
Abstract
Abstract
Background:
An integral part of ventilator-associated pneumonia (VAP) therapy is the appropriate choice of empiric antibiotics. Our previous experience demonstrated adherence to an empiric therapy pathway was associated with only modest changes in organisms causing VAP. The purpose of the current study was to evaluate the impact of a restrictive antibiotic policy for VAP in trauma patients on the incidence and sensitivities of causative pathogens since the previous study.
Patients and Methods:
Patients with VAP diagnosed on bronchoalveolar lavage since the previous study were stratified by age, gender, mechanism of injury, and injury severity. All patients received empiric antibiotics based on duration of intensive care unit (ICU) stay using a unit-specific pathway. The incidence and sensitivities of causative pathogens in the current study were documented. The adequacy of the VAP pathway was evaluated for all VAP episodes. The current study was then compared with the previous study.
Results:
Over a 10-year period, 1,474 episodes of VAP were diagnosed with 2,387 causative pathogens isolated. Overall incidence of gram-positive and gram-negative VAP pathogens was unchanged between the study periods. The current study experienced an increase in the incidence of Staphylococcus aureus (23% vs. 17%, p = 0.001) and methicillin-resistant Staphylococcus aureus (10% vs. 6%, p = 0.002) compared with the previous study. The pathway for empiric antibiotics resulted in adequate empiric coverage in 85% of VAP episodes, which was improved compared with the previous study (76%, p = 0.024). Furthermore, despite the increased incidence of early methicillin-resistant Staphylococcus aureus (MRSA) VAP, adequacy of the pathway improved for both the early period (91% vs. 86%, p = 0.001) as well as the late period (86% vs. 63%, p < 0.001) in the current study compared with the previous study.
Conclusions:
A comprehensive protocol for the diagnosis and management of VAP, along with antibiotic stewardship, can prevent the development of bacterial resistance to empiric therapy.
V
Multiple studies have demonstrated increased mortality in those patients receiving inadequate empiric antibiotics (i.e., no in vitro activity against causative pathogens), underscoring the importance of choosing the appropriate antibiotics for empiric VAP coverage [4]. Consequently, there is well-defined management algorithm for both the diagnosis and management of VAP at our institution that has been modified and refined since its inception. Specifically, our empiric antibiotic coverage was tailored to address causative pathogens based on intensive care unit (ICU) length of stay: early period defined as seven days or less in the ICU and late period defined as more than seven days in the ICU [5–15].
It is clear that optimal diagnosis and appropriate choice of empiric antibiotic agents remain two of the most important facets of VAP management. For more than two decades, empiric antibiotic agents (dictated by length of hospitalization) for our VAP clinical pathway have remained unchanged. In order to ensure optimal empiric therapy for VAP, periodic evaluation of causative pathogens is vital. In 2005, a study from our institution demonstrated adherence to our empiric therapy was associated with only modest changes in organisms causing VAP [4]. The purpose of the current study was to evaluate the impact of a restrictive antibiotic policy for VAP in trauma patients on the incidence and sensitivities of causative pathogens since the previous study.
Materials and Methods
Identification of patients
Data on all patients admitted to the trauma ICU at the Presley Regional Trauma Center in Memphis, Tennessee, who developed VAP over a 10-year period ending in May 2016 were entered into a prospectively collected database. Collected information included all cultured organisms, quantitative colony counts, sensitivities, and timing of cultures.
Consecutive patients surviving more than five days post-injury with VAP diagnosed on BAL subsequent to the previous study were identified and stratified by age, gender, mechanism of injury, and injury severity (as evidenced by Injury Severity Score [ISS]). Additional data regarding the incidence and sensitivities of each causative pathogen were recorded. These data were then merged with additional patient information from the trauma registry (NTRACS version 4.1, Digital Innovations, Forest Hill, MD) to compile the database for this study.
Diagnosis and management of VAP
The diagnosis and management of VAP at our institution follows a previously described algorithm [3]. Determination of VAP was made by quantitative culture of BAL fluid obtained by flexible fiberoptic bronchoscopic examination (Fig. 1). The clinical triggers for BAL included a new or changing infiltrate on chest radiograph, abnormal temperature (>38°C or <36°C), abnormal white blood cell count (>10,000 cells/mm3 or <4,000 cells/mm3), and grossly purulent sputum. Presence of any three of these clinical indicators prompted bronchoscopy with BAL. In fact, BAL was only performed for this clinical trigger and the diagnosis of VAP required bacterial colony counts equal to or greater than 105 colony-forming units per milliliter (CFU/mL) in the BAL effluent. No episodes of VAP were diagnosed in the absence of BAL.
