
Abstract
Abstract
Background:
Recent cases of hospital-acquired (HA) aspergillosis on our Trauma Service raised the question of whether this represented an outbreak or just increased case identification.
Patients and Methods:
After Institutional Review Board approval, we performed a retrospective analysis of all 117 patients with positive pulmonary Aspergillus cultures at Grand Strand Medical Center from 2010 through 2016. The diagnosis of community-acquired (CA) invasive pulmonary aspergillosis (IPA) was determined when patients were admitted with a pneumonia and the diagnosis was made within the first week of hospitalization.
Results:
Of patients with fungus cultures (3929), 3% (117) were positive for Aspergillus. More than 70% (84) of patients were colonized. The remaining 33 patients were treated for IPA. Twenty-seven patients had chronic respiratory problems and presented with a new lower respiratory illness; 23 had CA IPA diagnosed within the first week of admission with 17% mortality rate; four patients had a delayed diagnosis (probable CA) with a 75% mortality rate. The six remaining patients all underwent a surgical procedure and were suspected to have HA aspergillosis. There was a significantly higher rate of HA in the surgical subset in comparison with all nonsurgical patients (p < 0.03). Patients treated for IPA were more likely to be receiving high dose prednisone (>20 mg/day, p < 0.004) and their mortality rate was significantly higher than colonized patients (27.3% vs. 9.5%, p < 0.026). Patients with HA IPA were divided evenly over the years of the study period and not thought to represent an outbreak.
Conclusions:
Aspergillus infection is an endemic infection in this region of the southern Atlantic states and may occur in patients with major trauma as well as patients with chronic pulmonary diseases. Our data support the concept that there were no breaches in air quality to cause the IPA. Aggressive fungal therapy should be considered in all at-risk patients.
H
According to Kousha et al. [4], recent reports document an increasing number of cases of pulmonary aspergillosis in atypical patient populations with certain risk factors such as chronic obstructive pulmonary disease, but who were otherwise considered immunocompetent. After seeing several instances of HA Aspergillus within our trauma patients, we reviewed all hospitalized patients within a seven-year period and found a subset of patients with invasive pulmonary aspergillosis (IPA), not traditionally considered immunocompromised patients. This realization of increased Aspergillus infection rates in our seemingly atypical population prompted us to investigate further etiologic trends and clinical similarities.
Patients and Methods
After independent Institutional Review Board approval, we performed a retrospective analysis over seven years of all bronchopulmonary Aspergillus-related infections in patients who were evaluated at Grand Strand Medical Center from of 2010 through 2016. Initially, patients included in the study were identified with documented isolates on microscopic analysis of sputum or bronchoalveolar lavage samples.
Patients with quantitative pulmonary cultures (>105 colony forming units) positive for Aspergillus were separated into those with invasive and those with colonized based on data reported previously [5]. Patient with a positive culture who had signs compatible with infection and abnormal computed tomography or chest radiography were considered to have IPA. Patients who had a positive quantitative sputum culture but did not have symptoms and had negative radiographic studies were considered “colonized” and were not treated. All patients without pulmonary isolates were excluded in this review. The galactomannan assay was not used in the diagnosis of disease in these patients.
Patients were categorized further as having community-acquired (CA) or HA infections. Those with definite CA IPA had lung infection present on admission by abnormal chest radiography and had a lower respiratory tract culture within the first week of admission that grew Aspergillus. Those with probable CA IPA had lung infection present on admission, but did not have a lower respiratory tract culture for Aspergillus performed until hospital day eight to 14. Patients with HA IPA had negative chest radiography during the first week after admission followed by development of abnormal chest radiography seven days or later after admission.
Demographic data including date of onset of symptoms, zip code, medications, age, gender, date of bronchoscopy, presence of infiltrate on chest radiograph, date of treatment with antifungal agent, body mass index, medical comorbidities were collected (Table 1).
IPA = invasive pulmonary aspergillosis; Rx'd = treated; SD = standard deviation; ND = no difference; SC = South Carolina; ID = infectious disease.
Numerical data were expressed as mean ± standard deviation. Statistical analyses were performed on continuous data using one-way analysis of variance followed by Tukey multiple comparison post hoc test and Student t tests. Categorical proportions were compared using chi-square or Fisher exact test, as appropriate. The p values less than 0.05 were considered statistically significant. Statistical analyses were performed with QI Macros software for Excel (Know Ware International, Inc., Denver, CO).
Results
Demographics and Aspergillus characteristics
Microbiology data
Of the 11,164 sputum cultures performed at the institution over the 7-y period, 3929 (35%) were for fungus. Of these, 123 were positive for Aspergillus species, but six charts were unavailable, leaving 117 (3.0% of sputum cultures) patients available for analysis. Of the 117 patients, 33 were treated with antifungal agents for presumed IPA infections. The remaining 83 patients had positive sputum cultures but were not treated because of their clinical presentation. These patients served as our control group.
