
Abstract
Abstract
Background:
Surgical site infection (SSI) remains a persistent and morbid problem in colorectal surgery. A novel surgical device that combines barrier surgical wound protection and continuous surgical wound irrigation was evaluated in a cohort of elective colorectal surgery patients. A retrospective analysis was performed comparing rates of SSI observed in a prospective cohort study with the predicted rate of SSI using the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) Risk Calculator.
Patients and Methods:
A prospective multi-center study of colectomy patients was conducted using a study device for surgical site retraction and protection, as well as irrigation of the incision. Patients were followed for 30 days after the surgical procedure to assess for SSI. After completion of the study, patients' characteristics were inserted into the ACS-NSQIP Risk Calculator to determine the predicted rate of SSI for the given patient population and compared with the observed rate in the study.
Results:
A total of 108 subjects were enrolled in the study. The observed rate of SSI in the prospective study using the novel device was 3.7% (4/108). The predicted rate of SSI in the same patient population utilizing the ACS-NSQIP Risk Calculator was estimated to be 9.5%. This demonstrated a 61% difference (3.7% vs. 9.5%, p = 0.04) in SSI from the NSQIP predicted rate with the use of the irrigating surgical wound protection and retraction device.
Conclusions:
These data suggest the use of a novel surgical wound protection device seems to reduce the rate of SSIs in colorectal surgery.
S
The American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) is a validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care. The ACS NSQIP Risk Calculator is a tool that utilizes 21 pre-operative variables to estimate the likelihood that patients will experience complications within 30-days after operation, including SSI [13,14] The model utilizes data from more than 3.2 million operations available in the ACS NSQIP database [15].
A novel surgical device that combines barrier surgical wound protection and continuous surgical wound irrigation was evaluated previously in a cohort of elective colorectal surgery patients. The purpose of this study was to compare the SSI rate observed in a prospective multi-center pilot study to the predicted SSI rates for the same patient population using the ACS NSQIP Risk Calculator.
Patients and Methods
