
Abstract
Abstract
Background:
Reports from high-quality healthcare systems have shown that active surveillance and management of factors associated with surgical site infection (SSI) decreased the incidence and improved overall outcomes.
Methods:
This study aimed to appraise the incidence trend of SSIs during the 10-year period between 2007 and 2016 in a university hospital in a middle-income country, focusing on six high-risk and high-volume procedures. The study also examined factors associated with SSIs and their impact on surgical outcomes.
Results:
A total of 10,139 procedures in 9,661 cases were reviewed. The overall incidence of SSI was 2.98%. The incidence increased substantially with increasing risk score according to the National Nosocomial Infection Surveillance (NNIS) system risk score. The incidence trend decreased over time during the 10-year period studied. The procedures with the highest SSI incidence were craniotomy, colonic surgery, and cholecystectomy, which were also the three procedures that had standardized infection ratios (SIR) higher than 1.0 in all risk score categories. Univariable analysis found that diabetes mellitus was the only risk factor associated with SSI (odds ratio [OR] 1.81, 95% confidence interval [CI] 1.2–2.73). The majority of the positive cultures were gram-negative bacteria (45%) and 49% of all reported organisms were drug resistant. There were two important consequences of the infections: length of hospitalization increased substantially from 13 days to 24 days (p < 0.01) and patients with SSI had more than three times higher mortality rate (7% compared with 1.9%, p < 0.001).
Conclusion:
With active surveillance, the incidence of SSIs decreased to less than 2.0% over the 10-year study period. More intensive surveillance should implemented for operations with high SIR and cases with diabetes mellitus.
Surgical site infections (SSIs), defined as infectious complications after a surgical procedure, are the most common hospital-acquired infections (HAIs) in low- and middle-income countries (LMICs) and are commonly caused by antimicrobial multi-drug–resistant micro-organisms (AMRs) [1]. Although SSI is known as the most preventable complications among HAIs, the associated complications have the highest impact on hospital stay, increased hospital expenditures, and also surgical morbidity and mortality worldwide [2,3]. The estimated annual cost for SSIs in Europe is $19 billion per year [1]. Surgical site infections have a higher prevalence in LMICs with an overall estimated incidence at more than 10%, at least two to three times higher than in high-income countries [1]. In Thailand, the reported incidence of SSIs is approximately 6%–8%, which is approximately 10% or the third most common HAIs after lower respiratory tract infections and urinary tract infections [4]. The problem is more severe in university hospitals or tertiary care settings and has been estimated to cost hospitals an additional cost of more than $1,224 per admission [5,6].
The European Centre for Disease Prevention and Control (ECDC) reported recently a decreasing trend in SSI incidence and suggested that active surveillance was the key success factor in SSI prevention [7]. The original landmark study on the efficacy of surveillance programs was first conducted in the United States in the 1970s [8]. Most of the subsequent studies from various levels of institution also reported a substantial impact in SSI reduction after initiation of a surveillance programs [8–12]. In our institute, an active SSI surveillance program was established in 1996 and has continued until now. Active surveillance, focusing on the six surgical procedures that were our highest risk and service volume patients was implemented in 2005 [5]. Selection of these index operation groups was based on our prior data of SSI rates and in-hospital expenditures. In subsequent years, SSI monitoring was integrated as a regular part of our surgical outcome measures.
Various endogenous and exogenous factors in the peri-operative process have potential risk for SSIs [13]. Risk scores, for example the National Nosocomial Infections Surveillance risk index (NNIS), have been constructed with an aim to predict and prevent SSIs although the influence of each factor may vary among institutions. A systematic review has demonstrated that high body mass index (BMI) and high NNIS were associated with an increased risk of SSIs [14]. Other parameters that have been reported as being associated with a higher risk of SSIs are diabetes mellitus, American Society of Anesthesiologists score (ASA score) of at least three, failure of administration of prophylactic antibiotic agents, trauma situations, re-operation, and low surgical volume [1,14–17]. Knowing the pattern of SSIs in an individual institute and the associated risk factors is helpful in monitoring and controlling the problem.