Community-acquired or HA
Thirty-three patients were treated for IPA; 23 (69.7%) had an abnormal chest radiograph and positive culture on admission and were categorized as definite CA IPA. Four additional patients had abnormal chest radiographs on admission but did not have lower respiratory fungal cultures performed until the second week of hospitalization (mean 11.0 ± 2.2 days, range 8–13 d) were positive for Aspergillus and were considered probable CA IPA. All of these patients had chronic lung disease.
The remaining six patients had negative chest radiographs during the first week of hospitalization and then pneumonias developed seven to 75 days after admission, mean 29.3 ± 25 days. All six of these patients came to the institution because of trauma or for a surgical procedure. Two patients had major trauma injuries, two had had a coronary artery bypass graft (CABG), and two were general surgery patients with complicated clinical courses (Table 2).
IPA = invasive pulmonary aspergillosis; Dx = diagnosis; ISS = Injury Severity Score; CT = cardiothoracic; MVR = mitral valve replacement; CABG = coronary artery bypass graft; Pt = patient.
Patient death.
Seasonal and annual variation
When the Aspergillus isolates were analyzed by the year of their occurrence, there were no significant trends identified. The mean number of cases per year was 4.7 ± 2.0, range 2–7 per year. Ground was broken for hospital construction for a new wing in 2010 and continued into 2011, during which time only four and two cases, respectively, were documented. When incidence by month was plotted, the mean number of cases per month was 2.8 + 1.2, range 0–5. The highest months were January (4), February (5), August (4), and November (4), which corresponded to planting and harvest seasons. The year and seasonal variation of diagnosis is graphically represented in Figure 1.
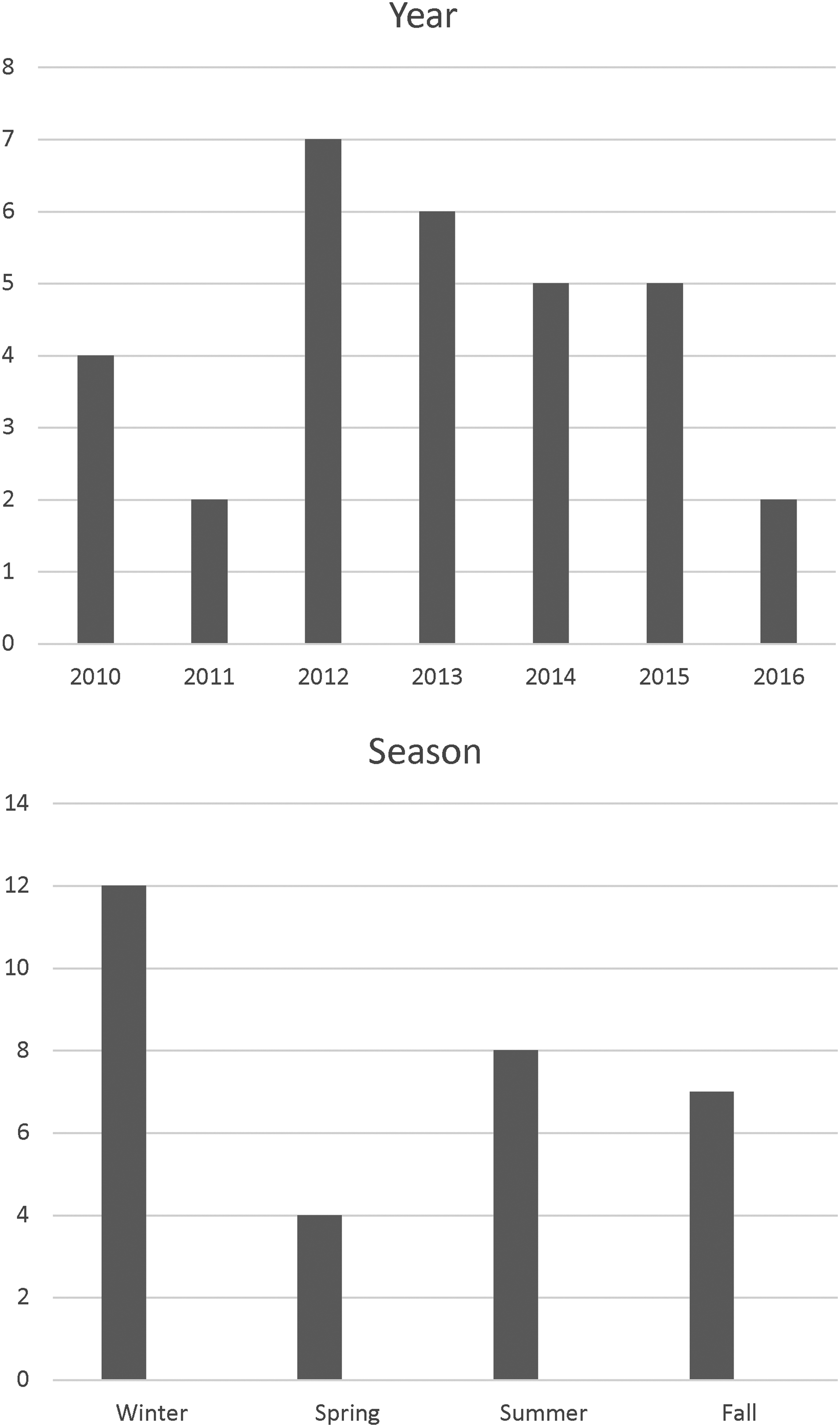
Variation of patients with invasive pulmonary aspergillosis by year and season. A peak in incidence was seen during the winter planting season.
