
Abstract
Abstract
Background:
The role of surgery in abdominal tuberculosis is being redefined, as many patients will be candidates for endoscopic dilatation rather than open surgery.
Methods:
A retrospective analysis was done of the surgical procedures performed in patients with abdominal tuberculosis in a large tertiary-care center in North India. Details such as clinical presentations, previous history of tuberculosis, any anti-tubercular therapy (ATT), Mantoux skin test results, and the surgical procedures and findings were recorded. Short-term outcomes also were analyzed.
Results:
Thirty-five patients (26 male) were included, and the median age at presentation was 24 years (range 12–80 years). Sixteen patients had received prior ATT for abdominal tuberculosis. The indication for surgery was intestinal obstruction, perforation, and bleeding in 23 (66%), 10 (29%), and 2 (6%) respectively. Twenty-eight patients had intestinal strictures, with the ileum being the most common site (n = 21). Perforation was present in 10 patients, of which six had multiple perforations. Cocoon abdomen was present in four patients, two of whom had associated small-bowel stricture. Among 33 patients who underwent bowel resection, 14 had ileo-cecal resection/right hemicolectomy. The rest had small-bowel resection. Primary anastomosis and stoma creation was performed in 12 (36%) and 21 (64%), respectively. Post-operative intra-abdominal collections (p = 0.02) and incision dehiscence (p = 0.05) were more common in patients having stoma creation.
Conclusion:
Surgical intervention is warranted in a subset of patients with abdominal tuberculosis and may be required in patients with recurrent intestinal obstruction or pain, intestinal perforation, or gastrointestinal bleeding.
A
With the advent of reliable diagnostic tools, better imaging studies, and endoscopic techniques, the likelihood of diagnosing abdominal tuberculosis pre-operatively has increased [1]. However, the diagnostic sensitivity of histologic and microbiologic tools remains low [1]. The majority of patients can be managed successfully with effective anti-tubercular therapy (ATT) [4,5]. In a recent series of cases of intestinal tuberculosis, however, only half of the patients with intestinal tuberculosis had complete symptom resolution, and the rates of stricture resolution was still lower (a quarter of the cases) [6]. These patients may need surgery for recurrent abdominal pain and intestinal obstruction if endoscopic dilatation is not feasible or unsuccessful. Apart from these groups of patients, a considerable proportion of patients with no prior ATT present with surgical emergencies such as perforation and obstruction. In an endemic region such as India, 10% of surgical emergencies are secondary to tuberculosis [7].
Therefore, surgery remains an important tool for the treatment of a subset of patients with abdominal tuberculosis to handle emergency situations or alleviate persistent symptoms. The aim of this study was to analyze the spectrum of abdominal tuberculosis presenting to a tertiary-care center and management of various cases.
Patients and Methods
The study was a retrospective analysis of a prospectively maintained database of patients admitted to the Department of General Surgery and Gastroenterology between January 2015 and October 2017 with a definitive or presumed diagnosis of abdominal tuberculosis. We describe the indications for surgery, the surgical procedure, the histologic findings, and the outcomes in these patients.
Diagnosis of abdominal tuberculosis
The diagnosis of “definite” abdominal tuberculosis was made in patients with clinical, imaging, or endoscopic evidence of gastrointestinal (GI) involvement and at least one of the following: (1) acid-fast bacilli (AFB) on smear or culture of biopsies [8]; (2) caseating granuloma on histologic evaluation in operative or pre-operative tissue [8]; or (3) classical intra-operative findings of tuberculosis with suggestive histology (granulomas) in the resected area or lymph nodes.
The diagnosis of “probable tuberculosis” was made if there was strong clinical suspicion based on clinical, radiologic, endoscopic, and suggestive histologic features (granuloma without caseation) with exclusion of other differential diagnoses and confirmed if there was objective response to treatment (in the form of ulcer healing with ATT) or suggestive intra-operative findings [9].
Tubercles or yellow-white miliary nodules over the parietal or visceral peritoneum were considered classical findings of tuberculosis [10]. Intra-operative findings considered suggestive of tuberculosis were: (1) single or multiple centric stricture with adjacent lymphadenopathy; (2) mass-forming lesions of the ileo-cecal region with biopsy negative for malignancy; (3) thick membrane-encasing bowel loops (cocoon); (4) or bowel perforation with any of the above findings.