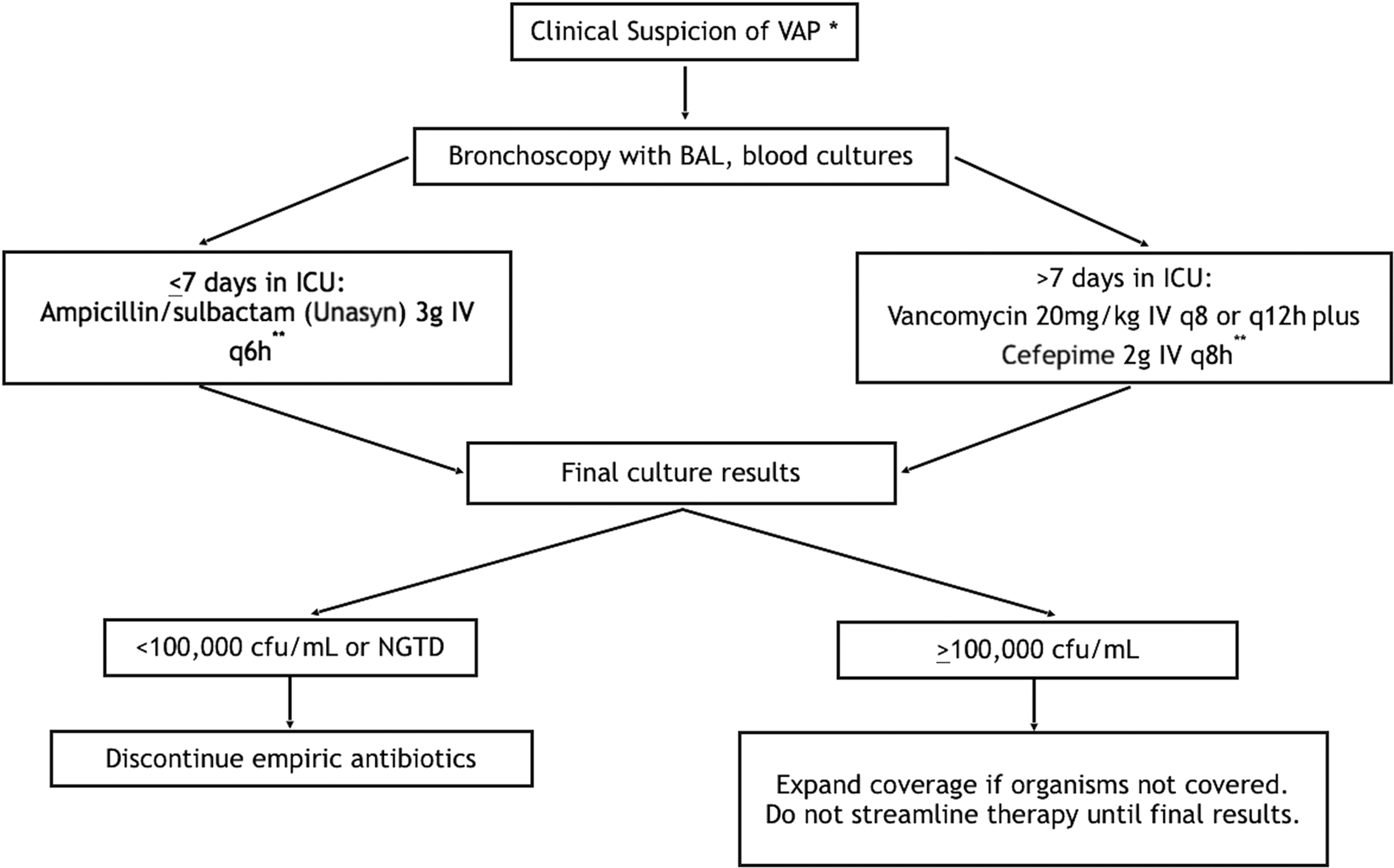
Clinical pathway for the diagnosis and empiric management of ventilator-associated pneumonia. *Defined as any three of the following: appearance of a new or changing infiltrate on chest radiograph; abnormal temperature (>38°C or <36°C); abnormal white blood cell count (>10,000 cells/mm3 or <4,000 cells/mm3 or the presence of more than 10% immature bands); macroscopically purulent sputum. **If severe β-lactam allergy, change: Unasyn® (Pfizer, New York, NY) to levofloxacin 750 mg IV every day, cefepime to ciprofloxacin 400 mg IV every eight hours or aztreonam 2 g IV every eight hours; dosage adjustment may be necessary based on renal function. VAP = ventilator-associated pneumonia; IV = intravenous; BAL = bronchoalveolar lavage; ICU = intensive care unit; NGTD = negative to date.