This study aimed to determine the incidence and trends of SSI in six selected surgical procedures highlighted for intensive monitoring by the infection control unit of our institution, namely coronary artery bypass grafting, cardiac surgery, mastectomy, cholecystectomy, colorectal surgery, and craniotomy. The study also analyzed for factors associated with SSIs and consequences of the complications.
Patients and Methods
The study had two parts: first, a retrospective study aimed at incidence and trend of SSIs in Songklanagarind Hospital, a tertiary care and medical teaching hospital of Prince of Songkla University and focusing on the trend of changes in the recent years. Included in this part were patients of the surgical department who underwent one of six selected operations in our hospital between January 1, 2007 and December 31, 2016. The SSI cases in this study were identified specifically from the database of the infection control unit. There was no fixed protocol for a pre-operative antibiotic regimen in our institute during the study period. However, prescription of imipenam, colistin, and vancomycin was available for internists who specialized in infectious diseases. Except for laparoscopic cholecystectomies, the majority of procedures were performed as open surgery. Diagnosis and classification of SSIs were based on standard definitions described by the U.S. Centers for Disease Control and Prevention (CDC) [18]. Wound classification also used the CDC criteria [19]. Prolonged operative duration was defined as the length of operation of more than the 75th percentile of the normal duration of each specific operation being performed [20]. Post-operative active surveillance was performed by full-time nurses trained specifically for hospital infection control. Follow-up was deemed completed at 30 days post-operatively when the patients came for their post-operative visit at the outpatient clinic.
Figures for SSIs in this study were normalized further using the standardized infection ratio (SIR), which was used to compare the incidence of SSIs to the NNIS systems database [21]. The SIR is the ratio of the observed number of SSIs that occurred to the expected number according to the NNIS. An SIR exceeding 1.0 indicates that the incidence of SSIs in that specific risk stratification was higher than expected, whereas an SIR of less than 1.0 indicates the opposite. The NNIS risk index, developed by the CDC in 1991, ranges from 0–3 points and is defined by three independent parameters. One point of risk index is scored for each of ASA physical status classification greater than 2, contaminated or dirty/infected wound class, and prolonged operative duration.
The second part of this study aimed to analyze the risk factors associated with SSIs, using a case control model. The controls were surgical cases performed in the same period with no SSIs. The cases and the controls were matched for surgical procedure and re-operation status to compose a case to control ratio of 1:3 by computer-generated matching using the R program [22]. Any cases that could not be matched were excluded from analysis. Collected data included patient demographic data, ASA physical status, presence of diabetes mellitus, BMI, smoking status, wound classification, organism culture, NNIS score, pre-operative antibiotic agents, type of surgery (emergency or elective), surgical procedure, operative time, hospital charges, length of stay (LOS), and survival status. The study protocol was approved by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University. Hospital expenditure figures in this study were converted from Thai baht to U.S. dollars using a weighted-average Interbank Exchange Rate of 32.659 baht/U.S. dollar (foreign exchange rates as of December 29, 2017).
Statistical analysis
Statistical analyses in this study included number and percentage, mean ± standard deviation, and median (quartile-1, quartile-3) (Q1, Q3) for descriptive statistics. Unpaired t-test, Wilcoxon test, χ2 test, and Fisher exact test were used for inferential statistics where appropriate, with 95% confidence interval and a p < 0.05 considered statistically significant.
Stepwise multiple logistic regression analysis was used to determine the demographic and clinical parameters that were associated independently with SSIs. Subgroup analysis of each operation was performed for parameters that had statistically significant association with SSI by multiple logistic regression analysis. The level of significance was also set at 0.05 (two-tailed). R program was used for analysis with the epicalc [23] and rio [24] packages.
Results
A total of 10,139 procedures involving 9,661 patients were performed during the study period. Three hundred two procedures in 301 patients had post-operative SSI resulting in an SSI incidence of 2.98% (Table 1). The cumulative incidence of patients with SSIs was the highest in craniotomies (5.2% of procedures), followed by colonic surgeries (4.1%), cholecystectomies (2.7%), coronary artery bypass grafts (1.7%), cardiac surgeries (1.2%), and mastectomies (1%). The SIR exceeded 1.0 in craniotomies, colonic surgeries and cholecystectomies. The cumulative incidence of SSIs shows a decreasing trend from year 2012 and this trend persisted until 2016, as shown in Figure 1.
