
Abstract
Abstract
Background:
Implant-related infections in hand surgery are dreaded complications, potentially leading to loss of finger joint function or amputation. Knowledge about the clinical presentation and treatment concepts of these infections is limited. The aim of this study is to present a consecutive series of patients with implant-related infections of the finger joints and wrist.
Patients and Methods:
We identified 25 patients with 29 implant-related infections. Infections were categorized as osteosynthesis-related infections (ORIs) or arthroplasty-related infections (ARIs). Further categorization included early and late post-operative (four weeks or less or more than four weeks after implantation) and exogenous and hematogenous infection.
Results:
Compared with patients with ARIs (n = 11), those with ORIs (n = 14) were predominantly male (n = 11), were younger (mean 43 vs. 65 years, p = 0.0023), had few or no comorbidities, and had an exogenous source of infection. Patients with ARIs were predominantly female with rheumatoid arthritis (n = 8) and had a hematogenous pathogenesis. Infections occurred late in 22 (88%) patients. The most commonly isolated micro-organism was Staphylococcus aureus (n = 12; 48%). All ORIs were treated with implant removal and a median antimicrobial treatment duration of 39 days (interquartile range [IQR] 28–50 days). In the ARI group, the implant was removed in three patients and exchanged in three patients (one-stage exchange in one patient, two-stage exchange in two patients). In five individuals, debridement and implant retention was performed. The median antimicrobial treatment duration for ARIs was 42 days (IQR 30–75 days). The median follow-up time was 96 days (IQR 42–258 days) and infection was cured or presumably cured in 22 patients (88%).
Conclusion:
Our series shows distinct host and clinical patterns in ORIs and ARIs, supporting this categorization. The infection prognosis in ORIs is excellent with implant removal and antimicrobial treatment. Treatment concepts in ARIs are often derived from algorithms for periprosthetic joint infections of larger joints and need to be further elucidated.
A
Patients and Methods
The Department of Plastic and Hand Surgery, Bern University Hospital, Bern, Switzerland, is a tertiary and referral center for hand surgery. In 2016, the institution provided specialized care for 12,538 patients in the outpatient clinic and surgical interventions for 1,787patients. Also, from 2005–2016, 182 arthroplasties were implanted at our institution.
For this study, adult patients (i.e., 18 years or older) with implant-related infections were identified from two datasets. From the first dataset, we collected all implant-related infections of finger joints and of the hands that were treated in our institution from 2005 to 2013 [6]. The second dataset consisted of infection episodes that were collected prospectively from 2014 to 2016. In every episode, data were obtained according to predefined variables [2,6]. The definition of infection was applied as described previously [2]. In brief, intra-operative pus surrounding the joint, or growth of micro-organisms, was required in at least one sample (or two samples with a micro-organism that belonged to skin flora) or histopathologic findings consistent with implant-related infections was required. Every infection episode was categorized in osteosynthesis-related infections (ORI) or arthroplasty-related infections (ARI), based on the type of the implant infected. The interval from device implantation to onset of symptoms was used to categorize infection in early postoperative (four weeks or less) or late (more than four 4 weeks) infections [7]. Based on the patient's history, age of the implant, duration of symptoms, and causative micro-organism, we categorized the pathogenesis of each infection episode as exogenous or hematogenous [7]. These definitions were extrapolated from those used for the categorization of periprosthetic joint infections (PJIs) [8]. Medical charts were reviewed for the site of infection, patient characteristics, and variables associated with medical and surgical treatment. The latest available follow-up examination was used for outcome assessment, which included infection resolution, restoration of joint mobility and stable bone. For resolution of infection the following criteria were required: no symptoms or clinical signs for local or systemic infection and a healed wound at the site of previous infection. Cure of infection was defined as an infection-free follow-up period of one year or more. If the period was less than one year, the outcome was defined as presumably cured.
GraphPad Prism 5.0 (GraphPad Prism Software, San Diego, CA) was used for statistical analysis. Differences in group proportions were assessed by contingency tables and the χ2 test or by Fisher exact probability test if frequency was less than five. Non-parametric t-test used nominal data. A two-tailed p value of ≤0.05 was considered significant. The local ethical committee and the Department of Research of the University Hospital of Bern, Switzerland, approved the study (Cantonal Ethical Committee Bern: 2016-01756).
Results
Patient characteristics
We identified 25 patients with 29 implant-related infections, consisting of 14 patients with ORIs and 11 with ARIs (Table 1). Patients with ORIs were predominantly male and younger and had few or no comorbidities. Infection manifestation was less than four weeks after implantation of the device in the majority of cases (88%). In the ORI episodes, the postulated pathogenesis was infection mainly from an exogenous source (i.e., typically in the peri- or post-operative period), whereas hematogenous seeding to the implant was the postulated pathogenesis in the majority of ARI episodes. This difference was significant (p = 0.0072) and consistent with the observation that ARIs occurred later than ORIs did.
