
Abstract
Abstract
Background:
The healthcare environment is a potential source of microbial pathogens, which may promote infectious cross-transmission. Terminal automated cleaning methods such as hydrogen peroxide systems have proven to be more successful than manual techniques. The aim of this study was to evaluate the effectiveness of an automated aerosolized hydrogen peroxide/silver cations dry-mist system. The goal was to prevent microbial transmission to patients in a clinical setting after two cases of sepsis caused by multi-drug resistant Acinetobacter baumannii had been diagnosed in a burn unit that relied on manual cleaning techniques.
Materials and Methods:
Samples were taken from room surfaces before and after the dry-mist system cycle, which was used to disinfect all burn unit rooms after patient discharge. The disinfection effectiveness was assessed using contact plate cultures, with microbial growth represented as the total number of colony forming units per square centimeter (CFUs/cm2).
Results:
No positive cultures from surface samples were observed after the intervention with the dry-mist system. Specifically, no further Acinetobacter baumannii growth was detected.
Conclusions:
Our results support the use of the hydrogen peroxide/silver cations dry-mist system as an adjunct to standard manual cleaning and disinfection protocols used in the healthcare environment because of its broad-spectrum and high antimicrobial activity. This system may be a valuable option to consider, particularly in the control of microbial outbreaks.
D
Recently, two consecutive patients were diagnosed with sepsis by MDR Acinetobacter baumannii at the burn unit of a tertiary care university hospital. In spite of the stringent local protocol for manual environmental decontamination and hand hygiene, these cases occurred within a short period of time, with both isolates displaying a similar phenotype. Acinetobacter baumannii infections have been increasing in number in many hospitals because of its ability to persist in the healthcare environment [2], its high resilience to standard decontamination protocols [9], and to the ease in developing multi-drug resistance [10], therefore rendering outbreaks difficult to contain. The aim of this study was to evaluate the disinfection effectiveness of an automated aerosolized hydrogen peroxide/silver cations dry-mist system in order to prevent further microbial transmission to patients in this burn unit.
Material and Methods
Settings
The study involved all five isolation rooms of the burn unit of a tertiary care university hospital. Each room has intensive care capability with its own laminar airflow system and high-efficiency particulate air filters. The routine terminal decontamination standard procedure of this unit involved manual techniques. The room and equipment surfaces were disinfected with undiluted Anios D.D.S.H.® (quaternary ammonia propionate; Laboratories Anios, Lille-Hellemmes, France) and the floor with 0.25% diluted Surfanios Citron® (N-(3-aminopropyl)-N-dodecylopropane-1,3-diamine; Laboratories Anios). No equipment was removed routinely from the room during the procedure.
The Glosair™ 400 system (Advanced Sterilization Products, Irvine, CA) is an automated dry-mist generator that uses the Glosair™ 400 cartridge, diffusing hydrogen peroxide and silver cations as small-size particles (approximately 10 mcm in diameter). These droplets circulate freely in the air as a dry aerosol. The Glosair™ 400 cartridge is composed of hydrogen peroxide 5%, phosphoric acid <50 ppm, silver cations <50 ppm, gum arabica <1 ppm and biosmotic water 95%.
Intervention
The dry-mist system was used once in each burn unit room. The disinfection cycle occurred after patient discharge and immediately after the routine standard terminal decontamination procedures. Because burn unit patients typically have prolonged lengths of stay, 32 days were needed to complete one disinfection cycle per room.
For each cycle, the dry-mist system was placed in a corner; equipment was removed and the rooms were closed. The spraying times and the volume of disinfectant were used as recommended by the manufacturer. Diffusion times were calculated according to each room size in order to reach the target concentrations, with an additional period of room inaccessibility as recommended. The complete cycle took approximately two hours.
