
Abstract
Abstract
Background:
Current practice guidelines for antimicrobial prophylaxis in surgery recommend a cephamycin or cefazolin plus metronidazole for various abdominal surgeries. In February 2016, cephamycin drug shortages resulted in a change in The Johns Hopkins Hospital's (JHH) recommendation for peri-operative antibiotic prophylaxis in abdominal surgeries from cefotetan to cefazolin plus metronidazole. The primary objective of this study was to quantify the percentage of abdominal surgeries adherent to JHH peri-operative antibiotic prophylaxis guidelines. A sub-group analysis investigated whether prophylaxis with cefazolin plus metronidazole was associated with a lower rate of surgical site infections (SSIs) versus cefotetan.
Patients and Methods:
This retrospective cohort study included adult inpatients who underwent an abdominal surgery at JHH in September 2015 (Study Period I: cefotetan) or February to March 2016 (Study Period II: cefazolin plus metronidazole).
Results:
Two hundred abdominal surgery cases were included in the primary analysis. A subset of 156 surgical cases were included in the sub-group analysis. The overall adherence rate to JHH guidelines was 75% in Study Period I versus 17% in Study Period II (p < 0.001). The largest difference in adherence was attributed to pre-operative administration time (87% vs. 23%, p < 0.001), primarily because of the longer infusion time required for metronidazole. Surgical site infections occurred in 14% (12/83) of surgeries with cefotetan versus 8.2% (6/73) with cefazolin plus metronidazole for prophylaxis (p = 0.19).
Conclusions:
Adherence to an institution-specific peri-operative antibiotic prophylaxis guideline for abdominal surgeries was limited primarily by the longer infusion time required for pre-operative metronidazole. A higher percentage of SSIs occurred among abdominal surgeries with cefotetan versus cefazolin plus metronidazole for prophylaxis.
A
Since the publication of the guidelines, several retrospective studies have demonstrated lower odds for SSI in colorectal surgery when administering cefazolin plus metronidazole as peri-operative antibiotic prophylaxis compared with other prophylactic regimens, including cefotetan or ampicillin-sulbactam alone [4–7]. Furthermore, a recent retrospective study conducted by the Michigan Surgical Quality Collaborative (MSQC) evaluated more than 18,000 surgical cases of abdominal and vaginal hysterectomy. The risk of SSI was found to be significantly higher for patients receiving a second-generation cephalosporin (e.g., cefoxitin, cefotetan, or cefuroxime; odds ratio [OR] 2.31; 95% confidence interval [CI] 1.21–4.41) compared with cefazolin plus metronidazole for prophylaxis [8]. It remains unknown whether the association between lower SSI rates and peri-operative antibiotic prophylaxis with cefazolin plus metronidazole can be extrapolated from colorectal surgery and hysterectomy to other abdominal surgeries.
On February 1, 2016, the Antimicrobial Stewardship Program at The Johns Hopkins Hospital (JHH) implemented a change from cefotetan alone to cefazolin plus metronidazole as the institution-specific peri-operative antibiotic prophylaxis guideline recommendation for various abdominal surgeries. This was driven by recent evidence suggesting lower rates of SSI associated with this regimen, as well as drug shortage issues. However, because the recommendation was to infuse metronidazole over 30–60 minutes, there were concerns for adherence to pre-operative antibiotic time of administration prior to incision.
The primary objective of this study was to quantify the percentage of abdominal surgery cases adherent to JHH peri-operative antibiotic prophylaxis guidelines (referred to herein as JHH guidelines). Secondary objectives were: (1) to determine the percentage of SSIs and re-admissions due to SSI within 30 days in abdominal surgery cases with cefotetan versus cefazolin plus metronidazole as peri-operative antibiotic prophylaxis and (2) to quantify the percentage of abdominal surgery cases with post-operative antibiotic prophylaxis for longer than 24 hours.
Patients and Methods
Patient selection
This retrospective cohort study included adult inpatients (≥18 years of age) who underwent an abdominal surgery at JHH between September 1, 2015 and October 1, 2015 (Study Period I: cefotetan) or February 15, 2016 and March 11, 2016 (Study Period II: cefazolin plus metronidazole). Patients were identified from operative records based on abdominal surgery performed. Colorectal, small bowel, bile duct/liver/pancreatic, gastric, and gallbladder surgery, as well as exploratory laparotomy requiring anaerobic coverage, were included. Patients were excluded if actively being treated for an infection with systemic antibiotic agents at the time of the surgery, if the purpose of the surgery was to treat an active infection, if the surgery was performed at the same site as a surgery that occurred within 30 days prior, or if death occurred within five days post-operatively. Antibiotic use, SSI development, and other patient data were collected from the electronic medical record.