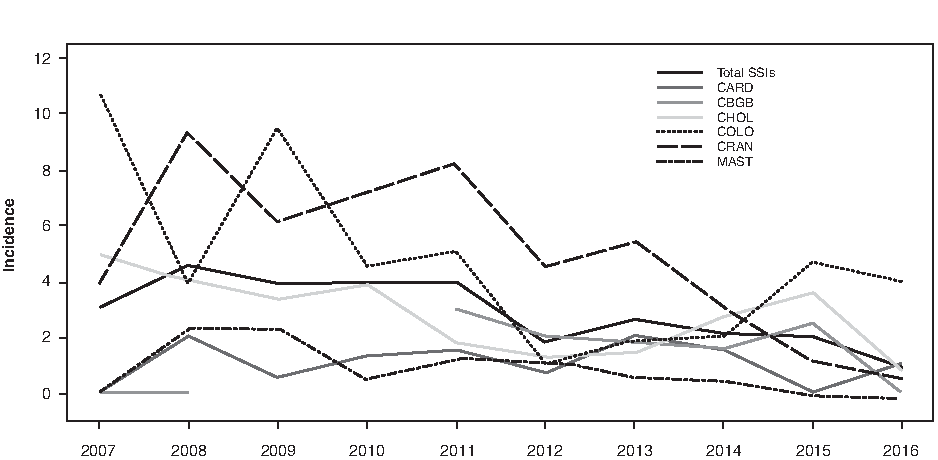
Annual incidence of surgical site infection from 2007–2016. CARD = cardiac surgery; CBGB = coronary artery bypass grafting-chest and donor site; COLO = colonic surgery; CRAN = craniotomy; MAST = mastectomy; CHOL = cholecystectomy.
Incidence and Standardized Infection Ratio of Surgical Site Infection in the Study (n = 10,139)
RI = National Nosocomial Infections Surveillance Risk index; SIR = standardized infection ratio; CARD = cardiac surgery; CBGB = coronary artery bypass grafting-chest and donor site; COLO = colonic surgery; CRAN = craniotomy; MAST = mastectomy; CHOL = cholecystectomy.
Analyzing for factors associated with SSIs
With case to control matching, 1,204 procedures were selected randomly for the analysis; there were 301 procedures for the SSI group and 903 procedures for the control group. Demographic characteristics were well balanced between the groups (Table 2). The SSI group and the control group had median age of 54 and 53 years, respectively. Male gender was nearly equal (51% in the SSI group and 49% in the controls). American Society of Anesthesiologists physical status was not statistically significantly different between the groups. Medians of BMI and obesity were not statistically significantly different between the groups. Only 13.2% of the patients had smoking habit, which was not different between groups. National Nosocomial Infection Surveillance scores and the presence of diabetes mellitus were the only two parameters that had statistically significantly differences between the groups. More than one-third of the patients with diabetes mellitus had post-operative SSI whereas only 23.5% of the patients without diabetes mellitus experienced post-operative SSI. Surgical procedure, type of surgery, prolonged operative time, and pre-operative antibiotic prescription were also not associated with SSIs.
Patient Demographic Data
Statistically significant with p < 0.05. *p < 0.05.
Rank sum test.
χ2 test.
SSI = surgical site infection; IQR = interquartile range; ASA = American Society of Anesthesiologists; DM = diabetic mellitus; BMI = body mass index; NNIS = National Nosocomial Infections Surveillance; CBGB = coronary artery bypass grafting-chest and donor site.
Consequences of SSIs
The consequences of SSIs are shown in Table 3. In our study, the SSI cases had more than three times the mortality rate of non-SSI cases (7% compared with 1.9%, p < 0.001). When types of surgery were considered, the differences in mortality were statistically significant only in cranial and colorectal procedures. The overall difference in median of hospital charges per admission was approximately $1,600 higher in the SSI group ($5,509.20 compared with $3887.90, p < 0.001). Significant differences were found in all operation types except for mastectomy. The median LOS was 11 days longer in the SSI group (24 days compared with 13 days, p < 0.001).
Consequences of Surgical Site Infections
Statistically significant with p < 0.05. *p < 0.05; **p < 0.01; ***p < 0.001.