All BAL procedures were performed in a uniform manner by the attending trauma ICU staff as described previously [2]. Briefly, after blind endotracheal suctioning through the ventilator circuit (performed twice to clear upper airway secretions), the bronchoscope is advanced into the lung segment without using suction where the radiographic changes are seen. With the bronchoscope appropriately positioned, 100 mL of non-bacteriostatic saline are instilled in sequential 20-mL aliquots and immediately aspirated. The effluent is then pooled and sent to the microbiology laboratory for gram stain, quantitative aerobic, and anaerobic culture and sensitivity.
Once the sample is sent, all patients received empiric antibiotics based on duration of ICU stay using a unit-specific pathway [5]. Patients in the ICU for seven days or less are started on ampicillin-sulbactam 3 g intravenous every six hours (or equivalent alternative in patient allergic to penicillin) and patients in the ICU longer than seven days received vancomycin 20 mg/kg intravenous every 12 hours plus cefepime 2 g intravenous every 12 hours. Vancomycin dosing was adjusted in all patients to achieve peak serum concentrations of approximately 40 mg/L and trough concentrations of 5–15 mg/L. Empiric antibiotic choice was driven by previous experience as well as periodic evaluation of unit-specific antibiograms [4]. Antipseudomonal monotherapy was used for those patients with suspected hospital-acquired VAP (late regimen) based on previous work at our institution [6,7].
If the quantitative BAL cultures returned with equal to or greater than 105 CFU/mL, antibiotic agents were continued (and adjusted/streamlined if necessary). If the cultures returned with less than 105 CFU/mL, patients were considered to have systemic inflammatory response syndrome and the antibiotic agents were immediately discontinued. Therapy was considered to be adequate if one or more antibiotic agent had in vitro activity against the causative pathogen. Duration of therapy was dictated by the causative pathogen and followed a well-defined management algorithm (Fig. 2) [8]. Briefly, those patients with early community-acquired VAP (methicillin-sensitive Staphylococcus aureus [MSSA], Haemophilus spp., and Streptococcus spp.) received seven days of antimicrobial therapy without repeat bronchoscopy [9]. Those with Pseudomonas VAP received 14 days of adequate antibiotic therapy without repeat bronchoscopy. Those with methicillin-resistant Staphylococcus aureus (MRSA), Acinetobacter, Stenotrophomonas maltophilia, or Enterobacteriaceae VAP underwent seven days of adequate antibiotic therapy. On day seven, a protocol bronchoscopy with BAL was performed. If quantitative cultures returned with less than 103 CFU/mL, antibiotic agents were discontinued for a total of 10 days of adequate antibiotic therapy. If cultures returned with greater than or equal to 103 CFU/mL, a full 14 days of antibiotic treatment was completed [8,10]. Although clinical and laboratory parameters after VAP diagnosis were monitored carefully, neither were used to determine resolution of pneumonia [8,11].
