
Abstract
Abstract
Background:
We aim to update a meta-analysis to evaluate the efficiency of polymerase chain reaction (PCR) for diagnosis of periprosthetic joint infection (PJI) because different types of PCR assays have yielded variable diagnostic efficiency from 2013.
Methods:
We conducted our systematic review by searching for keywords in online databases from 2013 to May 2017. Studies were chosen based on inclusion and exclusion criteria and the quality of included studies was assessed. Pooled sensitivity and specificity were compared with other synovial fluid biomarkers. A total of 20 studies, comprising 2,526 participants were assessed.
Results:
The pooled sensitivity, specificity, and diagnostic odds ratio (DOR) were 0.76 (95% confidence interval [CI]: 0.65–0.85), 0.94 (95% CI: 0.92–0.95), and 0.94 (95% CI: 0.92–0.96), respectively. Meta-regression analysis indicated that use of specific genes, fresh samples, and more than one sample per patient may improve sensitivity.
Conclusions:
Although novel PCR assays have been developed, the sensitivity of PCR for the diagnosis of PJI had decreased compared with the previous meta-analysis (0.86, 95% CI: 0.77–0.92), whereas the high specificity is reliable for excluding PJI. Novel synovial fluid biomarker such as α-defensin, which possesses pooled sensitivity between 0.96 and 1.00, might be more efficient than PCR in PJI diagnosis.
T
The American Academy of Orthopedic Surgeon's (AAOS) guidelines first appeared in 2010 as a reference for the diagnosis of PJI [3], and includes erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) as screening tests and aspiration of the joint when serologic markers are elevated. In 2013 the Musculoskeletal Infection Society (MSIS) issued a consensus statement providing a concise definition of PJI [4]. Although the MSIS definition provides a standard for definitive retrospective diagnosis and research, it has a complexity that makes it difficult to execute in daily clinical practice [5].
Polymerase chain reaction-based method for the diagnosis of PJI began to be used in the past decade. With the high sensitivity and short required time, it has been considered as a reliable and accurate method for detection of PJI [6]. Along with the development of PCR, different PCR assays occurred in recent years, which facilitate clinical diagnosis. There continues to be more published articles regarding the diagnosis of PJI with PCR, however, the sensitivity varies greatly among these studies. In addition, more synovial fluid biomarkers for the diagnosis of PJI have been investigated during the past several years, most of which are also reported to be highly sensitive and specific [7–9].
Qu et al. [6] conducted a meta-analysis of PCR as a diagnostic tool for PJI. The pooled sensitivity was reported to be 0.86 (95% confidence interval [CI]: 0.77–0.92), whereas specificity was 0.91 (95% CI: 0.81–0.96). However, some recent articles have recommended culture instead of PCR because cultures of sonication periprosthetic tissue were more sensitive than PCR [10–12]. Some authors expressed concern regarding the susceptibility to contamination, labor-intensive DNA extraction, and limited use because of the pathogen panel [13,14]. One investigator reported that PCR did not yield additional information to that of microbiologic cultures [15]. In addition, in previous meta-analyses, there was no gold standard for PJR detection, which is a drawback to assess PCR procedures for diagnostic accuracy. Last, the prospective manner of studies was not clarified in the previous systematic analysis, which might influence the sensitivity.
Thus, we considered it essential to update the diagnostic accuracy of PCR to evaluate its efficiency in the diagnosis of PJI. We onducted a meta-analysis based on articles published from 2013 to May 2017. Our hypothesis was that the pooled sensitivity might be influenced from varied types of novel PCR methods. In addition, we also compared PCR assay with some recently developed synovial fluid biomarkers to provide a better diagnostic panel for PJI.
Methods
The methodological approach to evidence searching and synthesis described in this protocol was based on the Cochrane Collaboration's diagnostic test accuracy method. We adhered strictly to standards of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) in reporting the findings of this review.
We searched electronic databases including PubMed, Embase, Web of Science, the Cochrane Library, and Science Direct for entries recorded from 2013 to May 2017. The starting date was chosen as 2013 because previous meta-analyses ended by 2012. We used all the newly published articles from 2013 so that the results could represent directly the diagnostic efficiency of newly developed PCR methods. We used keywords or Mesh words as follows: “periprosthetic joint infection” or “prosthesis-related infections” and “PCR” or “polymerase chain reaction” as our target index.