The study was approved by JHH Institutional Review Board. Patients were screened for inclusion in chronological order, beginning on day one of each study period, until 100 abdominal surgery cases for each study period were included (Fig. 1). All surgical cases were assessed for adherence to JHH guidelines and cessation of antibiotic prophylaxis within 24 hours post-operatively, whereas only surgical cases with either cefotetan or cefazolin plus metronidazole as peri-operative antibiotic prophylaxis were included in the assessment for SSI and re-admission. The JHH guidelines provide recommendations for antibiotic selection, dosing, and timing (Table 1), as well as alternative, non-β-lactam antibiotics for patients with a documented penicillin allergy, based on type of abdominal surgery. The 2013 Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery recommend that administration of pre-operative antibiotic prophylaxis begin within one hour prior to surgical incision [3]. The Johns Hopkins Hospital has developed specific antibiotic recommendations for the minimum percentage of dose administered within one hour prior to incision based on several pharmacokinetic/pharmacodynamic studies to ensure that goals of efficacy are met (Table 1) [9–13]. Because the duration of infusion for antibiotics was not documented within the anesthesia medical record, all peri-operative metronidazole infusions were assumed to be infused over 30 minutes.
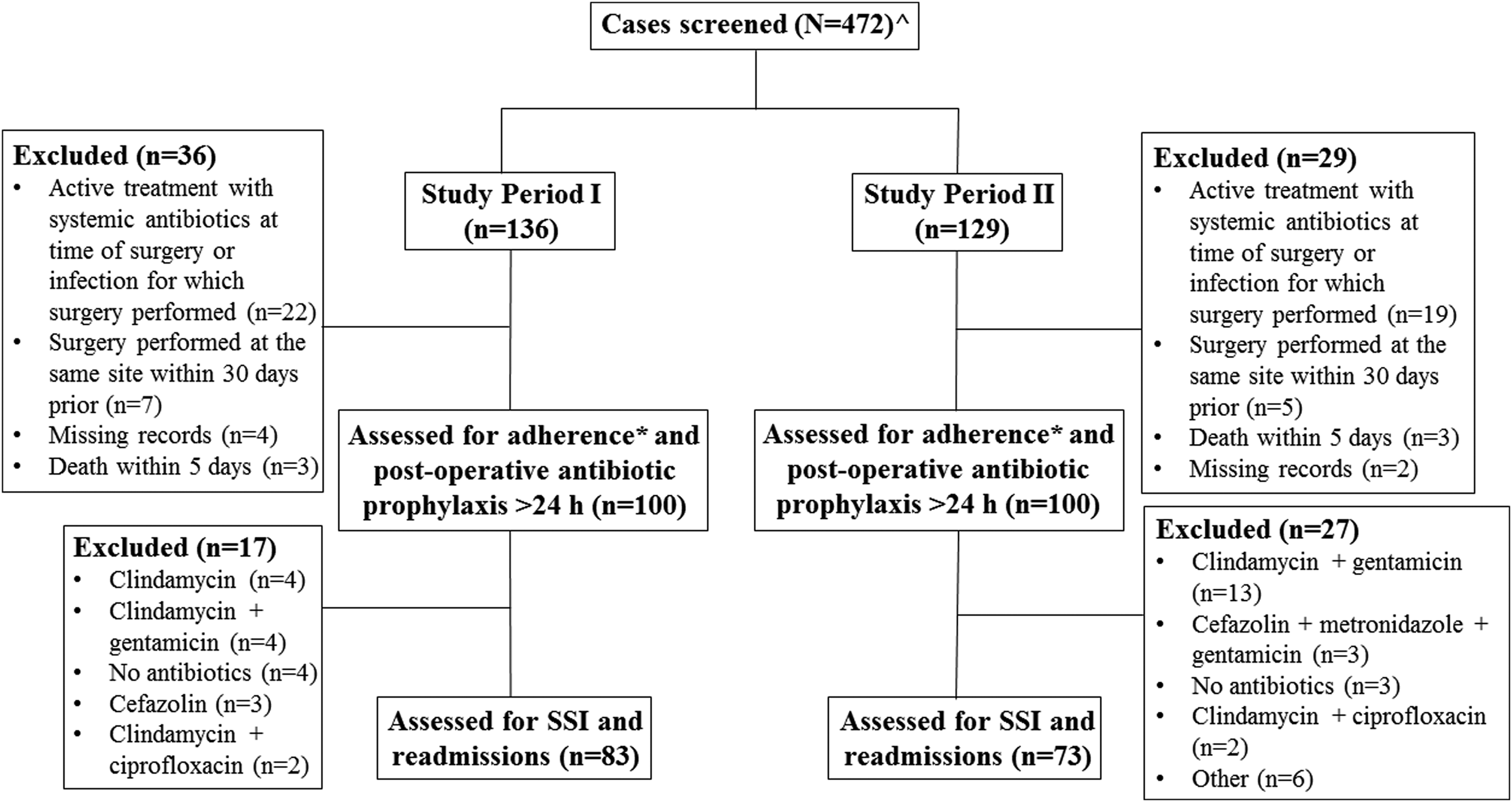
Patient selection flow diagram. ^Ninety and 117 cases in Study Period I and Study Period II, respectively, did not meet inclusion criteria based on type of abdominal surgery. *Adherence to The Johns Hopkins Hospital peri-operative antibiotic prophylaxis guidelines. SSI = surgical site infection.
Re-dose for every 1,500 mL of blood loss if CrCl >60 mL/min.
If on dialysis or CrCl <20 mL/min, use 2 mg/kg; use adjusted body weight if patient is ≥20% over ideal body weight.
For surgical procedures occurring during Study Period I, 100% of all antibiotics was required to be administered within 1 h prior to incision.
CrCl = creatinine clearance; IV = intravenous.
Definitions
Surgical site infections were identified and classified as superficial incisional, deep incisional, or organ/space based on the National Healthcare Safety Network (NHSN) surveillance definitions [2]. At least two study team members reviewed each potential SSI case. Adherence to peri-operative antibiotic choice, dose, and timing of administration was determined based on JHH guidelines (Table 1). Patients were considered to be immunosuppressed if they had any condition or medication known to impair