A retrospective analysis was conducted comparing the rate of SSI observed in a prospective cohort study to the predicted rate of SSI using the ACS NSQIP Risk Calculator. A multi-center pilot study of colectomy patients was conducted previously using a novel device for surgical wound retraction and protection, as well as irrigation of the incision (CleanCision Wound Retraction and Protection System, Prescient Surgical, San Carlos, CA) (Fig. 1). A total of 108 patients were enrolled in the previous study inclusive of both the roll-in and treatment groups between April 2015 and June 2016. Patients were followed for 30 days after operation to assess for SSI, per the Centers for Disease Control and Prevention definitions. The prospective study was approved by each participating site's Institutional Review Board. All patients provided informed consent.
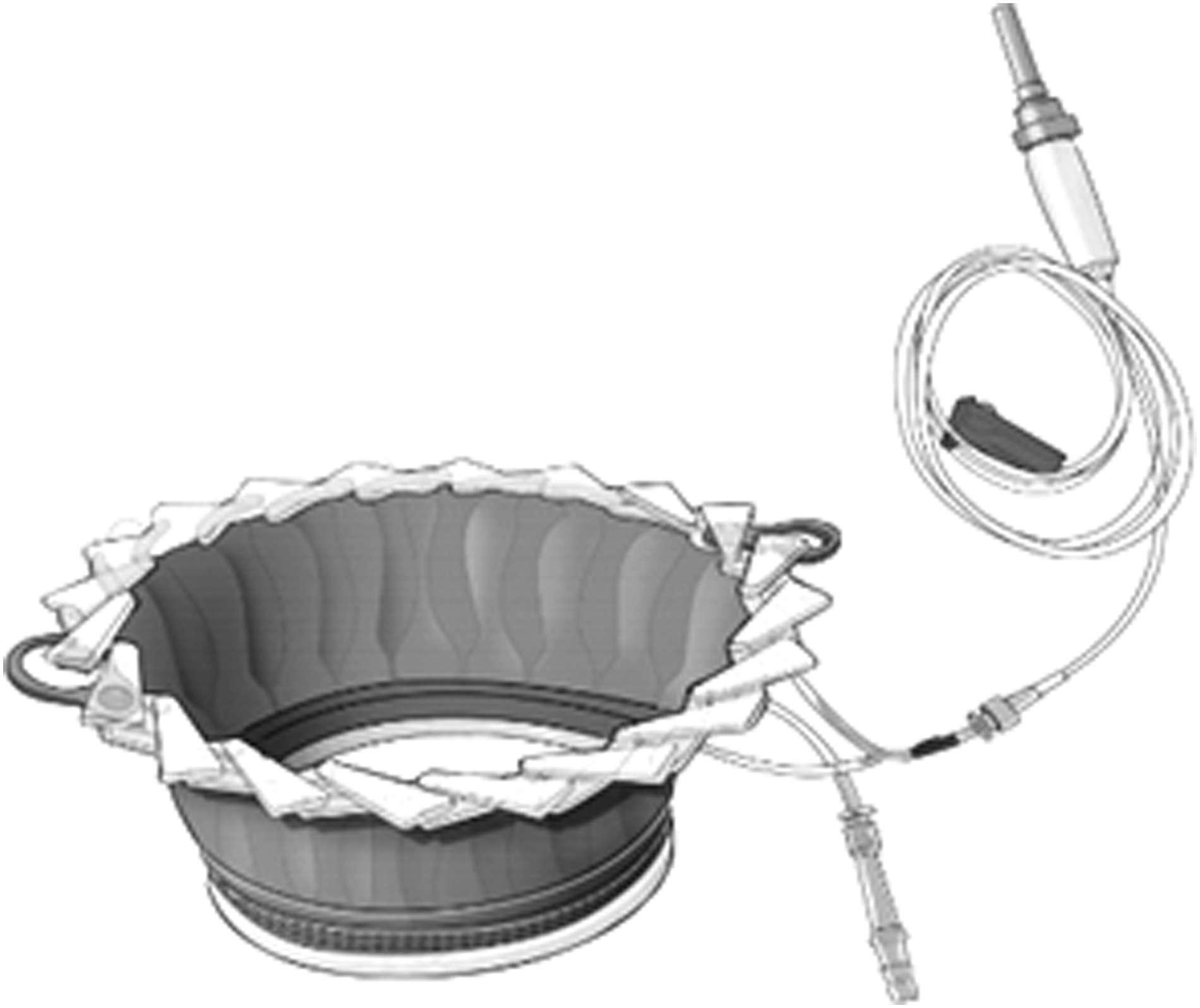
Surgical wound retraction and protection system.
After completion of the study, the patients' baseline demographic and procedure data were utilized to enter the pre-operative variables into the online ACS-NSQIP Risk Calculator to determine each patient's predicted SSI risk. The ACS NSQIP Risk Calculator only allows for a single procedure code to be entered. Therefore, for patients who had multiple colorectal procedures performed in a single operation, the procedure code with the highest risk was entered in the risk calculator. The mean predicted SSI risk from the ACS-NSQIP Risk Calculator for all patients was used to determine the predicted rate of SSI for the given patient population and compared with the observed rate in the study.
Statistical analysis
The predicted SSI rate was calculated by taking the mean predicted risk of SSI for all patients from the ACS NSQIP Risk Calculator. Statistical analysis was performed using a two-sided exact binomial test comparing the observed proportion of SSI from the cohort study with the predicted rate (mean SSI risk) from the ACS NSQIP Risk Calculator. A p < 0.05 was considered statistically significant. Statistical analysis was performed using SAS System software Version 9.4 (SAS Institute Inc., Cary, NC).
Results
A total of 108 patients were included. The mean patient age was 60 years, with 56% female and 44% male. Table 1 provides a summary of key patient characteristics. Key procedure characteristics including the type of colorectal resection and the access are listed in Table 2. The most common colorectal procedures were laparoscopic partial colectomy with anastomosis (CPT 44204), open partial colectomy with anastomosis (CPT 44140), open partial colectomy with removal of terminal ileum and ileocolostomy (CPT 44160), and laparoscopic partial colectomy with coloproctostomy (CPT 44207) at 53%, 11%, 7%, and 6%, respectively.