SSI = surgical site infection; NA = not available; IQR = interquartile range; LOS = length of stay; SD = standard deviation; CBGB = coronary artery bypass grafting-chest and donor site.
Organisms and drug resistance
Two hundred five specimens for organism culture were collected from 152 SSI events (Table 4). The most common type of organisms were gram-negative bacteria (44.9%), and almost half were drug-resistant organisms (49.3%), although few were multi-drug resistant. Enterococcus spp. was the most common gram-positive organism (14.6%), followed by Staphylococcus aureus (10.7%), and coagulase-negative staphylococci (7.3). For gram-negative organisms, Escherichia coli was the most common (19.0%), followed by Klebsiella spp. (11.7%), Acinetobacter baumanii (7.3%), Enterobacter spp. (3.9%), and Pseudomonas aeruginosa (2.9%). Vancomycin-resistant enterococci (VRE) was not found in this study, whereas methicillin-resistant Staphylococcus aureus (MRSA) was reported in five cultures (22.7%). Approximately 80% of Escherichia coli were resistant to extended-spectrum cephalosporins and fluoroquinolones. Slightly more than half of Klebsiella spp. were resistant to extended-spectrum cephalosporins (54.2%) but not resistant to carbapenems group. Most Acinetobacter baumannii were resistant to carbapenems group (60%) and two were resistant to sulperazone, one resistant to tigecycline, and none were resistant to colistin. Half of the Enterobacter spp. were resistant to extended-spectrum cephalosporins. One-third of Pseudomonas aeruginosa were resistant to carbapenems group and cephalosporins, and none resistant to piperacillin or piperacillin-tazobactam. On multivariable logistic regression analysis, diabetes mellitus was the only important risk factor for post-operative SSI (OR 1.79; 95% CI 1.17–2.73, p = 0.008; Table 5).
Organisms and Drug Resistance
SSI = surgical site infection; VAN = vancomycin; OX/METH = oxacillin/methicillin; AMP = ampicillin; ESC4 = extended- spectrum (ES) cephalosporins (cefepime, cefotaxime, ceftazidime, ceftriaxone); FQ3 = fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin; SULP = sulperazone; COLIS = colistin; TIGE = tigecycline; AMINOS: aminoglycosides (amikacin, gentamicin, tobramycin); ESC2 = ES cephalosporins (cefepime, ceftazidime); Carbapenems are imipenem and meropenem; NA = not available.
Multivariable Regression Analysis
Discussion
Surgical site infection is one of the most frequently reported and preventable hospital-acquired infections. This 10-year retrospective study found an overall SSI rate of 2.98%. Among the 6 selected operations, craniotomy (5.18%), colon surgery (4.09%), and cholecystectomy (2.65%) were associated with the highest incidence rates of SSIs. Patients with an SSI have a higher mortality rate compared with non-SSI patients, longer hospital stays, and higher in-hospital expenditures. Approximately half of the organisms identified in this study were drug-resistant organisms, including some with multi-drug resistance. Diabetes mellitus was the only independent risk factor for post-operative SSIs in the multivariable regression analysis model in our study and remained the only substantial risk factor after subgroup analysis.
The rate of SSI in this study was low compared with other studies done in low- to middle-income countries (6.1%) [25,26] and Southeast Asia (7.8%) [27]. Compared with developed countries, however, the observed incidence rate of SSI (2.98%) was relatively high. For example, a study from the U.S. National Healthcare Safety Network between 2006 and 2008 reported an overall SSI rate of 1.9%. This difference could be attributed to higher standards of care in developed countries and a result of effective surveillance program.
In this study, the cumulative incidence was lower after 2012 and became comparable to developed countries (1%–2.7%). The reason that the cumulative incidence of SSIs began to decrease in our study might be because of the initiation of an SSI prevention program. This program was based on prescribing appropriate pre-operative antibiotic agents, pre-operative skin shaving method, pre-operative blood sugar control (target <200 mg%), hand washing before and after wound dressing, and prevention of peri-operative hypothermia (maintain body temperature >35.5°C). After this program was initiated, the percentage of hand washing before and after wound dressing increased to more than 80% in every quarter. Moreover, no new cases of MRSA SSIs were reported after the year 2010, which could be the best result of good hand hygiene. In this study, the operations in which the SIR exceeded 1.0 were craniotomy, colon surgery, and cholecystectomy, and we note that many reports from developed countries in Europe and Asia report similar incidences of SSI among these operations [7,28–30].
