies (n) and percentages (%) for categorical variables and as means (M) and standard deviations (SD) for quantitative variables, after checking to see if the asymmetry coefficient fell inside the [−2; 2] interval. Univariable analysis between laboratory data and SSI were performed with the independent-sample t-test.
Receiving operator characteristic (ROC) curves were built in order to assess the sensitivity and specificity of the biomarkers WBC count, CRP, and PCT one and three days after surgery. The CAR was calculated three days after surgery. Precision was calculated as the area under the curve (AUC) (null hypothesis—H0—was AUC = 0.5). We also calculated the positive and negative predictive values for the significant early biomarkers.
Finally, adjusted odds ratios (ORs) were determined for the significant early biomarkers using adjusted unconditional logistic regression. The confounders tested were sex, age, arterial hypertension, type II diabetes mellitus, dyslipidemia, and surgical approach. Significant results were considered as p < 0.05.
This work has been reported in line with the STROCSS criteria [14].
Results
Study population and baseline characteristics
From August 2015 to August 2016, a total of 138 patients were enrolled, and eight patients were excluded, four because of high-grade dysplasia and one each for serrated adenoma, lipoma, metastasis at surgery, and adenocarcinoma of the appendix. There were 81 men (62.3%) and 49 women with a mean age of 67.83 years (SD 13.07) and a median age of 68.5 years (range 34–91 years). The rest of the baseline characteristics, surgery and treatment performed, and pathologic characteristics of the tumor are summarized in Table 1. There were 26 patients (20.0%) who had detectable SSIs. Of these, 12 patients (9.2% of the total series) had superficial incisional SSI, 1 (0.8%) had deep incisional SSI, and 13 (10.0%) had organ/space SSI.
Anastomotic leak occurred in 10 of 121 patients with anastomoses.
Predictive clinical features
To assess the utility of clinical features for the early assessment of SSIs, analysis of the WBC count, CRP concentration (mg/L), and PCT concentration (ng/mL) was made on PODs 1 and 3, whereas the concentration of albumin (g/dL) was measured only on POD 3 (Table 2). On POD1, patients with SSI exhibited significantly higher CRP concentrations than did those without SSI (p < 0.05). On POD3, patients with SSI exhibited higher CRP concentrations and CAR values than did those in the non-SSI group (p < 0.05). There were no statistically significant differences between the two groups in WBC count or PCT on PODs 1 and 3. The surgical approach (laparoscopy vs. laparotomy) was associated with a statistical difference in the development of SSI (p = 0.035) and exhibited differences in the laboratory values of the inflammatory markers (Table 3).
To compare each marker and to determine the optimum cut-off for SSI diagnosis, ROC analysis was performed. On POD1, CRP was the most reliable predictor of SSI (cut-off value 73 mg/L; AUC 0.639). On POD3, the CAR was a significant predictor of SSI (cut-off value 43; AUC 0.736) as was CRP (cut-off value 123 mg/L; AUC 0.729) (Fig. 1).
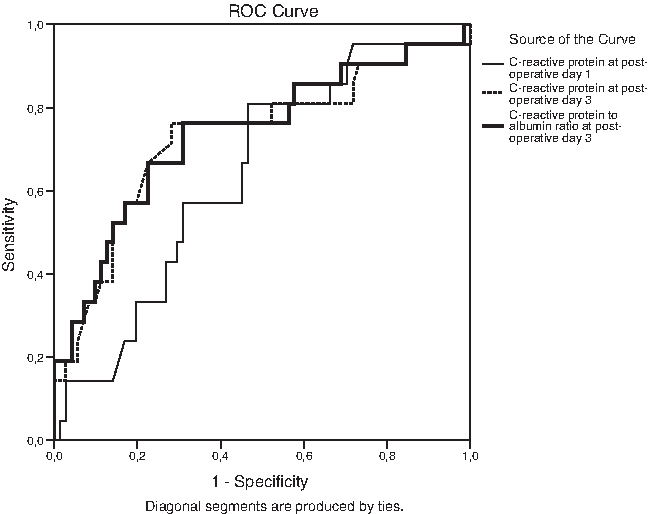
Receiver operating characteristics curves of C-reactive protein (CRP) on POD1 and CRP and C-reactive protein-to-albumin ratio (CAR) on POD3.
The optimum cut-off and the corresponding sensitivity, specificity, and positive and negative predictive values are summarized in Table 4.
CAR = C-reactive protein-to-albumin ratio; CRP = C-reactive protein; POD = post-operative day.
Risk and predictive factors for SSI after colorectal cancer surgery
Adjusted logistic regressions showed significant results for CRP on POD1 and CRP and CAR on POD3 for the risk of infection. For CRP on POD1, our proposed cut-off value was associated with a risk 7.355 times higher for patients with SSI (odds ratio [OR] 7.355; 95% confidence interval [CI] 12.076–26.066; p = 0.002). For CRP on POD3, our proposed cut-off was associated with a risk 7.605 times higher for patients with SSI (OR 7.605; 95% CI 2.313–25.007; p = 0.001). For CAR, our proposed cut-off showed a risk 8.337 times higher for patients with SSI (OR 8.337; 95% CI 2.202–20.168; p = 0.001) (Table 5).