Patient Characteristics as Defined by National Surgical Quality Improvement Program Risk Calculator
BMI, body mass index; ASA = American Society of Anesthesiologists; COPD = chronic obstructive pulmonary disease.
Procedure Characteristics
HALS = hand-assisted laparoscopic surgery
Data shown as %/
There were four SSIs reported in the cohort study—two superficial incisional and two organ space. The overall observed SSI rate (superficial, deep, or organ space) was 3.7% (4/108). The patient characteristics of the 108 patients were inserted into the ACS-NSQIP Risk Calculator. The mean predicted rate of SSI in the same patient population utilizing the ACS-NSQIP Risk Calculator was 9.5% (standard deviation = 4.15%). This demonstrated a 61% difference in SSI between the NSQIP predicted rate (9.5%) and the observed rate (3.7%) with the use of the irrigating surgical wound protection and retraction device (p = 0.04). (Fig. 2) This equates to an observed/expected ratio of 0.39.
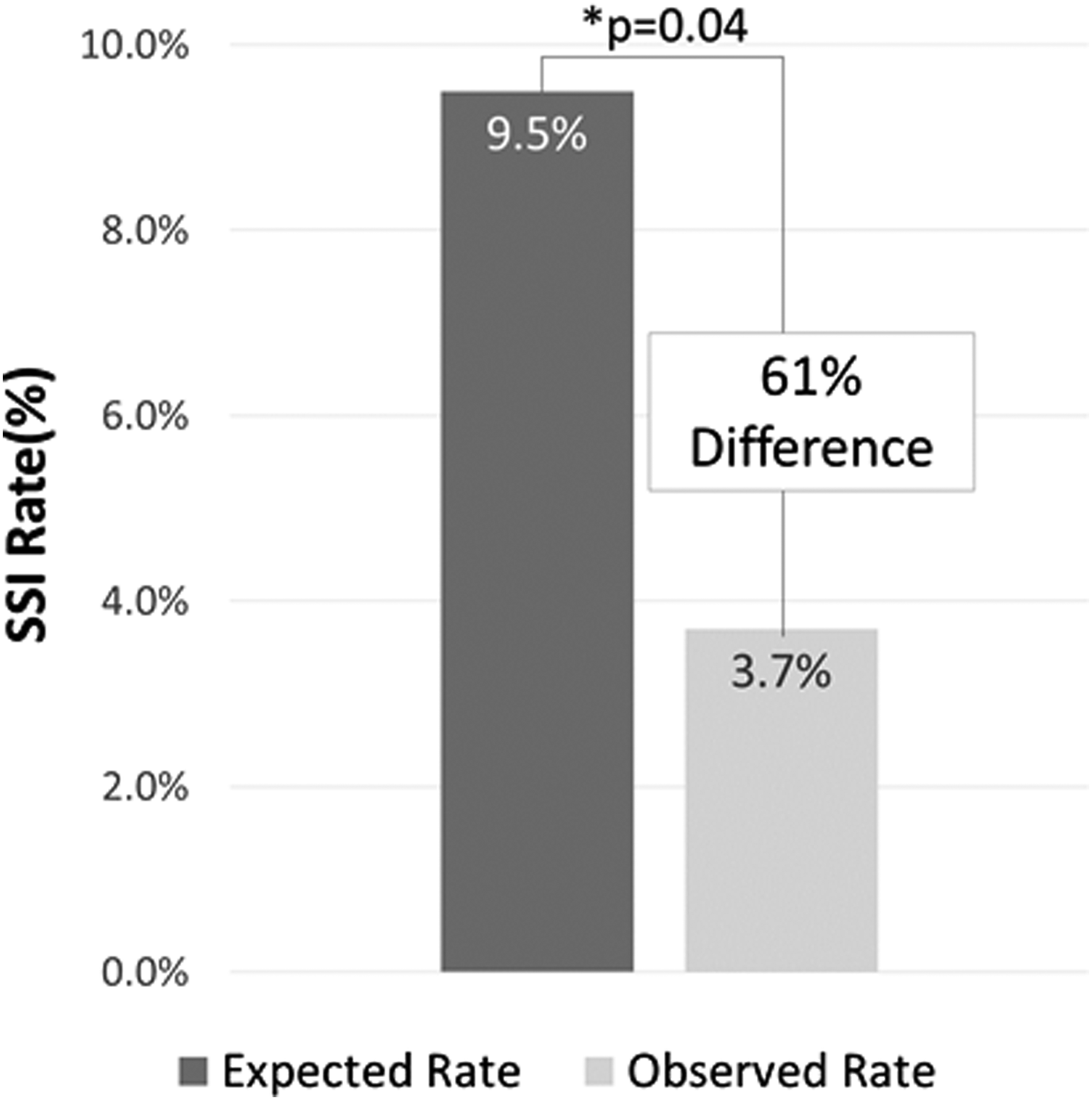
Observed versus expected rate of surgical site infection (SSI); N = 108.