the immune system, including a diagnosis of human immunodeficiency virus (HIV) with CD4 count <200 cells/mm3, receipt of bone marrow or solid organ transplant, absolute neutrophil count (ANC) <1,000 cells/mm3, corticosteroid treatment (≥ 20 mg/d prednisone or equivalent for two weeks or longer in the preceding three months), chemotherapy treatment in the preceding six months, or treatment at the time of surgery with one or more of the following agents: calcineurin inhibitor, mTOR kinase inhibitor, interferon, monoclonal antibody, tyrosine kinase inhibitor, mycophenolate, azathioprine, hydroxychloroquine, sulfasalazine, or leflunomide. Post-operative hyperglycemia was defined as a blood glucose of ≥180 mg/dL within 48 hours post-procedure.
The length of procedure was defined as the time from initial incision to surgery stop time, as noted in the anesthesia medical record. A surgical case was defined as one visit to the operating room, involving one or more procedures. For surgical cases including more than one procedure, the primary procedure represents the highest risk for SSI, as determined based on rankings provided by the NHSN Principal Abdominal Operative Procedure Selection List [2]. Post-operative antibiotic agents were defined as antibiotic agents administered immediately post-operatively without a documented indication for treatment of active infection.
Statistical analysis
The unit of analysis was the surgical case. Univariable comparisons were conducted using the Student t-test or Wilcoxon rank-sum test for continuous parameters, and the χ2 or Fisher exact test for categorical parameters. A two-tailed p value of 0.05 was considered significant. Logistic regression was performed, with development of SSI as the dependent parameter. Parameters with a p value of <0.05 in univariate analysis were evaluated for inclusion in the multivariate logistic regression analysis. All analyses were conducted using StataIC version 13.1 (StataCorp LLC, College Station, TX).
Results
Population
Two hundred abdominal surgery cases were assessed for adherence to JHH guidelines and post-operative antibiotic prophylaxis for longer than 24 hours, whereas a subpopulation of 156 surgical cases was assessed for SSI and re-admission. Baseline characteristics for all patients are shown in Table 2, with no significant differences between Study Periods I and II. The median age was 61 years, 50% (100/200) were male, 73% (145/200) were Caucasian, and the median weight was 77 kg. Notably, no patients required renal replacement therapy. Overall, 17% (33/200) had a documented penicillin allergy and 2% (4/200) had a documented cephalosporin allergy.