The present study showed a higher incidence of SSI with increasing NNIS risk index score and presence of diabetes mellitus as an underlying disease, but no such associations with gender, age, ASA physical status, tobacco use, BMI, wound class, use of pre-operative antibiotic agent, prolonged operative time, or emergency surgery. On multivariable logistic regression analysis, diabetes mellitus was the only important risk factor for post-operative SSI. This finding on the risk factors of SSI differed from a recent report by the World Health Organization, in which not only diabetes mellitus, but high BMI, high NNIS risk index score, severe wound class, prolonged surgical duration, ASA physical score of at least three, and pre-operative antibiotic use were also associated with SSI. A systematic review by Korol et al. [14] also found that comorbidities, advanced age, risk indices, patient frailty, surgery complexities, longer surgery, and diabetes mellitus were risk factors for SSI. In our study, these parameters were associated with higher rates of SSI but without statistical significance. This might be explained by differences in surgical practice among institutes. Although consistent with other studies, our data showed that SSIs increased hospital expenditures, length of hospital stay, and in-hospital mortality.
The most commonly detected organisms were Escherichia coli (19.0%) followed by Enterococcus spp. (14.6%), Klebsiella spp. (11.7%), and Staphylococcus aureus (10.7%). Although these findings differ from an NHSN study in which Staphylococcus aureus was the predominate organism [30], our findings are similar to those reported in a study from Southeast Asia [27]. Although half of our SSIs were drug resistant, the antimicrobial multi-drug–resistant micro-organism problem remained in a small fraction in this study, possibly because of the control of antibiotic usage in our institute. In addition, the incidences of MRSA and VRE in our study were lower compared with the NHSN study although the frequency of carbapenem-resistant Enterobacteriaceae (CRE) was higher [30]. Another factor that may be related to the high incidence of drug-resistant organisms in Thailand is the national policy of antibiotic agent distribution. Although nationwide campaigns such as the Antibiotic Smart Use program have been introduced to promote rational drug use, a recent report from the World Health Organization found that most antibiotic agents in Thailand can be easily accessed from retail pharmacies without prescription or monitoring system [31].
The overall prevalence of diabetes mellitus in this study was 12.36% and was substantially higher in the SSI group. Also, on multivariable analysis, diabetes was the only important factor for SSIs. A systematic review and meta-analysis in 2015 that included 94 studies comprising a total of 866,427 procedures and 32,067 SSIs also reported substantial association between diabetes and SSI (OR = 1.53; 95% CI 1.11–2.12; I2, 57.2%) [32].
The strength of this study was its high control to case ratio (3:1), which provided a power of 80% (α = 0.05, β = 0.2). Moreover, surgical procedure matching between cases and controls was performed because of differences in risk of SSIs and risk factors in individual operations. The completeness of the matching design was well reflected by the non-statistically significant differences in baseline characteristics between the two groups. However, there were also three notable limitations. First, this study only included selected operations based on the six procedures with the highest risk indexes from the registry of the infection control unit. The true overall incidence of SSIs in all procedures in our center certainly lower than this study would indicate, considering the exclusion of low risk operations. Second, the nature of the study design that used random sampling of cases and controls might have compromised the power of the study by limiting the number of subjects analyzed. Finally, although the modified NNIS risk index has been updated in favor of a laparoscopic procedures, this study used the standard NNIS because the analysis used a registry in which data regarding laparoscopic surgery were not separately collected.
Overall, the SSI rates for our study were comparable with other studies. The overall trend of SSIs was decreasing following 2012, although some procedures still had a high incidence. Efforts to further reduce SSIs should focus on those procedures, especially in patients with diabetes.
Footnotes
Acknowledgments
Dave Patterson from the International Affairs Unit, Faculty of Medicine, Prince of Songkla University, reviewed the English in the manuscript.
Author Disclosure Statement
No competing financial interests exist.