Two researchers reviewed independently the title and abstract of each assay to select those that were likely for further screening. Inclusion criteria included: (1) patients who had undergone knee, hip, or shoulder joint replacements and were suspected of having PJI; (2) MSIS or AAOS criteria or a combination of clinical data including the clinical symptoms of pain, local swelling and heat, tenderness, aspiration of purulent joint fluid, purulence surrounding the disease site, and laboratory findings such as white blood cell (WBC) count, ESR, CRP. Cultures of synovial fluid or tissues obtained surgically from the infected site were considered as the gold standard for diagnosis of PJI; (3) PCR was performed with synovial fluid or periprosthetic tissues; (4) sufficient data was provided to construct the diagnostic 2 × 2 table. Exclusion criteria included: insufficient data to calculate for sensitivity and specificity; unqualified article format such as case reports, commentaries, expert opinion, narrative reviews, and duplicates.
The methodological quality of the included studies was appraised by an adapted version of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2), which consist of four key domains that address patient selection, index test, reference standard, and flow and timing. (Review Manager [RevMan] [computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.).
The following information was extracted: (1) study characteristics including author, year of publication, country, design, sample size, gold standard; (2) sample and detection characteristics including sample type, sample condition (fresh or frozen), number of samples collected for PCR, method of PCR, target genes; (3) outcomes including false/true positive, false/true negative from 2 × 2 table for diagnostic studies. Data were extracted by a single reviewer for all outcomes and then verified by the second reviewer.
The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood (NLR), and the diagnostic odds ratio (DOR) were calculated by using the bivariate model. The summarized receiver operating characteristic (SROC) curve was constructed. The percentage of the total variation across studies was described by the I2 statistic. We performed meta-regression and subgroup analyses to assess potential heterogeneity, and we constructed Deeks funnel plot asymmetry test to evaluate potential publication bias. All statistical analyses were conducted using both Meta-DiSc software (version 14.0, Madrid, Spain) and Stata software (version 14.0, StataCorp, College Station, TX). According to the previous meta-analysis and comments related to the meta-analysis, the pooled sensitivity and specificity generated from Meta-DiSc and Stata are different. Thus, we used both of these statistical methods and compared the results between them.
Results
Identification and characteristics of the study
Of the identified 194 articles, 20 articles were included for systematic review and meta-analysis [10–29] (Fig. 1). A total of 2,526 patients who had undergone joint arthroplastic surgery were included and the detailed information of study design and PCR methods are provided in Table 1. Twelve studies were conducted prospectively and samples were fresh, whereas the other eight were conducted retrospectively and samples were frozen. Six studies used MSIS whereas the remaining studies used reference standard of their own institute for diagnosis of PJI. As for target genes, 11 studies used specific genes of bacteria, six studies used 16s rRNA, whereas the remaining three studies used both types of genes. Seventeen studies detected infection of hip or knee, whereas three studies also included shoulder and elbow. Eleven studies used more than one type of sample such as synovial fluid, prosthesis tissues, or bone biopsies, whereas the other nine studies used only synovial fluid or prosthesis tissues.

Flow chart of selection process for eligible studies.
PCR = polymerase chain reaction; PJI = periprosthetic joint infection; P = prospective study; R = retrospective study; MSIS = Musculoskeletal Infection Society; IDSA = Infectious Disease Society of America.
Quality assessment of individual studies
Graphical summary of the methodological assessment based on QUADAS-2 quality assessment for the included 20 studies is shown in Figure 2. All the included studies fulfilled the requirements of acceptable reference standard, partial verification bias avoided, differential verification bias avoided, incorporation bias avoided, detailed description of index test, blinding of investigators to reference, uninterpretable results reported, and withdrawals explained.