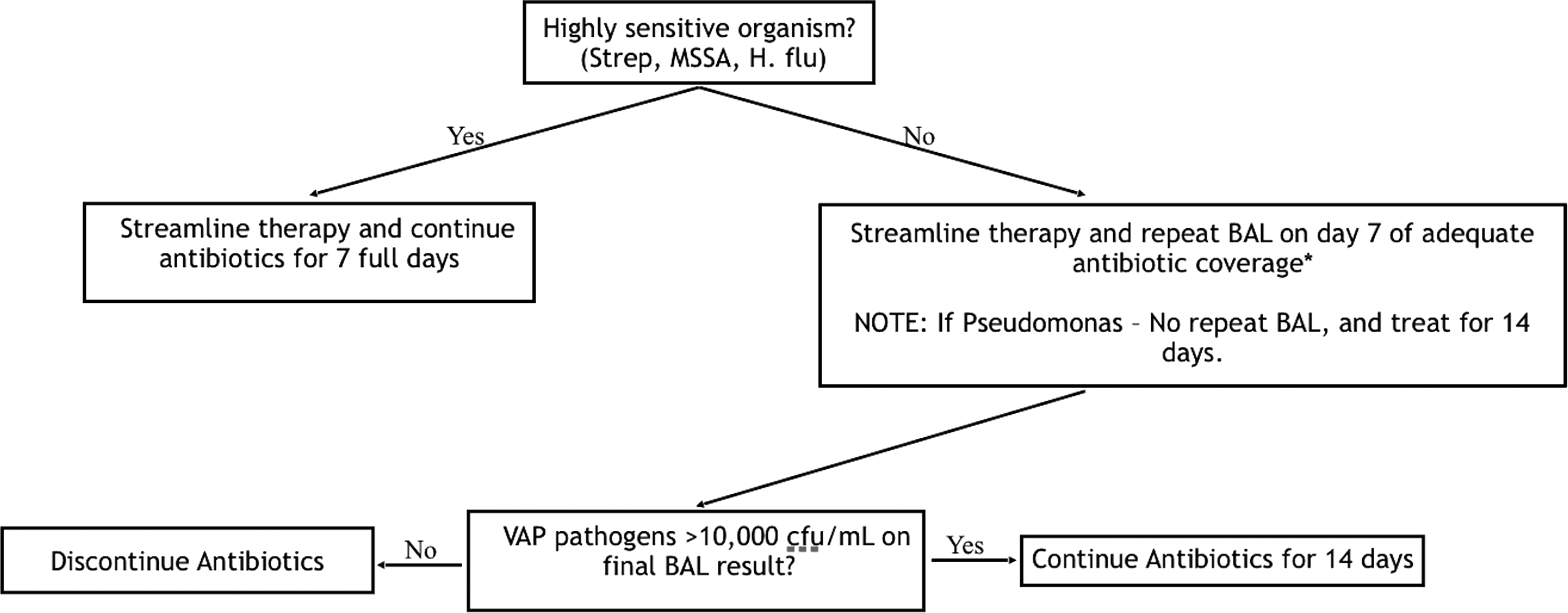
Clinical pathway for duration of definitive therapy for ventilator-associated pneumonia. *Adequate antibiotic therapy is defined as therapy with in vitro activity against the pathogen. MSSA = methicillin-sensitive Staphylococcus aureus; BAL = bronchoalveolar lavage; VAP = ventilator-associated pneumonia; H. flu = Haemophilus influenzae.
Comparison
Outcomes including ventilator days, ICU and hospital length of stay, risk factors for severe VAP (polymicrobial VAP), and mortality were recorded. The incidence and sensitivities of all causative pathogens in the current study were also documented. In addition, the adequacy of the VAP pathway was evaluated for all VAP episodes. The current study was then compared with the previous study.
Analysis
All data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC). Dichotomous data were compared using Student t-test and χ2 analysis or Fisher exact test where appropriate. Continuous data were compared using a Student t-test or Wilcoxon rank sum test where appropriate. Differences were considered significant at p < 0.05. The Institutional Review Board of the University of Tennessee Health Science Center approved this study.
Results
VAP episodes
Over the study period, 1,179 patients underwent 2,252 BALs. Based on quantitative culture results, 65.5% of suspected VAP episodes were diagnosed definitively as VAP with only 39.3% in the previous study (p < 0.001). A total of 1,474 VAP episodes were included in the current analysis. From the 1,474 VAP episodes, 2,387 causative pathogens were isolated. Overall incidence of gram-positive and gram-negative VAP pathogens was unchanged between the study periods. However, the most common pathogen isolated in the current study was Staphylococcus aureus (23%) compared with only 17% in the previous study (p = 0.001).
Patient characteristics
Patients in the current study ranged in age from 18 to 81 years old (mean age, 44) and included 884 males (75%) and 295 females (25%) and were clinically similar to those in the previous study with the exception of an increase in the number suffering blunt injuries (88% vs. 55%, p < 0.001) and a reduction in the number of polymicrobial VAP episodes (39% vs. 46%, p = 0.01). Despite this increase in blunt trauma, there was no significant difference in ventilator days, hospital and/or ICU length of stay, and overall mortality between the two study periods. In fact, in the current study, there was no statistical difference in mortality for those patients who received adequate empiric antimicrobial therapy compared with those patients who received inadequate empiric antimicrobial therapy (16% vs. 15%, p = 0.91). The characteristics of all study patients are shown in Table 1.
ISS = Injury Severity Score; IQR = interquartile range; ICU = intensive care unit; VAP = ventilator-associated pneumonia.
