
Abstract
Abstract
Background:
To evaluate the effectiveness of an antibiotic regimen for prostate biopsy by analyzing patients who were hospitalized because of complications after transrectal ultrasound-guided prostate biopsy.
Methods:
We reviewed retrospectively the medical records of 10,339 patients who underwent transrectal ultrasound-guided prostate biopsy at our institution from May 2003 to April 2017. We excluded patients with low quality data. All patients underwent urine culture before transrectal ultrasound-guided prostate biopsy and received intravenous antibiotic agents 30–60 minutes before biopsy. Patients were either given prophylactic quinolone or cephalosporin (second or third generation). Clinicopathologic factors including patient age, antibiotic regimen, number of biopsy cores, body mass index, prostate specific antigen, prostate volume, and infection-related complications that required hospitalization were subsequently analyzed.
Results:
A total of 9,487 patients were included in the final analysis, of whom 33 patients (0.35%) were hospitalized because of infection-related complications. Infection-related hospitalization rates were lower in patients who received cephalosporin (0.2%) than in patients who received quinolone (1.59%). At our institution, cephalosporin has been used predominantly to prevent post-biopsy infections since February 2013. Only five patients (0.12%) developed infection-related complications of the 3,863 patient who underwent transrectal ultrasound-guided prostate biopsy since February 2013. Multivariable analysis revealed that use of second- or third-generation cephalosporin was the only independent predictor of infection-related complications.
Conclusion:
Implementing an effective antibiotic prophylaxis regimen at our institution by using second- or third-generation cephalosporin could reduce infection-related complications after transrectal ultrasound-guided prostate biopsy.
P
Of the many possible infection-related complications after TRUS-PBx, sepsis is the most feared and life-threatening complication. The incidence of urosepsis after TRUS-PBx is increasing from less than 1% 20 years ago to almost 2%–3%, according to recent studies [7,8]. Infectious complications after TRUS-PBx are germane to fluoroquinolone-resistant Escherichia coli, because the prostate needle biopsy penetrates the rectal mucosa, which is laden with bacterial flora [9]. As a result of the recent emergence of quinolone-resistant Escherichia coli and its close association with post-operative sepsis, current antibiotic prophylaxis recommended by the Cochrane Review should be re-assessed [10].
We previously conducted a study in which we reviewed retrospectively 5,215 patients who underwent TRUS-PBx at our center to evaluate various clinico-pathologic risk factors, and concluded that the use of prophylactic cephalosporin may decrease infection-related complications after TRUS-PBx [11]. Based on these previous results, and other recent studies, the cephalosporin-based antibiotic regimen has become the standard prophylactic regimen for patients who undergo TRUS-PBx at our clinic. This current study aims to evaluate the effectiveness of the revised cephalosporin-based antibiotic regimen for prostate biopsy, which has been used predominantly at our institution since February 2013.
Patients and Methods
Patient population
After obtaining approval from our Institutional Review Board (IRB) (B-1708/412-007), we reviewed the medical records of 10,339 biopsy-naïve patients who underwent TRUS-PBx at our institution between May 2003 and April 2017 to analyze the clinical outcome of initial systematic prostate biopsy (Fig. 1). Of these patients, we excluded 434 patients who underwent magnetic resonance imaging (MRI)/ultrasound fusion-guided biopsy; 119 patients whose records were insufficient; 86 patients who were prescribed antibiotic agents other than quinolone or second- or third-generation cephalosporin; and six patients who had fewer than six biopsy cores. Additionally, 207 patients whose prostate-specific antigen (PSA) level was over 100 ng/mL were not included in the study. We ultimately retrospectively analyzed the data from 9,487 patients who underwent multicore random TRUS-PBx between May 2003 and April 2017. Of these, 1,007 took prophylactic quinolone and 8,480 took second- or third-generation cephalosporin.

Flow diagram of patient selection.