Patient work-up and management
All patients underwent baseline investigations that included complete hemogram, renal and liver function tests, and chest radiograph. Other findings such as a previous history of tuberculosis, family history of tuberculosis, positive Mantoux skin-test results, and human immunodeficiency virus (HIV) serology were recorded. Patients with suspicious chest radiographic findings underwent a computed tomography (CT) scan of the chest. Exploratory laparotomy or laparoscopy was performed. Resection of the diseased segment was done in patients having intestinal perforation, stricture, or mass. Adhesiolysis was performed in patients with an abdominal cocoon. Any associated strictures of intestinal lesions in patients with a cocoon were managed with resection of the diseased segment. Stoma creation or primary repair/anastomosis was left to the discretion of the surgeon. Multiple biopsies were taken from lymph nodes and peritoneum when involvement was suspected. Patients with no history of ATT were subjected to six months of such therapy post-operatively. Those patients on ATT requiring surgery completed six months of ATT. The standard antitubercular regimen included four drugs; i.e., isoniazid (H), rifampicin (R), ethambutol (E), and pyrazinamide (Z) for two months followed by HR (E) for four months. The patients were followed up every month. We used weight-based therapy and the patients received their drugs through the directly observed treatment, short course (DOTS) strategy from the national program.
Operative findings
Morphologic patterns for intestinal tuberculosis were described as stricturing (strictures and narrowing), ulcerative (bleeding or perforation), and mass formation or pseudo-tumoral forms. Any nodal involvement was recorded. The patient status was divided into two groups (peritoneal and intestinal) on basis of the operative findings and clinical features. Restoration of bowel continuity was done after the completion of ATT in patients who underwent stoma formation during the initial operation. Patients were placed on regular follow-up. Data regarding clinical details (demographics, clinical history, details of ATT, history of tuberculosis, physical examination), the indication for and type of surgical intervention, histopathologic findings, and outcome were analyzed.
Results
Clinical presentation
Patients with abdominal tuberculosis usually are treated in our Gastroenterology Unit. During this period, 119 patients were seen. Seventy-five had intestinal involvement, of which 48 (64%) had stricturing disease. Of these 48 patients, 22 continued to be symptomatic; and 10 underwent dilation of whom eight improved, and 14 underwent surgery. Apart from these patients, some presenting directly to us with perforation (with or without stricture), symptomatic abdominal cocoon, bleeding, or acute intestinal obstruction also underwent surgery. A total of 35 patients underwent surgery. The median age at presentation was 24 years (range 12–80 years), and the majority (n = 26) were male. Clinical and demographic profiles are depicted in Table 1. Of the findings on chest radiographs, three patients had evidence of active disease (cavity in two and consolidation in one), and three patients had fibrotic changes suggestive of remote infection.
ATT = anti-tubercular therapy; SD = standard deviation.
All patients had abdominal pain, and 24 had a history suggestive of sub-acute intestinal obstruction. The median pre-operative abdominal pain duration was one month (range one day–one year). Fourteen patients (40%) had an acute presentation. Ten of the 16 patients with confirmed abdominal tuberculosis had completed the six months of ATT. One patient defaulted after completing two months of treatment after symptom resolution. The mean Body Mass Index (BMI) of the study population was 20.89, with two patients undernourished (BMI <18.5). Abdominal CT examination done in 24 patients. The pre-operative findings were cocoon in three patients, strictures in 17 patients (Fig. 1), mass-like lesions in four patients, and abdominal lymphadenopathy in 15 patients, with hypodense centers in five patients and calcification and free fluid in one patient each. On presentation, ten patients had signs of peritonitis. Eight patients were in shock at presentation (seven with perforation and one with GI bleeding) requiring inotropic support and blood transfusion. An abdominal lump was palpable in seven patients, and ascites was present in only one patient. None of them was positive for retroviral infection.
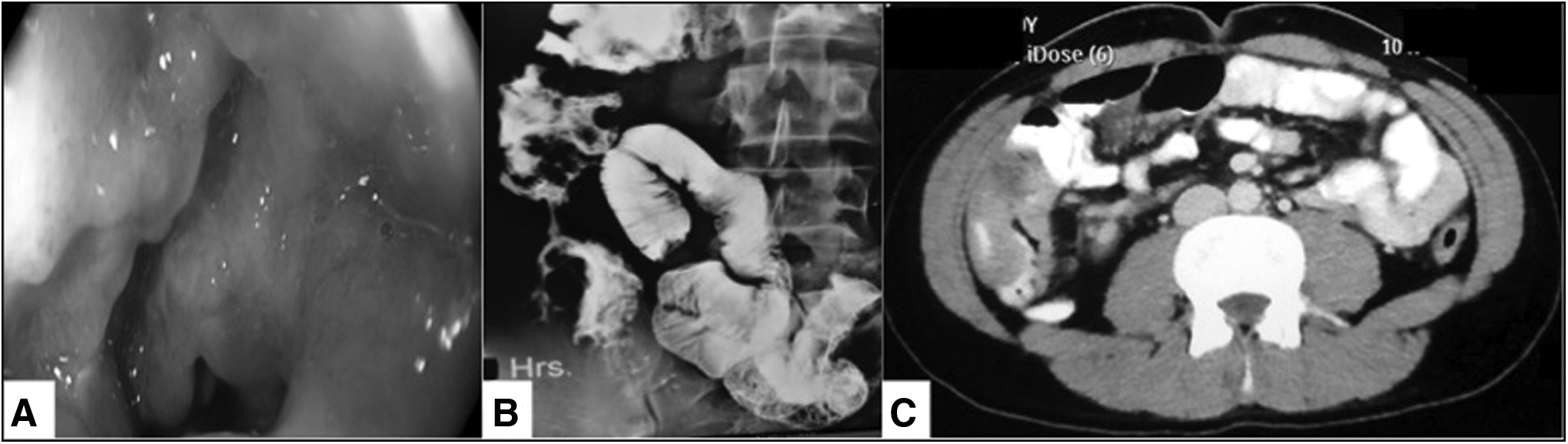