Incidence
Causative pathogens in the current study are compared with those from a previous study in Tables 2 and 3. The incidence of gram positives was increased in the current study compared with the previous study (38% vs. 34%) but that increase was not statistically significant (p = 0.065). However, the overall increase in gram positives was a direct result of an increase in the incidence of Staphylococcus aureus in the current study (23% vs. 17%, p = 0.001) compared with the previous study. Not surprisingly, the majority of the increase in Staphylococcus aureus was secondary to the increased incidence of methicillin-resistant Staphylococcus aureus in the current study compared with the previous study (10% vs. 6%, p = 0.002).
All numbers with the exception of n are expressed as percentages. All comparisons between current study and previous study are based on Total column only.
VAP = ventilator-associated pneumonia; MSSA = methicillin-sensitive Staphylococcus aureus; MRSA = methicillin-resistant Staphylococcus aureus.
All numbers with the exception of n are expressed as percentages. All comparisons between current study and previous study are based on Total column only.
There was a minor decrease in the incidence of gram negatives in the current study compared with the previous study (62% vs. 66%) but once again that decrease was not statistically significant (p = 0.065). In fact, the incidence of Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia remained unchanged (Table 3). This observation was consistent throughout all gram negatives, including both early and late periods.
Sensitivities
As reported above, there was an increase in the overall incidence of MRSA. This observed increase was primarily a reflection of an increase in the incidence of MRSA diagnosed during the first seven days of ICU stay (early) in the current study compared with previous study. In fact, the incidence of early MRSA VAP doubled between the two study periods (8% vs. 4%, p = 0.009). This finding is concerning because it directly impacts the adequacy of the empiric antibiotic regimen of the VAP pathway regarding early coverage.
The sensitivities for Pseudomonas aeruginosa and Acinetobacter baumannii in the current study are reported in Table 4 and compared with the previous study. Susceptibility patterns to cephalosporins, extended-spectrum penicillins, aminoglycosides, and fluoroquinolones were unchanged for Pseudomonas aeruginosa. However, there was minor improvement in the sensitivity of Acinetobacter baumannii to imipenem/cilastatin in the current study compared with the previous study (85% vs. 78%, p = 0.17).
Adequacy of VAP pathway
Ninety-five percent (1,400/1,474) of VAP episodes were treated with empiric antibiotics that fit the pathway and were therefore included in the adequacy analysis. The primary reason for exclusion was enrollment in a clinical trial (n = 55), followed by request of a consulting service for broader coverage based on their operative procedure (n = 19). Consequently, the pathway resulted in adequate empiric coverage in 85% of VAP episodes. Not surprisingly, adequacy was better in the early period (91%) compared with the late period (86%). The most common organism not covered by the early regimen (as indicated above) was MRSA and Enterobacter sp. The most common organisms not covered by the late regimen were multi-drug–resistant Acinetobacter baumannii and Stenotrophomonas maltophilia.
Table 5 compares appropriate empiric antibiotic coverage (%) for both the previous study as well as the current study by early and late VAP onset for gram-positive and gram-negative pathogens. Overall adequacy of the pathway improved in the current study compared with previous study (85% vs. 76%, p = 0.024). In addition, despite the increased incidence of early MRSA VAP, adequacy of the pathway improved for both the early period (91% vs. 86%, p = 0.001) as well as the late period (86% vs. 63%, p < 0.001) in the current study compared with the previous study and these changes were statistically significant.
All numbers are expressed as percentages.
Discussion
Antimicrobial resistance continues to increase within the spectrum of micro-organisms causing VAP, thus rendering these infections more difficult to treat [12]. Previous literature has demonstrated clearly that delay in appropriate antibiotic therapy for VAP is associated independently with patient mortality, and early adequate empiric therapy is the most important factor in preventing morbidity and mortality from VAP [13]. In the current study, continued adherence to an empiric antibiotic regimen for VAP was associated with minimal changes in organism incidence and sensitivities over the last decade.
In our clinical pathway for empiric management of VAP, the early period is defined as the first seven days in the ICU. Many institutions utilize a much shorter time interval (up to four days) to define the early period. In 2010, McMillian et al. [14] reviewed the utility of their antibiotic regimen within an early period, defined as the first four days. Similar to our institution, the authors utilized ampicillin-sulbactam as empiric therapy in the early period. However, McMillian et al. [14] found a high rate of resistance (40%) to empiric ampicillin-sulbactam for the treatment of VAP starting at day three and concluded they must weigh the benefits of using a broader spectrum antibiotic against the risk of introducing multi-drug–resistant organisms into their ICU.