Antibiotic regimen and biopsy technique
Urine analysis and cultures were performed on all patients approximately one to three weeks before they underwent TRUS-PBx. For those patients who were suspected to have an urinary tract infection based on this analysis, TRUS-PBx was postponed until the patients recovered fully. All patients received a glycerin enema for bowel preparation before the biopsy. All patients received intravenous antibiotics 30 to 60 minutes before the biopsy was performed. Patients were either given prophylactic quinolone (levofloxacin, 750 mg; ciprofloxacin, 400 mg; or moxifloxacin, 400 mg) or prophylactic second- or third-generation cephalosporin (cefotetan, 1 g; cefuroxime, 750 mg; ceftriaxone, 1 g; ceftizoxime, 1 g; or cefotaxime, 1 g).
All patients underwent TRUS-PBx under local anesthesia and stayed in the hospital for several hours to one day in order to monitor possible complications after the procedure, such as rectal bleeding, severe lower urinary tract symptoms (LUTS), high fever, etc. Two experienced expert radiologists at our institution performed standardized multicore random biopsies on patients who were placed in the left lateral decubitus position. All patients were made aware of possible TRUS-PBx complications by dedicated nurses in the department when they were discharged. Patients were told to return promptly to the hospital if they experienced any of the following symptoms: severe bleeding, a high fever, severe LUTS, or urinary retention.
Data analysis
After the IRB approval from the ethics committee at our institution, all patients' data were collected and handled by professional data managers. The entire set of data was anonymized and then analyzed retrospectively. Receiving signed patient consent for the current study was not required because the study was conducted retrospectively. Infection-associated hospitalizations because of complications after TRUS-PBx were defined as a postponed discharge, an emergency department visit, or a new admission to the urologic department within two weeks after the biopsy. This research adhered to the requirements of Helsinki Declaration and the reference number IRB is B-1708/412-007.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences® 22.0 software (IBM Corp, Armonk, NY). Student t-test and χ2 tests were used to compare the clinico-pathologic variables for the entire cohort. Univariable and multivariable logistic regression analyses for the infection-associated hospitalization after TRUS-PBx were performed. All p values were two-sided and values <0.05 were considered to be statistically significant.
Results
A total of 9,487 patients of the original cohort with 10,339 biopsy-naïve patients who underwent TRUS-PBx at our institution between May 2003 and April 2017 were included in the final analysis. The patients' clinico-pathologic characteristics are described in Table 1. The mean age of the cohort was 64.9 ± 9.3 years and the median PSA level was 6.6 ng/mL (interquartile range [IQR]: 4.3–10.5). Among these patients, 1,007 patients (10.6%) were given prophylactic quinolone, whereas 8,480 patients (89.4%) were given second- or third-generation cephalosporin for prophylaxis. Of these patients, 20.7% in the cephalosporin group (n = 1,967) took second-generation cephalosporin, and 68.7% (n = 6,513) took third-generation cephalosporin. Before February 2013, 28 patients (0.54%) developed post-biopsy infectious complications and were re-admitted to the hospital [11]. After implementing the revised antibiotic prophylaxis regimen of treatment with second- or third-generation cephalosporin after February 2013, only 0.12% of patients (5/3,863 patients) developed post-biopsy infectious complications (Fig. 2). Therefore, 33 patients (0.35%) of the entire cohort developed post-biopsy infectious complications that required hospitalization.