Quality assessment of included studies using Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool criteria. Color image is available online at www.liebertpub.com/sur
Diagnostic value of PCR for diagnosis of PJI
The pooled sensitivity with Meta-DiSc is 0.69 (95% CI: 0.66–0.72), which is lower than that with Stata, 0.76 (95% CI: 0.65–0.85). The pooled specificity was the same with two methods, 0.94 (95% CI: 0.90–0.97) and 0.94 (95% CI: 0.92–0.95) for Stata and Meta-DiSc, respectively (Fig. 3A–3D). The DOR was 54 (95% CI: 28–106) and 42.23 (95% CI: 24.21–73.69), respectively, analyzed with Stata and Meta-DiSc. The area under the summarized receiver-operating curve (SROC) was 0.94 (95% CI: 0.92–0.96) and 0.93 (95% CI: 0.91–0.96), respectively, with Stata and Meta-DiSc (Fig. 4A and 4B). The meta-analysis of Meta-DiSc is based on a traditional univariate model, whereas Midas module for Stata (version 11) is based on a bivariate mixed-effects regression model. The post-test probabilities based on various pre-test probabilities were illustrated using a Fagan nomogram (Fig. 5).

Pooled sensitivity and specificity of polymerase chain reaction (PCR) in the diagnosis of periprosthetic joint infection (PJI). (
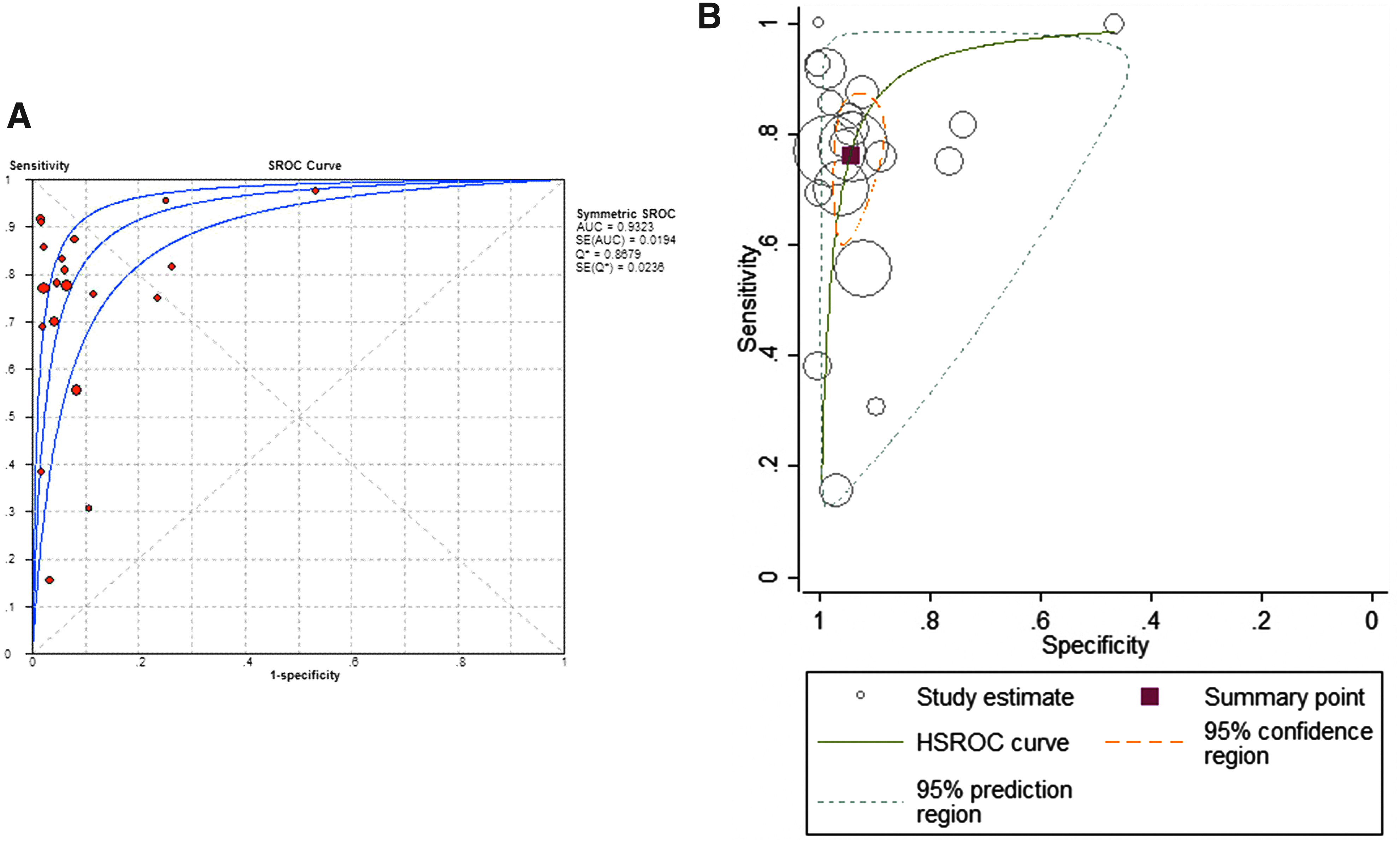
Summarized receiver operating characteristic (SROC) plot for the included studies with the associated 95% confidence region and the 95% prediction region. (
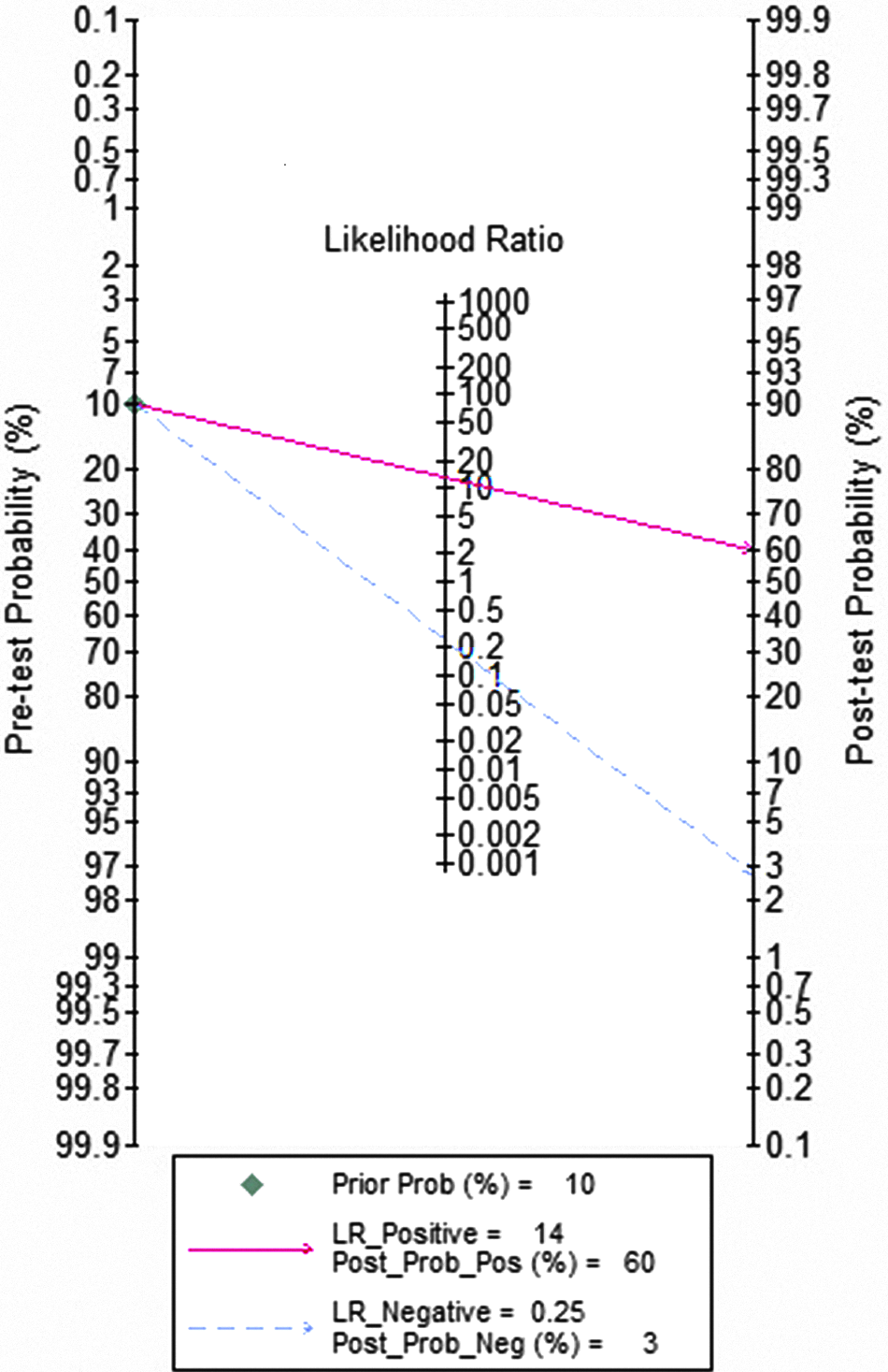
Fagan nomogram for the calculation of post-test probabilities with a fixed pre-probability of 60%. Color image is available online at www.liebertpub.com/sur
The between-study variability (heterogeneity) was high for sensitivity and specificity (with an I2 of 89.49 for sensitivity and 85.85 for specificity with Stata). We then performed subgroup analysis based on sample condition, sample size, target gene, reference standard, sonication, and sample type to explore the heterogeneity of the study further. Meta-regression indicated that target gene, sample condition, and sample number per patient accounted for the heterogeneity of specificity (Table 2). Finally, Deeks funnel plot indicated the absence of publication bias (p = 0.79; Fig. 6).