In our previous study, we found that resistant organisms were not common in even our more inclusive definition of an early period (seven days) [4], and our current data demonstrates ampicillin/sulbactam is still adequate early empiric therapy at our institution. These results seem to contradict nationwide trends. Interestingly, the American Thoracic Society/Infectious Disease Society formerly recognized ampicillin-sulbactam as an appropriate empiric regimen for VAP diagnosed within the first four days of hospitalization [15]. However, the societies have since changed their guidelines to no longer differentiate between early and late VAP [16]. Fortunately, at our institution, the typical community-acquired pathogens (MSSA, Streptococcal sp., and Hemophilus influenzae) associated with early VAP have remained uniformly sensitive to ampicillin/sulbactam with a stable antibiogram.
Staphylococcus aureus remains one of the most common causes of VAP. Fortunately, the majority of these infections are secondary to MSSA [17]. However, there has been a significant increase in the incidence of MRSA in the community leading to a concomitant increase in MRSA as a cause of early VAP [18,19]. In fact, in the current study, the rate of MRSA in the early period doubled to 8% from 4% in the prior study. In 2012, we examined this changing trend in early MRSA VAP [17] at our institution and found that although the incidence of VAP secondary to Staphylococcus aureus did not change over the time period of that study, the incidence of early MRSA VAP did increase. Nevertheless, despite this finding, early MRSA VAP did not lead to increased mortality over patients with MSSA VAP and our empiric coverage was not altered. In fact, after adjustment for age, ISS and 24-hour transfusion requirements, early MRSA was not an independent predictor of mortality (odds ratio, 0.815; p = 0.59) [17]. However, this increase in early MRSA is concerning and warrants periodic evaluation for the need to broaden early VAP coverage.
Other institutions have had better luck with the incidence of MRSA VAP. In 2010, the Denver group demonstrated a remarkably low incidence (2.2%) of MRSA VAP during the early period (defined as zero to four days) at their institution [20]. A more recent study from Lollar et al. [21] also revealed a low incidence of early MRSA VAP of only 2.8%. The observed discrepancy of early MRSA VAP among institutions is likely caused by geographically varying rates of MRSA colonization in the local population. Interestingly, despite this reportedly low incidence in early MRSA VAP at other institutions, guidelines have changed to broaden empiric coverage [16].
In the current study, adherence to our empiric antibiotic regimen allowed for stable sensitivity patterns for all late pathogens, including the potentially virulent Pseudomonas aeruginosa and Acinetobacter baumannii organisms. This adherence to the restrictive policy allowed for improvement in the adequacy of the late empiric antibiotic regimen over the time period of the 2 studies. These results correspond with previous literature from our institution. In fact, in 2008, we demonstrated consistently following a unit-specific pathway for empiric management of VAP decreased the number of episodes of inadequate empiric therapy, ultimately reducing resource utilization and hospital mortality [5].
Limitations
The major limitations of this study include, first, the retrospective design. This precludes the exclusion of selection bias and unevaluated differences as potential confounding variables. In addition, this allows only for associations to be made, and cannot account for potential confounding differences between the previous study and the current study. Second, the generalizability of the study may be limited by both the fact that the patients were all treated at a high-volume level I trauma center that aggressively screens for VAP and follows a well-proven algorithm for the diagnosis and management of VAP. Finally, because this study examined patients from a single trauma ICU, application of the results to other critically ill populations should be done cautiously. This is especially true with regard to local patterns of susceptibility and to non-trauma populations, who have been shown to have worse VAP outcomes when compared with critically ill trauma patients.
Other institutions should evaluate their own antibiograms to determine which antibiotic therapy would be the most appropriate empiric regimen. In addition, the application of a disciplined protocol (similar to that presented in this study) could be applied to reduce emergence of antibiotic resistance and improve outcomes of VAP in institutions with similar patient populations.
Conclusions
Continued adherence to the current empiric antibiotic regimen employed in the VAP clinical pathway was associated with only minor changes in the causative pathogens. In addition, these antibiotics continue to provide adequate empiric coverage in the majority of VAP episodes. Periodic institutional review of antibiotic resistance patterns is imperative to assess continued efficacy of empiric therapy. A comprehensive protocol for the diagnosis and management of VAP, along with a policy of antibiotic stewardship, can prevent the development of bacterial resistance to empiric therapy.
Footnotes
Author Disclosure Statement
None of the authors have any competing financial interests to disclose.