Other comorbidities included arterial hypertension, congestive heart failure, chronic renal failure, solid cancer, hematologic cancer, psychiatric disorder, and intravenous drug abuse.
The interval from device implantation to onset of symptoms was used to categorize infection as early (≤4 weeks) or late (>4 weeks) postoperative.
On the basis of the patient's history, onset of infection manifestation, and causative microorganism, the pathogenesis of the infection was categorized as exogenous or hematogenous.
ORI = osteosynthesis-related infection; ARI = arthroplasty-related infection; CPPD = calcium pyrophosphate dehydrate crystal deposition disease; SD = standard deviation; IQR = interquartile range.
Devices and infection sites
Twenty-nine infection sites were identified. The devices used in the ORI group (n = 17) included Kirschner wires and screws in 13 patients and plates in one patient. The devices in the ARI group (n = 12) included silicone finger joint implants in six patients, total wrist arthroplasty in four patients, and ulnar head arthroplasty in one patient. One patient had a finger joint implant, as well as radiocarpal arthroplasty (i.e., 12 implants in 11 patients). In eight of 11 patients, the arthroplasty was implanted in our institution. The distribution of infection sites is shown in Figure 1. In 10 of 11 patients with ARI, the right hand was involved. In contrast, among the 14 patients in the ORI group, the distribution was almost even (right hand in 8, left hand in 7 patients). In this group, the third and fourth digits (5 of each; 32%) were affected most commonly, as was the distal inter-phalangeal joint (n = 12 of 17 joints; 71%).
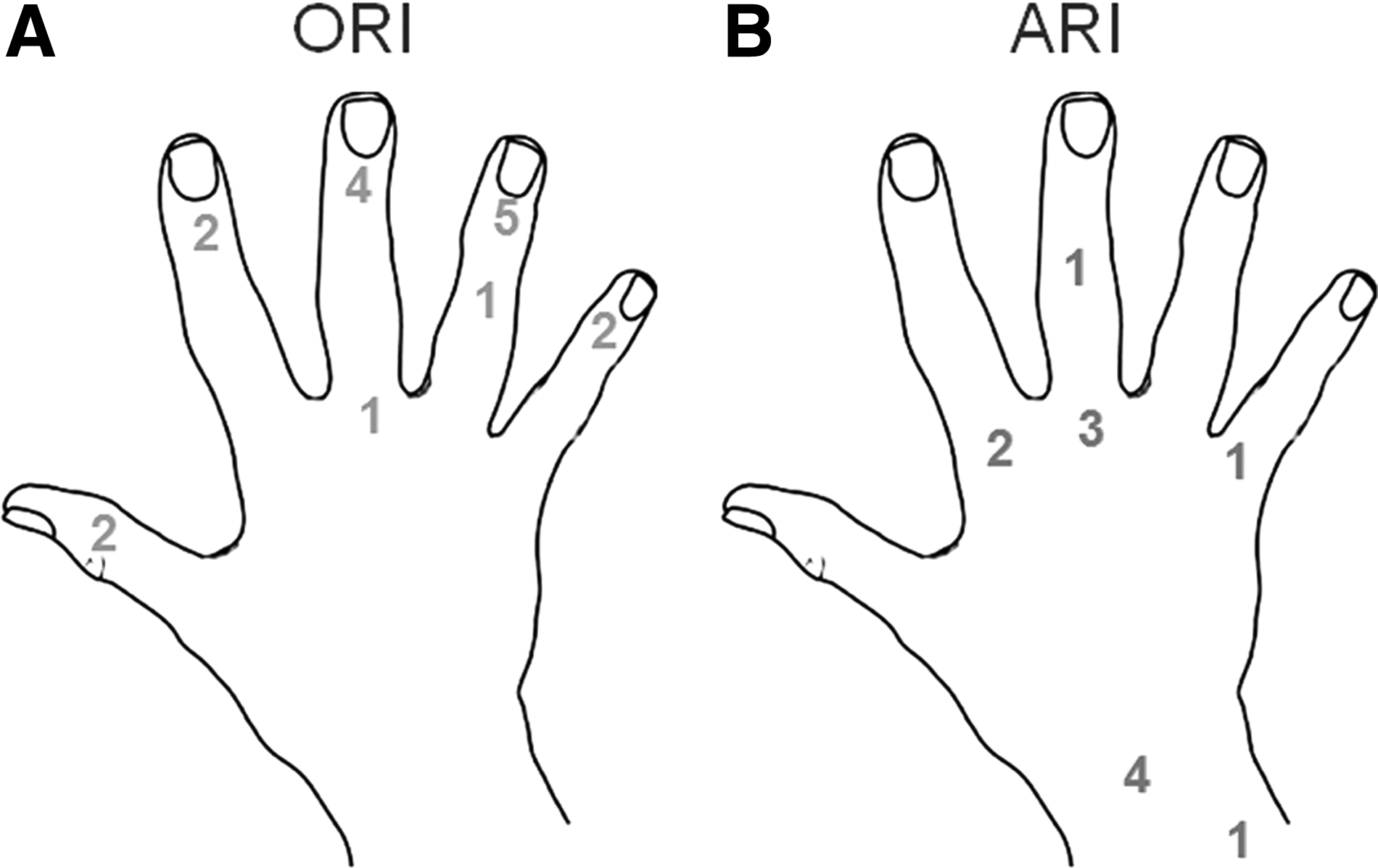
Distribution of 17 osteosynthesis-related infections (ORIs) in 14 patients (
Microbiology
The results of the microbiologic investigations are displayed in Table 2. An organism was isolated in 23 of 25 patients (92%), despite administration of antibiotic agents pre-operatively in 14 (56%). Staphylococcus aureus was the species found most commonly (12 patients; 48%) followed by Streptococcus spp. (5 patients; 20%). In two patients, polymicrobial infection was evident. There was no significant difference in the distribution of micro-organisms between ARIs and ORIs.