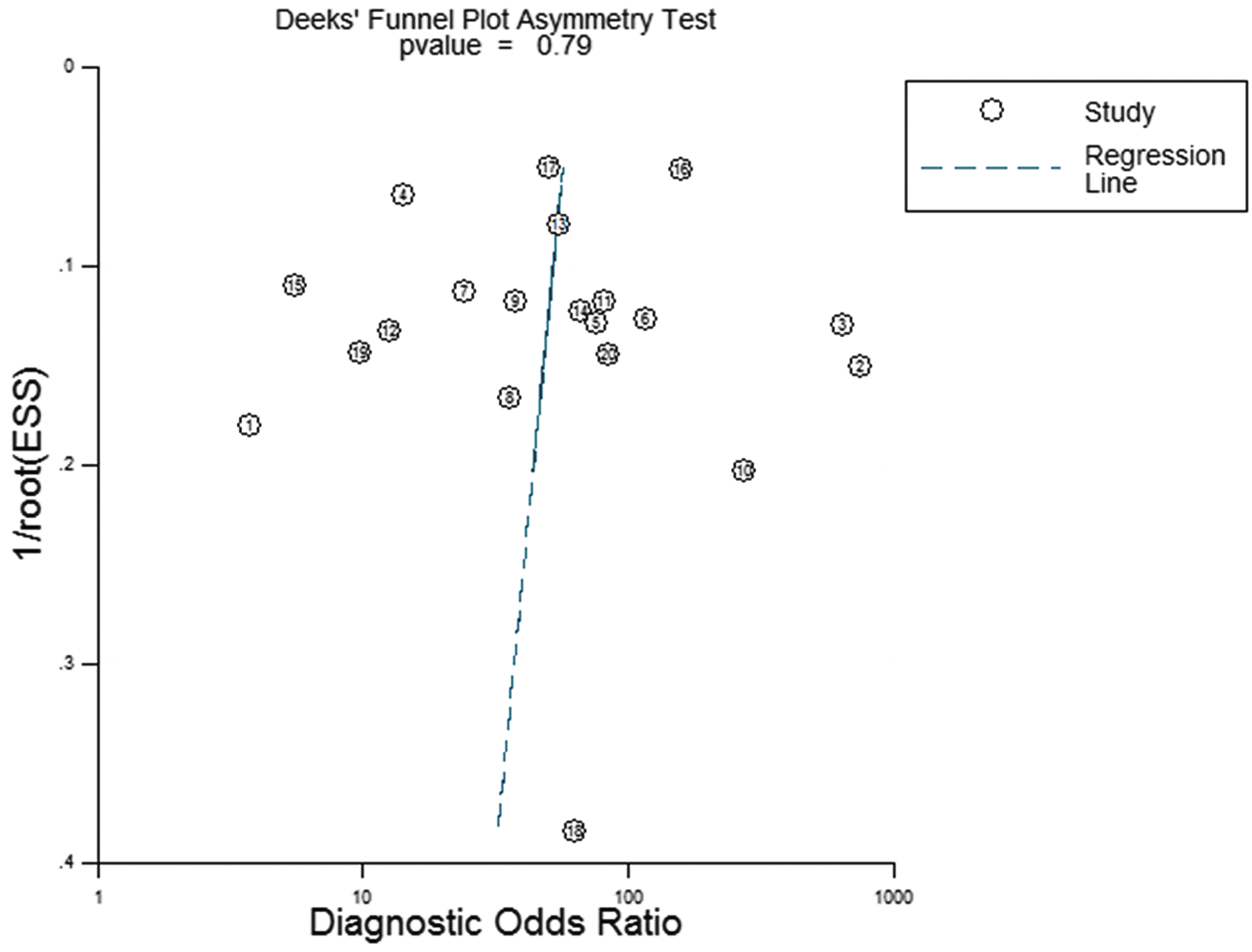
Deeks funnel plot for the evaluation of publication bias (p = 0.79). Color image is available online at www.liebertpub.com/sur
p < 0.05.