Stricture associated with abdominal tuberculosis. (
Surgical procedure and outcomes
The most common indication for surgery was intestinal obstruction (66%) followed by perforation (29%) and bleeding (6%). Details of surgery are shown in Table 2. Of the 35 patients, 32 underwent exploratory laparotomy, and three had laparoscopic resections (two right hemicolectomy and one ileo-cecal resection). At the time of exploration, stricture was the most common finding, being present in 80% (n = 28). Small-bowel strictures constituted 67% of the total strictures. Only one patient had an isolated ascending colon stricture. Twelve patients (43%) had multiple strictures Four were found to have a membrane around the bowel loops consistent with abdominal cocoon. All of these underwent adhesiolysis, and two also had small-bowel resection and stoma creation for associated small-intestinal pathology. The two patients operated on for lower GI bleeding had intra-operative enteroscopy for localization of the bleeding. One of them had ulceration in the distal ileum, and the other had an ulcerative lesion in the cecum warranting small-bowel resection and ileo-cecal resection, respectively. Among the 14 patients with ileo-colic resection, eight had primary anastomosis, and six had stoma creation.
SD = standard deviation.
The mean post-operative hospital stay was 11.25 ± 4.67 (standard deviation [SD]) days. The incidence of post-operative complications was 69% (n = 24). The most common complication was incision dehiscence, accounting for 43% (n = 15). A lower BMI (<18.5) and stoma creation were associated with a higher incidence of post-operative intra-abdominal collection formation (p = 0.01). Two patients died, and both had undergone resection and stoma creation for multiple ileal perforations with disseminated peritoneal tubercles. They succumbed to persistent sepsis and multi-organ dysfunction on the second post-operative day in one case and the third post-operative day in the other.
We performed a subgroup analysis comparing the patients who underwent stoma creation with those having primary anastomosis. The former were likely to have a shorter duration of abdominal symptoms (p < 0.01) and underwent surgery on an emergency basis (p = 0.01). Of the 21 patients who underwent stoma creation, 20 had an emergency operation for acute obstruction or perforation, whereas of those who did not need stoma creation, the majority of operations (n = 8) were elective. Underlying factors for surgical intervention affected the need for creation of a stoma (p = 0.007). All patients except one with a perforation underwent stoma creation, whereas none of the patient with a mass-forming infection needed a stoma. Among the patients with a stoma, the incidence of perforation as the indication for operative intervention and post-operative intra-abdominal collection was higher (p = 0.02 in both cases). All four patients operated on for failed ATT administered for an ileo-cecal mass had a primary anastomosis with one case complicated by incision dehiscence (Table 3).
Statistically significant differences are in
SD = standard deviation.
Histopathologic examination (confirmed and probable TB)
A total of 76 specimens from the 35 patients were subjected to histopathologic evaluation. On the basis of this examination, 19 patients had confirmed tuberculosis (caseating granuloma and/or AFB positivity). Overall, an additional 12 patients with findings of probable tuberculosis as judged by histology examination had characteristic operative findings, and therefore, 31 patients had confirmed tuberculosis.
Therapy for abdominal tuberculosis
A total of 16 patients had a recent history of ATT for abdominal tuberculosis. Fifteen had strictures, with nine patients having multiple strictures. The incidence of multiple strictures was significantly higher in patients with prior ATT than in those without prior therapy (9/16 vs. 3/19; p = 0.05). The rest of the lesions (mass, cocoon, and perforation) were similarly common in patients with and without prior therapy. The immediate post-operative outcome also was similar in both the groups. Of the 16 patients who had received previous ATT, nine had a partial clinical response, and seven had no response.
Follow-up
As mentioned previously, there were two deaths. Also, three patients were lost to follow-up. At a median follow-up of 10 months, 13 patients had undergone restoration of bowel continuity after completion of ATT. Five patients are still receiving ATT. All patients had complete symptom resolution and gain in weight.
