
Abstract
Abstract
Background:
Laser hair depilation has shown promise in small series of patients with pilonidal sinus disease. The purpose of this study was to review the published literature on laser hair depilation in pilonidal disease to determine its effect on disease recurrence.
Methods:
The PubMed, Embase, and Cochrane Central Register of Controlled Trials databases were searched to identify all studies published through December 1, 2017 that examined the role of laser hair depilation in the treatment of pilonidal sinus disease. Study characteristics, including design, treatment regimen, number of patients evaluated, rate of recurrence, and duration of follow up were recorded.
Results:
Thirty-five published studies were included. Of these, 28 studies were retrospective and seven were prospective. There were five comparative studies: two retrospective, one prospective observational, and two randomized controlled trials. The number of patients included in each study ranged from one to 86 patients and patients received between one and 11 laser treatments. The pilonidal disease recurrence rate after laser depilation ranged from 0% to 28% at a mean follow-up ranging from 6 months to 5 years across studies. Four of the five studies that included a comparative group demonstrated a decreased recurrence rate compared to the non-laser cohort.
Conclusion:
Laser hair depilation is a promising therapy in the management of pilonidal disease. However, the literature published to date is heterogeneous and has limited generalizability. Additional research is needed to determine the effectiveness of laser hair depilation to prevent pilonidal disease recurrence.
P
Laser hair removal was first described as a therapy in the treatment of pilonidal disease in 2002 and works by the process of selective photothermolysis, which targets melanin in the hair follicles [9,10]. By selecting the appropriate light source, wavelength, pulse duration, and energy for the individual hair and skin type, the resulting thermal damage causes destruction of the hair follicles and impairs future hair growth [11,12]. Laser depilation may decrease pilonidal disease recurrence by decreasing the local hair concentration thereby eliminating the need for patients to perform difficult mechanical or chemical depilation at home [13].
Laser hair removal has been proven to be an effective depilation technique and is used commonly for cosmetic purposes, although its role in the management of pilonidal disease remains unknown. We performed a systematic review of all published literature examining laser hair depilation in the treatment of pilonidal disease to better understand its effect on disease recurrence.
Methods
Search strategy and study selection
Two authors (D.R.H. and A.O.) searched the PubMed, Embase, and Cochrane Central Register of Controlled Trials databases for relevant studies published through December 1, 2017. The search keywords in the title and abstract included “pilonidal AND laser,” “pilonidal AND ruby,” “pilonidal AND diode,” “pilonidal AND Nd:YAG,” “pilonidal AND intense pulsed light,” “pilonidal AND alexandrite,” “pilonidal AND epilation,” “pilonidal AND depilation,” “pilonidal AND hair removal,” and “pilonidal AND photothermolysis.” These searches were performed without any restriction on date or language and repeated until no unique publications were found. Where appropriate, a review of cited references was performed.
Eligibility criteria
We included both prospective and retrospective studies describing the use of laser hair depilation in the treatment of sacrococcygeal pilonidal disease. Abstracts and case series were also eligible for inclusion. We included research published prior to December 1, 2017. We excluded studies that examined the use of a laser device for reasons other than hair depilation, studies examining hair depilation for conditions other than pilonidal disease, and studies that investigated the use of laser hair depilation at locations other than the gluteal cleft. Editorials and reviews that did not present new patient data were also excluded. Two reviewers (D.R.H. and A.O.) independently judged the eligibility of each study while screening individual manuscripts. Disagreements were adjudicated by a third author (P.C.M.).
Data extraction and quality assessment
Two investigators (D.R.H. and A.O.) independently extracted the following data points from each eligible study: first author, year of publication, study design, patient population, number of laser treatments, interval between laser treatments, number of patients in the laser group, number of patients in the comparison group (if applicable), laser group disease recurrence rate, comparison group disease recurrence rate (if applicable), and duration of follow up. Both investigators assigned a Jadad score [14] and a Newcastle-Ottawa Scale (NOS) quality score to randomized controlled trials and cohort or case controlled studies, respectively [14,15]. A third author (P.C.M.) reviewed the data and resolved any discrepancies.