Unknown serum creatinine for one case in Study Period I.
BMI = body mass index; CrCl = creatinine clearance; EBL = estimated blood loss; SD = standard deviation; IQR = interquartile range.
Additional baseline characteristics were collected for the subpopulation of 156 patients who received cefotetan or cefazolin plus metronidazole for prophylaxis (Table 3). Similarly, there were no significant differences in baseline characteristics noted between groups. Overall, 15% (24/156) were diabetic, 26% (40/156) had a body mass index (BMI) >30 kg/m2, and the median length of procedure was 4.3 hours in the cefotetan group versus 4.7 hours in the cefazolin plus metronidazole group (p = 0.43). The median length of stay was 8 days in the cefotetan group versus 7 days in the cefazolin plus metronidazole group (p = 0.97). In the cefotetan group, 36% (30/83) were immunosuppressed, compared with 37% (27/73) in the cefazolin plus metronidazole group (p = 0.91). Post-operative hyperglycemia was common in both the cefotetan and cefazolin plus metronidazole groups (28% vs. 32%, respectively; p = 0.63).
Unknown first post-operative temperature for two cases in each group.
Unknown blood glucosemax for two cases in cefotetan group and one case in cefazolin plus metronidazole group.
For surgical cases including >1 procedure, the primary procedure was determined based on rankings by the NHSN [2].
Surgical case included in study if ≥1 procedure met inclusion criteria.
BMI = body mass index; IQR = interquartile range; NHSN = National Healthcare Safety Network.
The distribution of abdominal surgeries within the subpopulation is also shown in Table 3. The most common procedures were bile duct/liver/pancreatic (44%) and colorectal (39%). Fifty-seven percent (89/156) and 22% (34/156) of surgical cases involved greater than one surgery and greater than two surgeries, respectively. There were no differences in the distribution of abdominal procedures between the cefotetan versus cefazolin plus metronidazole groups.
Adherence to guidelines
Cefotetan accounted for 83% (83/100) of pre-operative antibiotic prophylaxis in Study Period I versus 0% (0/200) in Study Period II, whereas cefazolin plus metronidazole accounted for 75% (75/100) in that of Study Period II versus 0% (0/200) in Study Period I. Sixty-four percent (127/200) were not re-dosed with prophylactic antibiotic agents intra-operatively.
Adherence to JHH guidelines is shown in Table 4. Adherence to both pre-operative and intra-operative guidelines was found to be greater in Study Period I versus Study Period II (75% vs. 17%, p < 0.001). Pre-operative adherence alone was also greater in Study Period I (80% vs. 19%, p < 0.001), as was intra-operative adherence alone (93% vs. 83%, p = 0.03). The difference in adherence to pre-operative antibiotic administration time accounted for the most significant difference in adherence between Study Period I versus Study Period II (87% vs. 23%, p < 0.001). Pre-operative and intra-operative adherence to choice and dose of antibiotic agent remained high in both study periods (i.e., ≥89%). Evaluating only those patients who received cefotetan or cefazolin plus metronidazole, adherence to pre-operative antibiotic administration time was found to be 98% with cefotetan versus 25% with cefazolin plus metronidazole (p < 0.001), with 99% of cefazolin doses adherent to administration time. Specific reasons for non-adherence to both pre-operative and intra-operative guidelines are also shown in Table 4.
Unknown administration time for one case in Study Period II.
EBL = estimated blood loss.
Surgical site infection and re-admission
Among patients who received peri-operative antibiotic prophylaxis with cefotetan, 14% (12/83) developed a SSI, compared with 8.2% (6/73) of those who received cefazolin plus metronidazole (p = 0.19; Table 5). The majority (72%) of SSIs were classified as organ/space. The number of organ/space infections was similar between the two groups; however, 6% (5/83) of patients in the cefotetan group developed superficial incisional infections versus 0% (0/73) in the cefazolin plus metronidazole group (p = 0.06). Surgical site infections occurred on median post-operative day eight in the cefotetan group versus day 12 in the cefazolin plus metronidazole group (p = 0.60). Overall, 5% (8/156) of patients were re-admitted within 30 days because of SSI. Cultured pathogens were identified in 49% (11/23) of SSIs as represented in Table 6, with the majority of SSIs being polymicrobial (9/11).