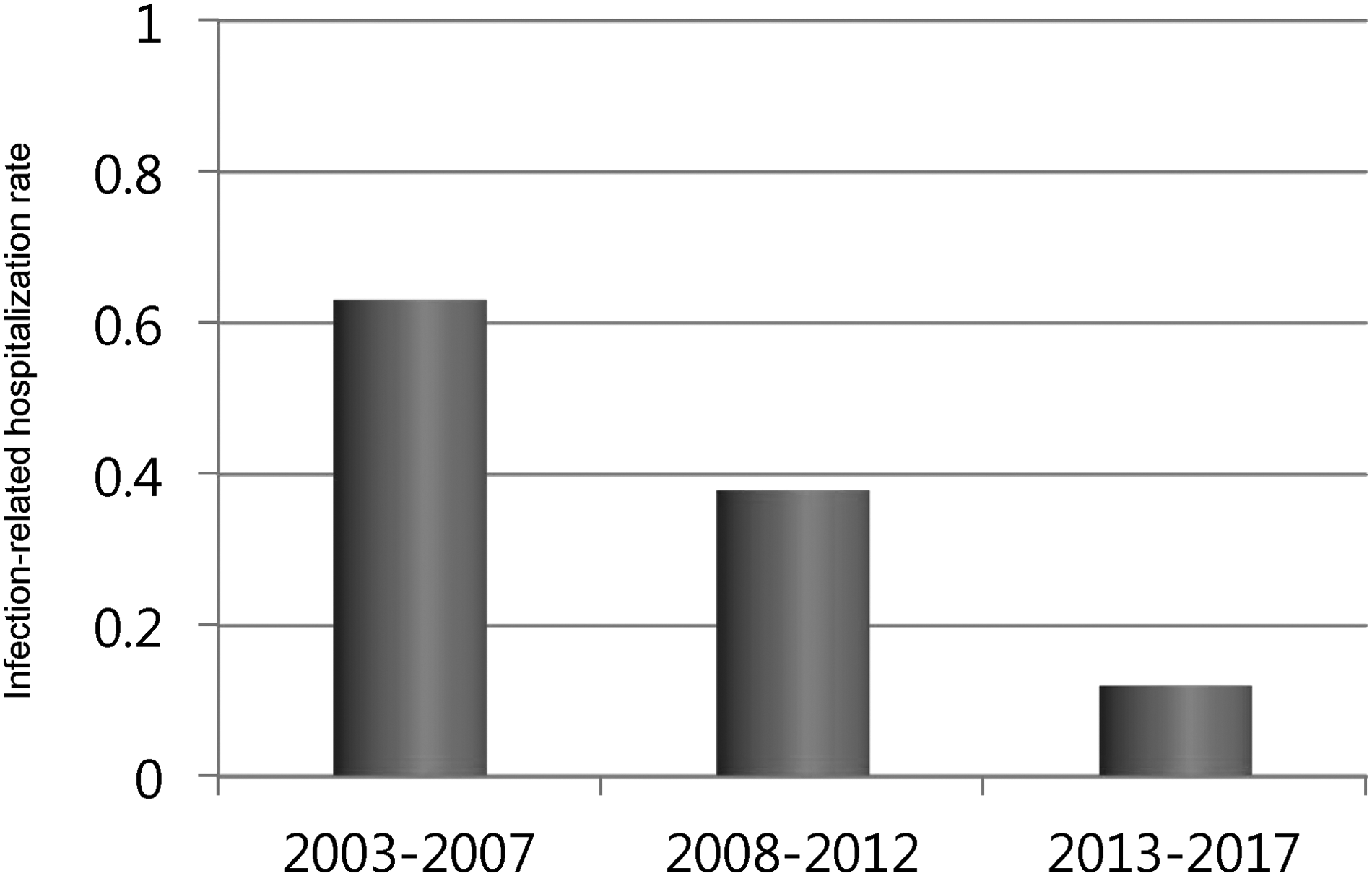
Infection-related hospitalization over time.
BMI = body mass index; PSA = prostate-specific antigen; IQR = interquartile range; IPSS = International Prostate Symptom Score.
The infection-related hospitalization rate of patients who took quinolone and cephalosporin was 1.64% and 0.2%, respectively. Clinical features of patients who were hospitalized because of infectious complications after biopsy and the results of their blood culture tests are shown in Table 2. Of the 16 patients in the quinolone group, there were 10 cases of quinolone-resistant Escherichia coli and one case of Enterococcus infection. Three patients experienced septic shock in the quinolone group, which led to one death. Of the 17 patients in the cephalosporin group, there were four cases of Enterococcus, one case of Escherichia coli, one case of coagulase-negative staphylococcus (CoNS), and one case of Klebsiella pneumoniae. Interestingly, there were no episodes of septic shock or mortality in the cephalosporin group.