p < 0.01.
CI = confidence interval; MSIS = MSIS = Musculoskeletal Infection Society.
Discussion
The current updated meta-analysis indicated that although novel types of PCR assays have been developed to identify synovial fluid bacteria, sensitivity of PCR for diagnosis decreased whereas specificity increased compared with the previous study [6]. Because of its variable sensitivity, PCR should be combined with other biomarkers in the diagnosis of PJI.
Identification of bacteria from tissue or synovial fluid is still considered as the gold standard for diagnosis of PJI. Traditionally, periprosthetic tissue culture, which has a positive detection rate of 0.70–0.90, is regarded as the gold standard test for PJI diagnosis [30,31]. However, in clinical practice, some types of bacteria are difficult to culture, which consequently confounds the use of antibiotic agents and surgical decisions. Thus, in clinical laboratories various types of PCR have been developed to test the existence of bacteria, which theoretically generates higher sensitivity, a faster turnaround time, and is not affected by current treatment [17]. Polymerase chain reaction become a prevalent technique for identification of bacteria. The popularity of PCR for diagnosis of PJI over the past several years is illustrated by the additional 20 publications.
Among the 20 studies, commercialized or home-designed PCR assays are summarized as follows. Unyvero ITI cartridge multiplex PCR system [30] (U-ITI; Curetis AG, Germany) can be used for specific genes in the panel including Staphylococus aureus, coagulase-negative staphylococci, Streptococcus agalactia, Escherichia coli, Enterococcus faecalis, etc. Xpert MRSA/SA SSTI assay [14,27] (Cepheid, Sunnyvale, CA) is designed for detection of mecA (gene for methicillin resistance), SCCmec (gene for staphylococcus cassette chromosome) and spa (staphylococcal protein A). Prove-it Bone and Joint StripArray assay (research-use-only version; Mobidiag Ltd., Helsinki, Finland) is used as broad-range PCR and microarray-based assay targeting more than 60 bacterial species, such as topoisomerase genes gyrB (Staphylococcus aureus) and parE (Streptococcus pneumoniae), and the methicillin-resistance gene mecA. As for PCR-Electrospray Ionization Mass Spectrometry (PCR-ESI-MS; Abbott Laboratories, Abbott Park, IL) , the molecular mass of the amplified DNA was determined by mass spectrometry. The organism detected (assessed based on the PCR assay that was positive and the base composition of the amplified product inferred from its molecular mass) was determined by the system's software with two parameters additionally reported, Q-score and level of detection [20]. In addition, universal primers of 16s rRNA or home designed primers of specific genes for multiplex PCR were reported in the remaining studies. Thus, in recently published studies, researchers prefer to use specific genes because this can assist clinicians determining which antibiotic agents can be used for treatment. However, in previous meta-analysis, only 2 included studies used Propionibacterium or Staphylococcus probes, the other 12 studies used 16s rRNA as the target gene. After amplification with universal primers, they performed sequencing to further identify the species of bacteria. Multiple available PCR assays give more options for clinicians and covers more types of bacteria to enhance results.
Because of the comments and reply to the previous meta-analysis [32,33] that different statistical model might influence the pooled results, we used both methods: Stata and Meta-DiSc. In agreement with the previous statement, there is a slight difference between Stata and Meta-DiSc in pooled sensitivity (0.76 and 0.69, respectively). But both these results are lower than the sensitivity of a previous study (0.86). The specificity of both methods is 0.94, which is higher than that of a previous study (0.91).