Monitoring of microbial growth
Samples were always taken from surfaces after the routine standard terminal decontamination procedures: before and immediately after the intervention with the dry-mist system. Samples were taken from the bed rails, monitor touch screen, television remote control, room floor, and bathroom handrails using contact plates. Brain heart infusion agar (Difco Laboratories, Sparks, MD) and Dichloran Glycerol 18 agar (Difco Laboratories) culture medium plates were used for surface sampling. The agar plates were incubated at 25°C and 35°C for five days. Sampling was always performed in duplicate. The total number of microbial species recovered from surfaces before and after the intervention (represented as colony forming units per cubic centimeter [CFUs/cm2]) was used to assess the antimicrobial effectiveness of the dry-mist system.
Clinical isolates from burn patients were monitored successively for species and antimicrobial susceptibility. Microbial identification and susceptibility testing was performed with VITEK 2 system (bioMérieux, Marcy L'Etoile, France).
Results
Before the intervention
The total number of bacteria and molds (CFUs/cm2) recovered in contact plates after the application of the standard disinfection protocol is shown in Figure 1. No yeasts were grown. Of particular note, Acinetobacter baumannii was recovered from the floor of one patient room with a previous diagnosis of sepsis by MDR Acinetobacter baumannii. This isolate was tested for antibacterial susceptibility and it displayed a similar phenotype to both clinical isolates.
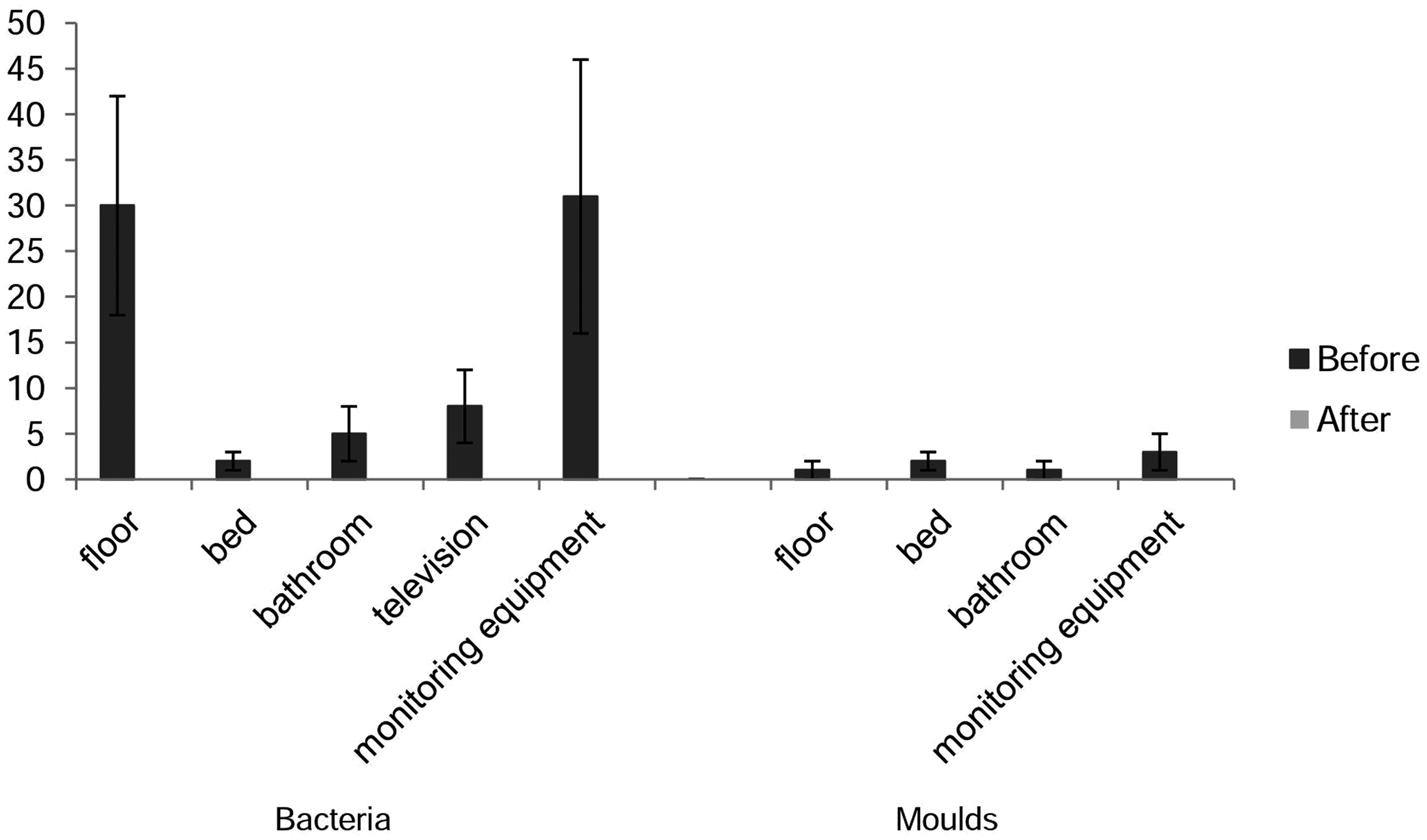
Results of contact plate cultures from surfaces of the five patient rooms, represented as the total number of colony forming units per square centimeter (CFUs/cm2), before and after the disinfection procedure with Glosair™ 400 system (Advanced Sterilization Products, Irvine, CA). Samples were obtained by pressing brain heart infusion agar medium contact plates against the different surfaces. Sampling was performed in duplicate.
After the intervention
Regarding surface samples obtained with contact plates after the use of the dry-mist system, no microbial growth was observed (Fig. 1). In the specific case of Acinetobacter baumannii, no further phenotypically related isolates were recovered from patients.
Discussion