Results
Study identification and selection
A total of 150 studies were identified initially: 65 through PubMed, 85 through Embase, and 0 through Cochrane. Fifty-three duplicate studies were excluded. The remaining 97 publications were reviewed for eligibility. Of these studies, 45 were excluded because they did not evaluate laser therapy for the purpose of hair depilation, five evaluated patients who did not have sacrococcygeal pilonidal disease, and 12 publications were editorials or did not present new patient data. In total, 35 studies were included for our review (Fig. 1).
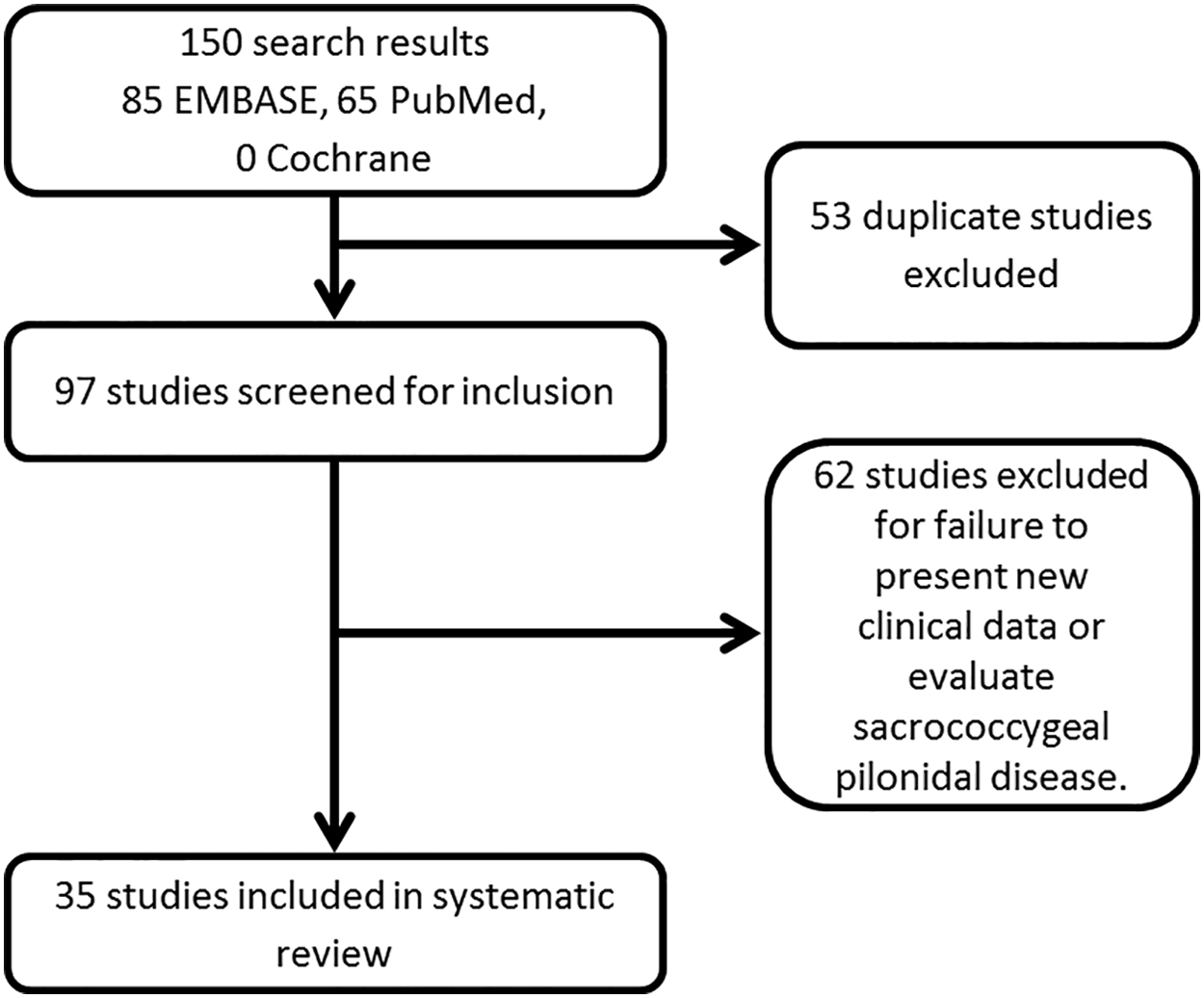
Study flow chart.