Discussion
The ACS NSQIP Risk Calculator utilizes data from the NSQIP database. Therefore, it is representing the current standard of care used by hospitals, including any SSI prevention bundles that have been implemented. It is unknown whether the operations reported within the NSQIP database utilized a standard surgical wound protector; however, the use of a surgical wound protector in colorectal procedures has been adopted widely. The predicted SSI rate of 9.5% is on the lower end of the range of SSI rates reported in the literature for colorectal surgery (7%–25%) [1–6].
The accuracy of the ACS NSQIP Risk Calculator to predict outcomes has been assessed both broadly by ACS [15] and specifically in colorectal operations by single institutions [16,17]. Cohen et al. [15] reported a c-statistic for colorectal surgery of 0.6890. Lubitz et al. [16] reported that the Risk Calculator accurately predicted outcomes for elective colorectal operations, whereas Adegboyega et al. [17] reported that the risk calculator underestimated the risk of SSI and overall complication rates at their center.
It is possible that single institution studies do not permit the separation of model performance from local quality effects [15]. The benefit of this study was that there were seven institutions participating to reduce the impact of local effects. To determine whether the predicted rate was reflective of the institutions participating in the prospective study, a comparison was made to the NSQIP reported colorectal SSI rate for the centers participating in the prospective study. Of the seven participating sites, four had NSQIP data available. These four sites enrolled the majority (81%) of the patients in the prospective study.
In addition, the SSI rate within the prospective study for those four centers was 3/88 or 3.4%, which is representative of the SSI rate of the overall population of 4/108 or 3.7%. The mean NSQIP reported SSI rate for colorectal procedures during the same period as the clinical study across these four sites was 10.6%, which is similar to the predicted NSQIP Risk Calculator rate for the population enrolled in the study. This shows that the predicted rate of 9.5% is within range, and the risk level of the patient population enrolled in the study is likely representative of the general colorectal surgical population at these institutions.
There are several limitations of this study. First, this was a retrospective analysis. The data from the prospective study and NSQIP are both collected prospectively, however. Ideally, one would want to do a randomized trial on SSI, but this was not possible because of cost constraints. The second is that it utilizes the NSQIP Risk Calculator rather than data specific to the hospitals participating in the study. This was assessed by looking at the site-specific NSQIP reported rates for SSI, which were very similar to the results predicted by the ACS NQIP Risk Calculator. Third was that there were some assumptions that had to be made to enter the data into the ACS NSQIP Risk Calculator, because the Calculator only allows for a single procedure to be entered, and some of the definitions for the variables used as input into the calculator were not identical to the definitions of the prospective study.
Footnotes
Acknowledgments
The authors thank Lisa Claude, MS of Prescient Surgical for editorial support.
The initial prospective study was funded by Prescient Surgical, Inc.
Abstract presented as a poster at Western Surgical Association Annual Meeting, Scottsdale, Arizona, November 4–7, 2017.
Author Disclosure Statement
No competing financial interests exist.
Editor-in-Chief Disclosure Statement
The Surgical Infections Editor-in-Chief, Dr. Donald Fry, declares a consulting relationship with Prescient Surgical.