Routine manual techniques for terminal decontamination of surfaces do not eliminate microbial pathogens completely. Therefore, improved no-touch methods addressing surface decontamination may be needed in order to reduce environmental sources of micro-organisms, particularly when dealing with an MDR microbial outbreak. As suggested by previous studies, hydrogen peroxide disinfection systems are a promising technology for environmental decontamination in hospital settings [8]. We used a system that provides aerosolized hydrogen peroxide/silver cations dry-mist. This technology was described previously to be effective against Clostridium difficile spores [11], Mycobacterium tuberculosis [12], and against MDR micro-organisms such as methicillin-resistant Staphylococcus aureus and Acinetobacter baumannii [13]. Moreover, hydrogen peroxide is catalytically converted to water and oxygen at the end of the cycle—harmless to humans—thus reducing occupational risk.
The antimicrobial effectiveness of this dry-mist system was assessed in a clinical setting. Our results showed that a single disinfection cycle was enough to eliminate surface bacteria and molds. Contamination of equipment that is difficult to clean such as ventilators, monitors, and electronic cables is particularly problematic when new patients are admitted to rooms occupied previously by colonized or infected patients. Moreover, recent studies using hydrogen peroxide vapor technology did not report any damage to or malfunction of the exposed medical equipment [3]. The reduction of surface microbial contamination, with no micro-organisms recovered after a single cycle of the dry-mist system, should reduce the risk for patient transmission. In the case of Acinetobacter baumannii, although the reduction of one positive environmental culture to no positive samples after the intervention may seem minor, the fact that no further phenotypically related isolates were recovered from patients was of utmost importance from a clinical perspective.
Conclusions
This study supports the use of the hydrogen peroxide/silver cations dry-mist system as an adjunct to manual standard decontamination protocols of the healthcare environment because of its broad-spectrum activity against bacterial and fungal pathogens. A high antimicrobial effectiveness was demonstrated in disinfecting the surfaces of the burn unit isolation rooms, making this system a valuable option to consider especially in the control of microbial outbreaks.
Footnotes
Author Disclosure Statement
Ana Pinto Silva was supported by Foundation for Science and Technology (SFRH/BPD/102831/2014). For the remaining authors, no competing financial interests exist.