Study characteristics
Thirty-five studies were identified for analysis. An overview of these studies can be found in Table 1. Twenty-eight retrospective studies and seven prospective studies were identified, reporting on 552 total patients across all studies. There was considerable variability among the studies. Two of the seven prospective studies randomly assigned patients to laser hair removal and 26 of the 28 retrospective studies were case reports or case series. The duration of follow-up ranged from 6 months to 5 years. The number of patients included in each study ranged from one to 86 patients. The number of laser treatments administered to patients varied between one and 11 laser treatments. The patient population included in each study also varied markedly across the studies. Of the studies scored on the seven-point Newcastle Ottawa scale, two studies received a score of one, four received a score of two, 15 received a score of three, nine received a score of four, three received a score of five, and no studies received scores of six or seven. The two randomized controlled trials were both assigned Jadad scores of one out of five. A summary of the studies included in our review can be found in Table 2.
Recurrence
Because of the heterogeneity between study designs, treatments, controls, and follow-up, a meta-analysis of the results of these studies was not appropriate. Table 1 details the reported recurrence rate in each study. The recurrence rate ranged from 0% to 28% across the studies with 230 studies reporting no recurrences after laser therapy. Five studies included a comparative group, of which four of five studies demonstrated a decreased rate of recurrence in the laser cohort. Of note, only four of the 35 (11%) studies clearly defined the criteria used to indicate disease recurrence.
Discussion
Pilonidal disease is a morbid disease of the natal cleft caused in part by hair growth. Laser hair depilation has been described in small series as an adjunct in the management of pilonidal disease, although its effectiveness has not been demonstrated clearly. We performed a systematic review of the published literature to examine the effectiveness of laser hair removal to decrease disease recurrence in patients with pilonidal disease. Overall, the published literature has considerable limitations that restrict our ability to combine study results and draw reliable conclusions.
In general, there is a notable absence of well-designed, prospective studies in the published literature. Of the 35 studies identified, only seven evaluated patients receiving laser therapy for treatment of pilonidal disease prospectively, of which only three included comparison groups. Ghnamm and Hafez [16] and Demircan et al. [17] randomly assigned patients to receive laser hair depilation after surgical excision, whereas ile El-Ramah and Darwish [18] compared similar groups in a prospective, controlled fashion. The remaining four prospective studies did not include a control group against which to compare the effectiveness of the intervention. Of the 28 retrospective studies, only two included a comparative group, with the remaining 26 studies being case reports or case series. The majority of the published literature consists of retrospective reviews and studies lacking randomization or comparative groups which results in the potential for significant bias in the reported results and limits the ability to draw reliable conclusions. Prospective comparative studies with control groups receiving mechanical or chemical hair depilation as recommended by the American Society of Colon and Rectal Surgeons are needed to objectively demonstrate the effectiveness of laser hair removal [6].