SSI = surgical site infection; IQR = interquartile range; SD = standard deviation.
MRSA = methicillin-resistant Staphylococcus aureus; MSSA = methicillin-susceptible Staphylococcus aureus.
A multivariable logistic regression was performed, with the development of SSI as the dependent parameter (Table 7). Compared with peri-operative cefazolin plus metronidazole, peri-operative cefotetan was associated with a non-significant increase in odds for SSI (OR 4.98; 95% CI 0.46–54; p = 0.19).
BG = blood glucose; OR = odds ratio; CI = confidence interval.
Similarly, non-adherence to pre-operative administration time was associated with a non-significant increase in odds for SSI (OR 1.62; 95% CI 0.03–4.3; p = 0.44). Post-operative hyperglycemia was associated with a significant increase in odds for SSI (OR 2.80; 95% CI 0.98–7.9; p = 0.05).
Post-Operative Antibiotic Prophylaxis
Antibiotic prophylaxis was continued post-operatively in approximately 45% (89/200) of patients overall and 7% (14/200) received post-operative antibiotic prophylaxis for longer than 24 hours.
Discussion
In this retrospective study, adherence to an institution-specific peri-operative antibiotic prophylaxis guideline decreased by 58% after a change in recommendation from cefotetan to cefazolin plus metronidazole for abdominal surgeries. Whereas the administration of two agents is certainly more complex than a single agent, non-adherence was primarily because of the longer infusion requirement (30–60 min) of metronidazole, which frequently led to the completion of infusion after the time of incision.
In a retrospective study at a large French university hospital conducted over a four-month period, 44.4% of approximately 1,300 peri-operative antibiotic prophylaxis interventions assessed were not adherent with the 2010 French Society of Anaesthesia and Intensive Care recommendations [14]. Similar to the current study, the most frequent inappropriate practice was the timing of antibiotic administration (34.8% non-adherence), with the majority occurring later than recommended. In a retrospective analysis conducted at two Australian hospitals over a 12-month period, 400 patients undergoing abdominal surgery were randomly reviewed for adherence to the Australian guideline, Therapeutic Guidelines: Antibiotic (version 14), with respect to peri-operative drug choice, dosing, timing of administration, and duration of administration [15,16]. The overall rate of adherence was 16.5% at a metropolitan hospital versus 19.5% at a regional hospital. These results are similar to the combined pre- and intra-operative adherence rates observed in our study during Study Period II. In contrast to the current study's findings, however, drug choice was the most frequent error type (71.3% vs. 69.6%) in the Australian study, followed by timing of administration (50.3% vs. 50%), with the majority of non-adherence because of early administration.
Using the same Australian guidelines, another retrospective study including approximately 1,000 patients undergoing hip or knee arthroplasty at three metropolitan hospitals in Melbourne over a 2.5-year period found an overall adherence rate of 61.3% [17]. The overall SSI rate was 2.7%, with a lower rate in those adherent to antibiotic guidelines than in those non-adherent (1.7% vs. 5.0%, p < 0.01). Interestingly, timing of pre-operative antibiotic administration was excellent, with an adherence rate of 98.6%. Lower adherence rates were observed for duration of prophylaxis, timing of re-dosing, and dose adjustment in patients weighing more than 80 kg.
Consistent with previous studies, a higher rate of SSIs was observed in the cefotetan group versus the cefazolin plus metronidazole group in the current analysis, although this fell short of reaching statistical significance [4–8]. In a nationwide, retrospective study including more than 400 hospitals and 90,000 patients who underwent open colectomies, overall SSI prevalence was found to be 5.2% [4]. The majority of patients (41.8%) received cefoxitin as peri-operative antibiotic prophylaxis. Compared with cefoxitin, lower odds for SSI were observed with ampicillin-sulbactam (OR 0.71; 95% CI 0.63–0.82), ertapenem (OR 0.65; 95% CI 0.58–0.71), and metronidazole plus cefazolin (OR 0.56; 95% CI 0.49–0.64). Metronidazole plus cefazolin resulted in the lowest overall SSI prevalence at 3.5%; cefotetan resulted in the highest at 5.9% of patients. In another retrospective study including more than 4,000 colectomy patients conducted by MSQC, ciprofloxacin plus metronidazole, cefazolin plus metronidazole, and ertapenem (p < 0.001, p < 0.001, p = 0.03, respectively) were each associated independently with lower SSI rates [6]. This association was not observed with ampicillin-sulbactam, cefoxitin, or cefotetan.