CoNS = coagulase-negative staphylococcus.
According to univariable logistic regression analysis for the infection-associated hospitalization after TRUS-PBx, these factors were significant independent predictors of infection: patients who were 70 years or older (odds ratio [OR] = 0.033, 95% confidence interval [CI] 0.934–0.998, p = 0.001), prophylactic antibiotic regimen of second-generation cephalosporin (OR = 0.032, 95% CI 0.004–0.238, p = 0.001) or third generation cephalosporin (OR = 0.153, 95% CI 0.076–0.306, p < 0.001; Table 3). However, according to the multivariable logistic regression analysis for infection-associated hospitalization after TRUS-PBx, the antibiotic regimen of second-generation cephalosporin (OR = 0.121, 95% CI 0.016–0.937, p = 0.043) or third generation cephalosporin (OR = 0.133, 95% CI 0.061–0.289, p < 0.001) were the only significant predictors of the infectious complications requiring hospitalization after the prostate biopsy (Table 3).
PSA = prostate specific antigen; BMI = body mass index; IPSS = International Prostate Symptom Score.
Discussion
Prostate needle biopsies are widely performed both in Korea and worldwide, including in the United States. Although prostate needle biopsy with a transrectal approach has been considered a generally safe procedure, recent studies found that post-operative complications occur more frequently than first predicted [6,12,13]. Over two decades, the infection-associated complication rate has almost tripled [13,14]. This increase has been associated with fluoroquinolone-resistant Escherichia coli [9,10]. Concerns have thus arisen about fluoroquinolone-resistant Escherichia coli and post-operative sepsis. It is therefore necessary to tailor antibiotic prophylaxis for prostate biopsy according to the bacterial susceptibility patterns at each institution [15]. To our knowledge, the present study is the largest single center study to evaluate the effectiveness of the antibiotic regimen for prostate biopsy by analyzing patients who were hospitalized because of complications after TRUS-PBx.
The revised antibiotic prophylaxis regimen at our institution, consisting of second- or third-generation cephalosporin, substantially reduced infection-related complications after TRUS-PBx (from 0.35% to 0.12%). Likewise, Pace et al. [16] reported that the re-admission rates after TRUS-PBx decreased from 5.7% to no incidence by adding 1 g ceftriaxone to the peri-prostatic lidocaine injection [16]. In the United Sates, Mehrad et al. [15] augmented their antibiotic regimen (three days of ciprofloxacin or Bactrim DS followed by one dose of pre-biopsy intramuscular gentamicin) and reported a 3.2% decrease in re-hospitalization rates (from 3.8% to 0.6%) [15]. Roberts et al. [17] reviewed studies from Turkey, Egypt, Spain, and Italy and reported that fosfomycin trometamol is more effective antibiotic prophylaxis for patients in reducing infections after TRUS-PBx than fluoroquinolone. Leahy et al. [18] assessed the prophylactic use of carbapenem after TRUS-PBx and found that there was no re-hospitalization for patients who received prophylactic carbapenem. Losco et al. [19] also assessed prophylactic ertapenem and reported that adding ertapenem to standard prophylaxis efficiently reduced post-operative sepsis after TRUS-PBx.