In addition to the variability in study designs among the published studies, we noted a significant degree of variability in the patient populations evaluated. For example, nine studies evaluated the effectiveness of laser hair depilation in patients after surgical excision, whereas the remaining studies included patients with varying states of disease and previous surgical histories. The number and frequency of laser treatments also varied substantially between studies, ranging from one to two treatments separated by weeks to several months. Rarely did studies conduct multivariable analyses controlling for disease stage, surgical history, or other characteristics that would be expected to influence recurrence. This limitation may have been because of the small sample sizes, as the studies reported their experience with between one and 86 patients. As such, these were likely inadequately powered to control for these confounding variables. For example, one of the two randomized controlled trials randomly assigned patients to laser depilation after a wide excision that was left to heal by secondary intention [16]. They reported a 0% recurrence rate in the laser group compared with the control group that faced a 2.3% recurrence rate after two years. The disability caused by these large open wounds makes it an unattractive procedure for many surgeons and patients, particularly adolescents. This limits the generalizability of these results to the broader population of patients with pilonidal disease. Additional studies are needed to better understand the role of laser depilation in the treatment of pilonidal disease.
Recurrent disease is common in patients with pilonidal disease. All studies in our review reported the rate of recurrent disease in their laser cohort, which ranged from 0% to 28%. Among the five comparative studies, four reported a lower recurrence rate in the laser cohort [16,18–20]. There was significant heterogeneity in the definition of pilonidal disease recurrence with only four of the 35 studies describing their criteria for recurrence and no uniformity among these four definitions (Table 3). Furthermore, there was marked variability in duration of follow-up, which ranged from six months to five years. Although laser hair removal appears to be a promising therapy to decrease pilonidal disease recurrence, the marked disparity in methodologies and results across the available studies limit our ability to draw conclusions from this data.
The remaining studies did not define criteria for recurrence.
LE = laser epilation; IPL = intense pulse light.
The American Society of Colon and Rectal Surgeons recommends performing hair depilation in patients with pilonidal disease to minimize the amount of hair in the gluteal cleft and thereby decrease the risk of disease recurrence [6]. However, the gluteal cleft is a technically difficult area to depilate adequately at home using traditional techniques such as shaving and application of creams. Consequently, compliance with hair removal is low [8]. Laser hair removal reduces the concentration of hair in this area and will minimize the need for patients to perform hair removal at home. A recent systematic review by Pronk et al. [21] demonstrated a decreased rate of recurrence in patients after laser depilation compared with traditional techniques (9.3% vs. 23.4%). This review, although well done, was limited to studies that included 10 or more patients and reported on 378 patients in total. Our study is a comprehensive review of all studies reporting the use of laser depilation in the management of pilonidal disease and includes data on an additional 46% of patients.
Our analysis demonstrates a significant degree of heterogeneity of the published literature on this subject, thus limiting the ability to draw reliable conclusions from the work performed to date. Future studies should include patients randomly assigned to receive either laser hair depilation or other forms of hair depilation in patients at varying stages of disease in order to better understand the role of laser hair depilation in the management of pilonidal disease.
Conclusion
Laser hair depilation is a promising therapy in the treatment of pilonidal disease. Our review underscores the paucity of strong evidence in the literature to support this practice. Well-designed, adequately powered, prospective comparative studies with standardized outcome measures are needed to determine the effectiveness of laser hair removal in reducing the pilonidal disease recurrence.
Footnotes
Acknowledgments
Author contributions are as follows. Study conception and design: D. Halleran, A. Onwuka, A. Lawrence, B. Fischer, K. Deans, P. Minneci. Data acquisition: D. Halleran, A. Onwuka, A. Lawrence, B. Fischer. Analysis and data interpretation: D. Halleran, A. Onwuka, A. Lawrence, K. Deans, P. Minneci. Drafting of the manuscript: D. Halleran, A. Onwuka, A. Lawrence, B. Fischer. Critical revision: K. Deans, P. Minneci.
This project was supported by intramural funding from the Research Institute at Nationwide Children's Hospital.
Author Disclosure Statement
All authors declare that they have no competing financial interests relevant to the data contained in this manuscript.