
Abstract

To the Editor:
A
Currently, exsanguination is achieved by a Martin bandage. There is controversy regarding its use in hand infections. The opponents are concerned about the spread of infection and suggest avoiding exsanguination [2]. The proponents do not believe that such a risk exists. Green, a senior hand surgeon, in his 25 years of practice, was routinely exsanguinating infected limbs without encountering any problems [3]. However, there is no evidence in the literature either to support or to refute the claim of infection spread.
In order to evaluate whether elastic exsanguination causes spread of fluid from one compartment to another, we designed a simple study in eight cadaver upper extremities. After taking control radiographs, we injected 15–30 mL of radio-opaque contrast medium (Cysto-Conray II; 17.2% w/v iothalamate meglumine; Mallinckrodt Inc., St. Louis, MO) in either the thenar or the midpalmar space. These spaces were selected because of their distinct, well-defined boundaries. Thenar-space injections were performed in four specimens by direct injection of contrast medium at a point between the 2nd and 3rd metacarpal bones, deep to the flexor tendons at the level of the distal palmar crease. Midpalmar space injections were performed in four specimens by direct injection at a point between the 3rd and 4th metacarpal bones, deep to the flexor tendons at the level of the distal palmar crease. After injection, another radiograph was obtained to confirm the containment of the contrast medium within the designated boundaries. Elastic exsanguination then was applied from the fingers to the elbow, and repeat radiographs were taken.
We observed spread of contrast material in two of the four cadaver limbs injected in the thenar space, whereas no spread was seen in those having midpalmar-space injections. Figure 1 demonstrates the spread of contrast proximally up to the carpal bones and distally to the flexor pollicis longus sheath.
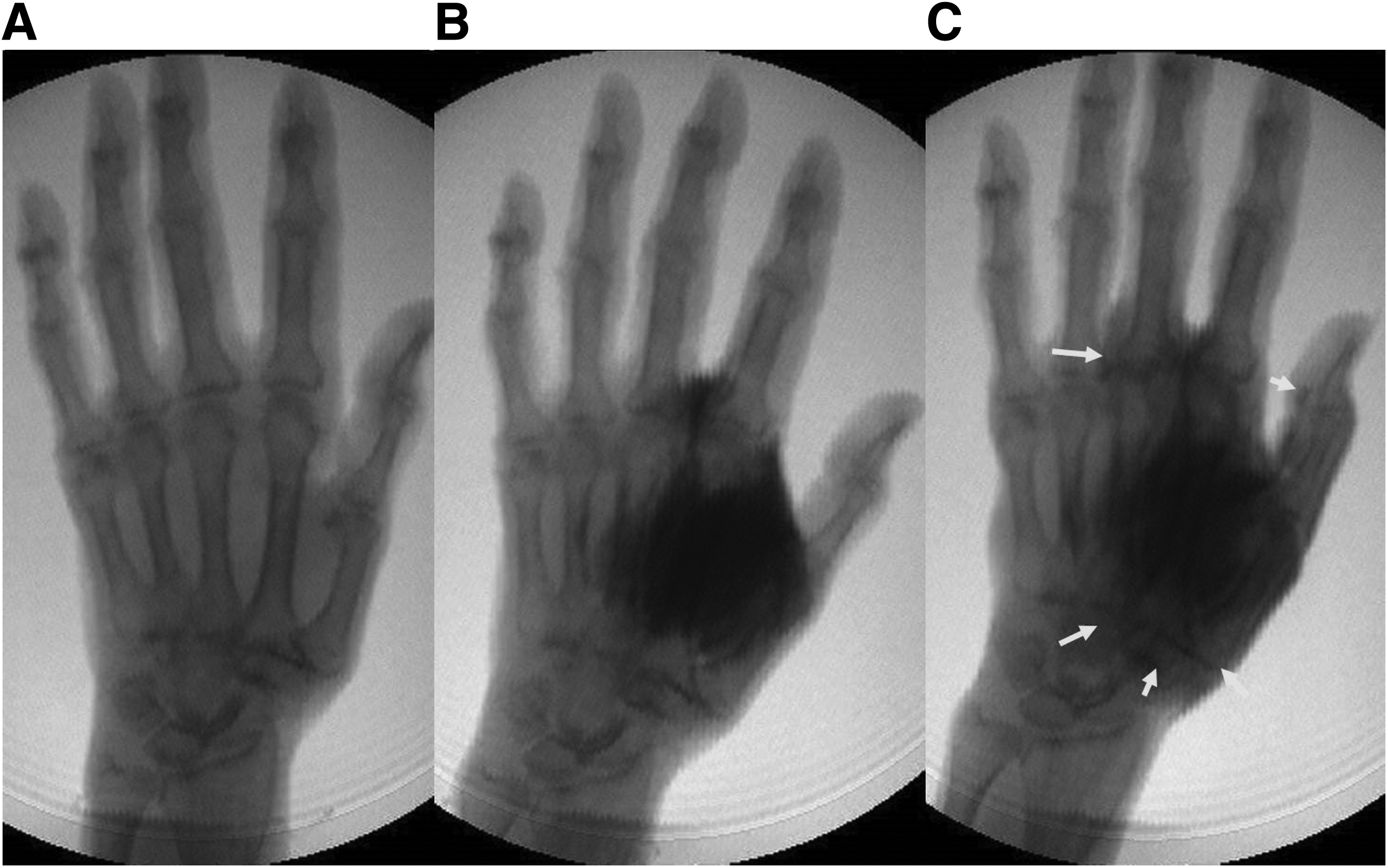
Example of spread of injection into thenar space. (
This is the first study to demonstrate spread of fluid from one compartment to another after application of elastic exsanguination. The reason for spread occurring in only two hands may be anatomic variations, difference in tourniquet pressure, or technical factors. Whether this spread would make any difference clinically after debridement and antibiotic treatment is not known. Whereas the use of elastic exsanguination may spread infectious material to adjacent tissues, it can be postulated that appropriate intravenous antibiotics can prevent any early infectious sequelae. However, with the increase in the number of immunocompromised patients and the prevalence of highly virulent multi-drug–resistant organisms rising steadily, it is foreseeable that additional tissue inoculation by infectious micro-organisms could have significant deleterious clinical effects. The principle of modern medicine is primum non nocere, and we strongly advise against use of elastic exsanguination in infected extremities. An alternative strategy of limb elevation and compression of the brachial artery can be used in such situations [4].
Footnotes
Acknowledgement
Presented at the Annual Meeting of the American Society for Surgery of the Hand (ASSH), San Francisco, California, September 7–9, 2017.