Interestingly, while the other parts of the world witnessed increased infection-associated complications after prostate biopsy [13,14], the infection-related re-admission rate (1.7%) in Australia, where fluoroquinolone prescription is restricted, did not show an overall increase in the five-year period ended in 2012 [20]. Moreover, the U.S. Food and Drug administration (FDA) warned about safety issues related to the side effects of fluoroquinolone use [21]. Furthermore, according to a recent study, Koreans have high fluoroquinolone resistance (54.9%) although fluoroquinolones are widely prescribed because of their good antimicrobial penetration into prostate tissues [22]. Also, Bidell et al. [23] analyzed nearly 10,000 hospital-associated urinary tract infections caused by Escherichia coli and found that third-generation cephalosporin resistance rates (8.6%) were only one-third of quinolone resistance rates (34.5%) regardless of geographic location or hospital. Because of the fluoroquinolone safety issues and increasing fluoroquinolone resistance, second- or third-generation cephalosporin are a more effective antibiotic prophylaxis. However, another overuse of a single antibiotic agent could lead to further resistant bacteria strains. In this regards, recent studies call for targeted antibiotic prophylaxis based on individual patient rectal swab results before prostate biopsy [10,24] although rectal swab cultures are limited because they are taken 24 to 48 hours before the biopsy [24]. Prior use of antibiotics and overseas travel should also be noted when tailoring prophylactic antibiotic agents to individual patients [24,25].
Despite numerous attempts to identify patient-specific risk factors related to infectious complications after prostate biopsy, pre-biopsy risk factors have not yet been evaluated conclusively [15,26]. In our previous study, the International Prostate Symptom Score (OR = 3.18, CI 1.24–8.13, p = 0.016) was an independent predictor based on multivariable analysis [11], whereas patient age of 70 years or older (OR = 0.033, 95% CI 0.934–0.998, p = 0.001) was the only independent predictor, other than use of second- or third-generation cephalosporin in this study. Our findings support the 2013 American Urological Association recommendations [27], in which PSA screening is recommended for men 55 to 69 years of age. However, it is necessary for clinicians to discuss the benefits and potential complications of PSA screening and prostate biopsy fully with patients.
Procedure-related risk factors, including number of biopsy cores [28–30] and number of the biopsy procedures during active surveillance [31,32], still remain controversial. Both in our previous study [11] and this study, the number of biopsy cores was not an independent predictor of infectious complications according to univariate and multivariate analyses. In a recent study, however, Papaqiannopoulos at el. [33] tried to identify independent predictors of infection-related post-biopsy complications after using targeted antibiotic prophylaxis and reported that the number of biopsy cores (OR = 1.28, 95% CI 1.04–1.54) was an independent predictor of infectious complications. Compared with its transperineal counterpart, transrectal biopsy is not a clean procedure: each needle core risks inoculating the prostate, genitourinary tract, or vessels with rectal bacteria [33,34]. In this study, we excluded MRI-fusion biopsies to evaluate accurately the effectiveness of our revised antibiotic regimen on contemporary systematic TRUS-PBx. However, with the development of MRI-fusion biopsies, it is increasingly possible to pinpoint tumors during the biopsy procedure with as few as one or two needle cores [34]. Further research is required on how many biopsy cores can be reduced using MRI-fusion prostate biopsy.
Our study has some limitations. First, the study was conducted retrospectively and thus is not designed as a double-blinded study. Second, our data were drawn from one cohort from a single center, and the majority of patients are of Asian descent. These facts limit generalizing the outcomes of our study to different ethnic groups. Third, even though all patients were educated about which TRUS-PBx complications require a hospital re-visit, there still may be events that were unknown to us. Fourth, in Korea, an inpatient stay is covered by national health insurance and 80.6% of the patients in our study are treated under inpatient settings. This may affect the outcomes of the study, because most patients rest in bed after the procedure under the supervision of registered nurses and physicians. Finally, when we empirically used cephalosporin-based antibiotics after TRUS-PBx, re-hospitalization rates because of infectious complications showed a statistically significant decrease. However, in order to prevent bacteria that are more resistant and harder to treat, it may be most desirable to use a targeted antibiotic regimen that is tailored to individual patients based on rectal swab culture, prior exposure to antibiotics, and overseas travel.
The antibiotic prophylaxis regimen at our institution, consisting of second- or third-generation cephalosporin, could significantly reduce infection-related complications after TRUS-PBx. A large-scale, multicenter prospective study is required to evaluate fully adequate antibiotic prophylaxis regimens for TRUS-PBx patients.
Footnotes
Acknowledgment
This research was supported by a grant of the Korean Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C1264).
Author Disclosure Statement
No competing financial interests exist.