Common causative organisms of SSIs resulting from abdominal surgeries include Bacteroides fragilis and other obligate anaerobes, aerobic Gram-negative enteric organisms (particularly Escherichia coli), Enterococcus spp., and skin flora, including Staphylococcus aureus and coagulase-negative staphylococci [3]. An important factor that may contribute to the difference in the effectiveness of antibiotic prophylaxis are increasing resistance rates of Bacteroides fragilis to the cephamycins [18–20]. In a European survey from 2007, 48% of Bacteroides fragilis isolates were found to be resistant to cefotetan [21]. Furthermore, induction of resistance among Gram-positives has also been described, with a decrease in activity of cefotetan against Staphylococcus aureus and streptococci [22–25].
According to the Food and Drug Administration (FDA)-approved package insert, intravenous metronidazole (prepared as 500 mg/100 mL) is recommended to be infused over 30–60 minutes for surgical prophylaxis [26]. An infusion rate of metronidazole 25 mg/min has also been recommended, which would equate to a 20-minute infusion for a 500 mg dose [27]. A recent randomized, controlled trial in Switzerland reported administration of pre-operative metronidazole 500 mg over two to five minutes for peri-operative prophylaxis [28]. Although it remains unknown whether this is safe and effective, this administration strategy would likely improve adherence to administration time of metronidazole prior to incision.
Adherence to pre-operative administration time was shown to have a non-significant decrease in odds for SSI. Because this study was not adequately powered to detect a difference in SSI between cefotetan versus cefazolin plus metronidazole, it is unclear whether this relation would persist as insignificant if the study was in fact powered to detect such a difference. Post-operative hyperglycemia was shown to be associated with an increase in odds for SSI, which is consistent with previous studies [29–32]. This highlights the continued importance of post-operative glucose monitoring and control in prevention of SSI.
The current study found that 7% of the 200 surgical cases included received post-operative prophylaxis for longer than 24 hours. The 2013 Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery recommend that if antimicrobial prophylaxis is continued post-operatively, the duration should be less than 24 hours, regardless of the presence of intravascular catheters or indwelling drains [3]. The Executive Summary of the College of Surgeons/Surgical Infection Society Surgical Site Infection Guidelines recently published an update that recommends that antibiotics be discontinued at the time of incision closure, with certain exceptions [33,34]. Despite the lack of evidence in the effective use of post-operative antibiotic prophylaxis in the prevention of SSI, this practice was shown to still be common at this institution, although prolonged use beyond 24 hours was low.
There were several limitations to this study. The retrospective, single-center study design using institution-specific guidelines limits its external validity. Some data were not available in the electronic medical record for evaluation. It is possible that patients received medical care for a SSI at an institution other than JHH. As previously mentioned, the study was not powered to detect a significant difference in SSIs between peri-operative cefotetan versus cefazolin plus metronidazole. Furthermore, the total number of events of interest (i.e., SSI) was low, which limited the number of independent parameters that could be included in the multivariable logistic regression. The number of parameters was limited to three to preserve the reliability of the model [35].
Because the duration of infusion for antibiotic agents was not documented within the anesthesia medical record, all peri-operative metronidazole infusions were assumed to be infused over 30 minutes, which may have overestimated adherence. Although timing of pre-operative antibiotic prophylaxis assessed as a continuous parameter may have been interesting to evaluate, particularly given that existing evidence for optimal timing is not completely clear, we were unable to do so given the constraints of retrospective data collection (specifically, lack of consistent documentation of duration of infusion) [36].
Oral antibiotic bowel preparation was not accounted for in the evaluation of SSI, although this is standard practice at this institution for colorectal surgery. Finally, sensitivities of the antibiotic agents of interest against recovered organisms from SSIs were not reported because of small numbers and limited microbiology testing results for anaerobes, leading to lack of clinically meaningful evaluation.
In conclusion, adherence to an institution-specific peri-operative antibiotic prophylaxis guideline for abdominal surgeries was limited primarily by the longer infusion time required of pre-operative metronidazole prior to incision, perhaps in addition to the added complexity of administering two antibiotics pre-operatively. There was no statistically significant difference in SSIs, although the study was not powered to detect a difference. Studies validating the safety and efficacy of rapid administration of metronidazole over two to five minutes are needed, as this has the potential to improve guideline adherence and, potentially, patient outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.