Discussion
Recent evidence suggests that standard ATT for six months is effective for patients with abdominal tuberculosis [4,5]. In intestinal tuberculosis, the response to ATT is judged by mucosal healing; i.e., healing of ulcers. The strictures, polyps, and hypertrophic lesions may persist and dictate the appropriate intervention (Fig. 2) [9]. However, the rates of stricture resolution are variable. Although the study by Anand et al. suggested that the majority of patients (91%) improve with ATT, more recent studies suggest lower clinical and stricture resolution rates [6,11,12]. Therefore, a subset of patients with intestinal tuberculosis will be candidates for endoscopic dilation, surgical intervention, or both. Endoscopic interventions are likely to be difficult for small intestinal strictures and long and multiple strictures and in patients with obstruction secondary to mass-forming (pseudotumoral) lesions. Indeed, a majority of our surgical cases had small-bowel strictures, which were multiple. Less than half of these strictures had evidence of granulomatous inflammation, and only two had AFB demonstrated in the intestinal specimen. In all patients with no evidence of granulomatous inflammation of the intestine, partial response or histologic evidence was noted in the lymph nodes or peritoneum (Fig. 3). Thus, the partial response was secondary to resolution of the edema and acute inflammation and replacement by progressive fibrosis resulting in symptomatic luminal narrowing. Further, we had four cases with mass-forming lesions needing surgical intervention in the form of resection of the diseased area.

Hypertrophic and polypoid lesion. (

Involvement of lymph nodes. (
The other indication for surgical intervention in our patients was GI perforation. Perforation in intestinal tuberculosis could result from dilation of bowel loops proximal to a tight stricture or deep ulceration related to disease action. A component of mesenteric vasculitis may contribute to ischemia leading to ulcer breakdown [13]. These patients may present acutely with severe pain and peritonitis in the presence or absence of preceding abdominal complaints. Further, two of our patients were operated on for GI bleeding. Tuberculosis has a tendency to cause vascular involvement of various types (hypervascularity, narrowing, occlusion), and therefore, bleeding may occur in an active ulcerative form [13]. However, multiple studies from India on obscure GI bleeding have suggested tuberculosis as one of the important underlying diagnoses, implying that tuberculosis is an important cause of GI bleeding in tropical countries such as India [14,15]. As in our patients, intra-operative endoscopy should be done in an otherwise-unevaluated patient to provide guidance to the appropriate surgical management.
Another underlying condition necessitating surgical intervention was abdominal cocoon formation. Although historically considered a surgical entity, some recent evidence suggests that conservative therapy may help in symptom resolution in a majority of cases [3,16]. Further surgery for abdominal cocoon is difficult and associated with a need for enterotomies and stoma creation with a stormy post-operative course. Indeed, two of our patients with cocoons needed intestinal resection [17].
Interestingly, none of our patients had underlying HIV infection. The reported incidence of HIV co-infection with abdominal tuberculosis is 14%–50% [18–20]. In this group of co-infected patients, the diagnosis of tubercular infection is difficult because of the overlap of symptoms and immune modulation and possible occurrence of other opportunistic infections. Abdominal tuberculosis in HIV may be associated with more systemic symptoms, ascites, and lymphadenopathy and more AFB smear positivity but similar complication and mortality rates [21]. Emergency surgical intervention in these patients is associated with high morbidity and mortality rates [22]. We also analyzed our data for the patients who underwent primary anastomosis rather than stoma creation. It is apparent that these two surgical approaches should be considered complementary, and the clinical situation should guide the choice. None of the patients had leak-related complications despite histologic evidence of active tuberculosis. Stoma creation thus should be done on the basis of the general condition and hemodynamic status of the patient and not merely on the extent and activity of abdominal tuberculosis. The decision in our series was left to the operating surgeon, and apparently those needing emergency surgery or operated on for perforation had a greater need for a stoma, possibly related to poor general condition and fecal peritonitis. The presence of tubercles should not dissuade the surgeon from performing an anastomosis. Prediction of those tubercular strictures resulting from symptomatic luminal narrowing during treatment is difficult. We had a significant proportion of patients who underwent surgery for multiple strictures after failing to respond to ATT. Multiple strictures are less likely to respond to ATT than are a single stricture [6,12,23,24]. Among the various endoscopic findings of colonic tuberculosis, luminal narrowing is the least responsive to ATT [11]. Despite the probable higher rate of failure of medical therapy in strictures, ATT remains the first line of treatment. However, patients with features of bowel obstruction should be counselled and monitored for a requirement for surgery [14].
In conclusion, the surgical audit of the patients in an endemic region who underwent surgery for abdominal tuberculosis highlights the various presentations of the disease. Although ATT remains the first choice in tubercular strictures, these patients might have a higher requirement for surgery. Associated poor socio-economic factors make appropriate patient education and ensuring adherence to medical therapy mandatory.
Footnotes
Author Disclosure Statement
No funding was provided for this study. The authors have no conflicts of interest with regard to the manuscript.