We further analyzed the included articles and attempted determine why with more novel PCR methods, the sensitivity of the pooled results decrease. Subgroup analysis indicated that target gene, sample condition, and sample number per patient accounted for the heterogeneity of specificity. First, for genes that were used for PCR, 16s rRNA (universal gene) or methicillin resistance (mecA, specific gene for Staphylococcus aureus) were most common. Universal genes can theoretically be identified in almost all bacteria, but it is difficult to establish a threshold and thus may generate false positives. The combination of PCR and sequencing is required. Only when at least two of the three samples demonstrate the same pathogen-related sequence can the bacterial identification be considered accurate [13]. However, if PCR is limited to a fixed panel of pathogens, it means that some types of pathogens cannot be identified with this assay, such as Staphylococcus lugdunensis, thus generating false-negative results. Second, the PCR method does not discriminate between dead and living bacteria; samples that are culture-negative may have a positive molecular result, which may explain culture-negative but PCR-positive results. Third, although new methods have been developed, the sensitivity of broad primer PCR (BR-PCR) depends on the analytical sensitivity in each laboratory, which may also generate false negatives. Fourth, sample condition may affect the PCR result. Prolonged storage of the studied specimens, low organism burden in synovial fluid, low specimen volume analyzed, and inhomogeneous distribution of organisms in synovial fluid can lower the sensitivity [10]. Last, some studies used only one sample, but others used two or more, which makes the result difficult to explain and result in different sensitivity. However, sample type (sonication synovial fluid, bone, or periprosthetic tissue) did not influence the sensitivity, which contradicts our previous hypothesis because bacteria are reported to be present on the surface of the prosthesis in the form of a biofilm and not in the surrounding tissue.
Joint aspiration is performed conventionally in patients with suspected PJI. Recently, research on PJI diagnosis has focused on synovial fluid because it represents the local environment of infection. Studies revealed that various types of antimicrobial peptides and inflammatory cytokines including interleukin (IL)-1, IL-6, IL-17A, interferon (IFN)-γ, and tumor necrosis factor (TNF)-α could be used as biomarkers but were non-specific to PJI. Other newly developed markers such as CRP, α-defensin, cathelicidin LL-37, although more specific for PJI, require enzyme-linked immunosorbent assay (ELISA) or immunoassay as the detection methods. These newer markers require more time to complete. Meta-analysis regarding synovial fluid biomarkers most frequently used for diagnosis of PJI include α-defensin, CRP, procalcitonin (PCT), and IL-6 was summarized [7–9,34,35] (Table 3). Based on the above meta-analysis, pooled sensitivity of α-defensin ranging from 0.96 to 1.00 is higher than the other biomarkers (IL-6: 0.72, PCT; 0.53, leukocyte esterase: 0.81, CRP: 0.92) and also higher than PCR. In addition, the specificity of these synovial fluid biomarkers varies within a smaller range, 0.90 to 0.99, which is similar to the sensitivity of PCR.
CI = confidence interval.
This study has several limitations. First, the gold standard for the diagnosis of PJI is not limited to MSIS, which is the consensus. Some studies used their own criteria for diagnosis, thus the varied diagnostic standard might influence results. Second, similar to the previous meta-analysis, the pooled results of our study also had high statistical heterogeneity. Third, antibiotic treatment was unclear in some studies, which is considered to be critical because it may lead to false-negative results.
Conclusions
We provide an update to a meta-analysis of PCR for diagnosis of PJI from 2013 to May 2017. The pooled sensitivity is lower than the previous meta-analysis and the pooled specificity is higher. We believe that the variability of reported sensitivities/specificities is generated from the net result of differences in technology, techniques, type of infections, expertise, and the lack of standardized methods. Thus, we are still in need of a more standardized PCR method. We recommend that further comparisons be made between PCR and synovial fluid biomarkers to assess their relative clinical effectiveness and cost effectiveness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
All authors declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work. There is no professional or other personal interest of any nature or kind in any product, service, and/or company that could be construed as influencing the position presented in or the review of the manuscript. Informed consent was obtained from all individual participants included in the study.
All data generated or analyzed during this study are included in this article.