CI = confidence interval; OR = odds ratio; POD = post-operative day.
Discussion
After colorectal cancer surgery, the most significant source of morbidity and delay of discharge is infectious complications. Through the use of newer biochemical markers (CPR and PCT), it may be possible to predict accurately a group of patients at higher risk of poor outcome because of infections [8] and, at the same time, help to identify patients for safe early discharge [7].
For many surgeons, the early identification of SSI is still a challenge. In the period after elective colorectal surgery, SSI can lead to prolonged hospital stays, increased morbidity and mortality rates, and higher medical costs [5]. Despite the combined evaluation of clinical, laboratory, and radiologic findings, early diagnosis of SSI cannot be made reliably by any known individual feature or even by experienced clinical judgment [9].
When most studies try to find a predictive factor for infection, few have attempted to identify predictors of an uneventful post-operative course in terms of infection. But such information can be valuable in developing algorithms for discharge. This study demonstrated an increase in CRP on POD1 and in CRP and CAR on POD3 with significant differences between patients with and without complications. The ROC curve analysis showed that the CRP concentration on POD1 and CRP and CAR on POD3 predict the development of post-operative infectious complications. In adjusted logistic regressions, both CRP on POD1 and CRP and CAR on POD3 were identified as independent predictors of SSI.
Our study shows that using a cut-off value for CRP of 73 mg/L on POD1 may have sensitivity and specificity adequate to be used for clinical decision making, but the most important finding is that, in our population, CRP ≤73 mg/L on POD1 predicted an uncomplicated course in 91.5% of patients. Although most studies agree that CRP on PO1 is influenced by surgical insult [2,8,15] and its post-operative peak occurs at 48 hours after surgery [2], the lack of increase in the CRP concentration on the first post-operative day is a predictor of a complication-free post-operative period.
At POD3, most studies suggest that CRP is a predictor of infectious complications [2, 7,15]. In our study, as on POD1, CRP at a cut-off 123 mg/L on POD3 had a high negative predictive value (91.2%).
Similarly, we studied CAR, which is based on circulating concentrations of two acute-phase proteins, CRP and albumin, which are associated with inflammation caused by surgical insult. In this way, we concluded that almost all patients with CAR ≤43 on POD3 will not develop an SSI (negative predictive value 90.7%).
The research on CAR is still in development. Ge et al. [5] found that patients with CAR >2.2 on POD3 should be monitored intensively for early detection of post-operative complications. Shibutani et al. [16] found pre-operative CAR to be a useful prognostic marker in patients with colorectal cancer undergoing potentially curative surgery. In patients with sepsis, Ranzani et al. [17] reported that residual inflammation at ICU discharge, as assessed by CAR, was an independent risk factor for a poor outcome.
Elevated WBC count is a nonspecific inflammatory marker and one of the SIRS criteria. Therefore, it is not surprising that the count had a poor diagnostic performance for infection in patients in the intensive care unit and post-operatively [15]. However, some studies have reported a late increase in WBC counts in patients with infectious complications of colorectal surgery, correlating with the clinical diagnosis of complications [15]. We could have missed this late increase, as we assessed inflammatory markers only on PODs 1 and 3. Furthermore, in our study, PCT failed as a predictor of early post-operative infection on both PODs 1 and 3. We could not find a correlation between SSI and the PCT concentration. Silvestre et al. [2] recently described finding that in critically ill surgical patients, an increase in PCT did not predict complications.
Our results show that the surgical approach influences the development of SSI and the mean values of inflammatory markers are different statistically according to the approach by laparoscopy or laparotomy. However, the clinical relevance of these findings cannot be assessed from these data because our study was not designed to evaluate the influence of the surgical approach on SSI and inflammatory markers. The study design did not assign patients to the laparotomy or laparoscopy groups at baseline. Therefore, these groups are not equally distributed, for example in terms of patients' age, and cannot be compared.
Finally, there are important limitations we should make note of. First, with an observational design and moderate sample size, this study requires validation in large-scale prospective multi-center trials. Second, because of the small sample, we combined patients with organ/space SSIs with those with incisional SSIs and analyzed them as one group. Although there are significant differences in CRP on POD1 and CRP and CAR on POD3 in patients with and without SSI, further studies are necessary to investigate the usefulness of those markers.
In conclusion, CRP on PO1 and CRP and CAR on POD3 can identify patients at low risk of SSI. Our study suggests that they can be used as a prognostic tool to forecast an uneventful post-operative period. They have been incorporate into our fast-track discharge criteria after elective colorectal resection, improving clinical decision-making.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest with regard to this manuscript.