Residence and Aspergillus infection
Because the town of Myrtle Beach is a popular vacation site with a large transient population, the zip code of the patients' home was recorded to identify whether or not they were local residents. Only four (12%) of the patients with IPA were not state residents. The majority of South Carolina residents were from Horry County.
Death
There were nine deaths overall for a mortality rate of 27.3%. Five deaths occurred in the definite CA group, three in the probably CA group, and in one of the HA patients, a CABG patient. There were no differences in mortality rates in the different IPA groups. The mortality rate in the IPA group, however, was greater in comparison with the Aspergillus colonized group (27.3% vs. 9.5%, p < 0.026).
Immunosuppression
The most frequent immunosuppressive agent used was prednisone. Eighteen (54%) patients received steroids in the IPA group as opposed to 27% in the patients without IPA (p < 0.025, Chi square). More significantly, 30% of patients in the IPA group were receiving high dose prednisone (more than 20 mg/d) compared with 7% in the non-infected group (p < 0.004).
Nosocomial infections
A summary of the surgical patients with HA IPA is shown in Table 2. All patients had critical illness as indicated by the Charlson score for the non-trauma patients and the Injury Severity Score for the trauma patients. A review of areas where the patients were housed during their hospitalization was performed carefully. Because the majority of patients presented with infection and were housed in different intensive care units (ICUs), no relation between their location and acquisition of their infection was found.
Discussion
This study was undertaken to investigate a possible outbreak of Aspergillus in ICU patients. Over a seven-year period, 117 patients were found to have a positive Aspergillus culture from a sputum or bronchoalveolar lavage specimen. Once IPA criteria were applied, 33 critically ill patients were identified with IPA. The overall mortality rate was 27%, within the literature reported range of 8% to more than 50% [5–7], depending on the duration of the follow-up. After the IPA determination was made, however, no evidence of an outbreak was found. What was remarkable about this study was that virtually all patients with CA IPA had chronic underlying lung disease and were receiving outpatient steroid therapy, whereas all HA IPA occurred in surgical patients.
In general, patient populations most susceptible to IPA are those undergoing bone marrow or solid organ transplantation, those with prolonged neutropenia, those on high dose corticosteroids, those with advanced acquired immune deficiency syndrome, and those with chronic granulomatous disease [8,9]. It has been estimated that the risk of development of IPA is approximately 10 times higher in patients undergoing transplant than in other susceptible populations [1].
Invasive fungal infections are a rare but increasingly frequent microbial infection in critically ill surgical patients, including burn patients [1,10–13]. A recent study at a university hospital by Davies et al. [10] found that 11 of their cases of IPA occurred in transplant patients and 12 occurred in non-transplant patients. In the former group, 36% were CA and 27% were ICU acquired, whereas in the latter group, 8.3% were CA and 83% were ICU acquired. In our community hospital, no patient had an organ transplant as a risk factor, 27 patients with CA IPA involved patients with chronic lung disease, and six of six patients with Hospital Corporation of America-associated IPA were surgical patients with the infections occurring in the ICU. Both of these studies are consistent with the concept that a small subgroup of ICU surgical patients are immunocompromised sufficiently for IPA to occur.
A number of recent studies have reported on Aspergillus infections in ICU patients not traditionally considered immunocompromised [10,14–19]. Some investigators have suggested that the immunosuppression in these ICU patients may be a consequence of sepsis [20]. Lange et al. [21] found that T-cell activator inhibitors were increased in sepsis/shock in ICU patients, and their levels correlated with death, suggesting a possible explanation for the immunodepression in some ICU patients. Further work will need to be performed to better understand the nature of the immunocompromised state that predisposes certain surgical patients to IPA.
While there are limited scientific data to support this conjecture, the degree of humidity in the region likely played a role in the incidence of the Aspergillus infestations. South Carolina is a rural state in the third largest water sheds on the East Coast [22]. A seasonal variation was seen in our data, with a peak incidence during the winter planting season, presumably related to aerosolization of the fungal spore [15].
Conclusion
The majority of our IPA were CA and occurred in patients with chronic lung disease receiving chronic systemic or inhaled steroid treatment. All nosocomial cases of IPA occurred in surgical ICU patients who were not thought initially to be immunosuppressed. We believe there is an ICU subpopulation that has, as yet, acquired a poorly characterized immunosuppression defect. The drawback to this study is that it is a small study in a single institution. It appears to confirm, however, a growing number of other small studies that suggest further study is warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.