Streptococcus spp. included β-hemolytic streptococci and Streptococcus milleri group. bStaphylococcus lugdunensis belongs to the group of coagulase-negative staphylococci. Because of its potential virulence, it is presented separately.
The sum of the numbers exceeds 25 (100%) because of polymicrobial infections (i.e., two organisms in one patient and four organisms in another).
Surgical and antimicrobial therapy
In all patients with ORIs, the foreign body was removed and the joint stabilized without implanting a device at a later stage. In nine of 14 patients (64%), a single intervention was performed, in three patients two interventions, and in two patients three interventions. Two patients in the ORI group required a flap for soft-tissue coverage. The median post-operative antimicrobial treatment duration was 39 days (interquartile range [IQR] 28–50 days).
In three of 11 patients with ARI (27%), the implant was removed permanently. In two patients (18%), a two-stage exchange was performed. The device was re-implanted after 44 days (metacarpophalangeal [MCP] joint silicone arthroplasty) or after 74 days (ulnar prosthesis). In one patient with two devices (finger joint implant and radiocarpal arthroplasty), a one-stage exchange of the MCP joint was performed, and the infection in the radiocarpal arthroplasty was suppressed without debridement. In the other five patients, each with one device, debridement and implant retention was performed. One surgical intervention was conducted in eight of 11 patients, and two were conducted in three patients. The detailed history of the eight patients with implant retention or implant exchange in the ARI group is presented in Table 3 and 4. The median duration of post-operative antibiotic treatment in 10 patients in the ARI group was 42 days (IQR 30–75 days). One patient was treated with antibiotic suppressive therapy.
Patient with intravenous drug abuse.
Patient with Staphylococcus aureus colonization. In the scar area, there was a suture granuloma with a sinus tract to the site of infection.
Hematogenous seeding from an infected Port-a-Cath infection with CoNS. Duration of symptoms approximately 3 months.
CPPD = calcium pyrophosphate dihydrate crystal deposition disease; PIP = proximal interphalangeal; DIG = digitus; MCP = metacarpophalangeal; CoNS = coagulase-negative staphylococci.
Number of surgical interventions after first infection diagnosis.
Second intervention because of complication or reimplantation of arthroplasty.
Last follow-up examination at day 42. Patient died after 69 d because of congestive heart failure.
Patient died 14 d after surgery and during hospitalization because of an advanced solid cancer.
DAIR = debridement and implant retention; IV = intravenous; PO = per os; MCP = metacarpophalangeal; RC-A = radiocarpal arthroplasty; 1-St-E = 1-stage exchange; 2-St-E = 2-stage exchange.
Follow-up and outcome
The median follow-up time for all patients was 96 days (IQR 42–258 days). In the ORI group, cure of infection or presumable cure of infection was assessed in all patients. Five patients (36%) in the ORI group developed functional complication. One patient developed complex regional pain syndrome and adhesion of the extensor tendon requiring tenolysis surgery. Three patients developed post-infectious arthrosis, and arthrodesis was performed in one of them. One patient developed a painless non-union of the distal phalanx.
In the ARI group, a complication was noted in only one patient (Table 4), who developed an unstable joint for which second-stage arthrodesis was performed. In the ARI group, two (8%) patients died in the follow-up period, at 14 days and 69 days after surgery, from non-infectious causes. Both patients were receiving antibiotic treatment, and there were no clinical signs of uncontrolled infection at the last follow-up investigation on days 14 and 42. In one patient with two devices, the MCP implant failed 8 months after one-stage exchange and was removed. Suppressive (lifelong) therapy for the infection at the site of the radioulnar arthroplasty was recommended. Overall, cure of infection or presumable cure of infection was achieved in 22 patients (88%).
Discussion
Treatment concepts for infections in hand surgery are not established, often being derived in analogy to treatment concepts for orthopedic surgery (e.g., osteomyelitis of the hand) [9]. Recently, we analyzed 101 infections in native joints of the fingers and the wrist and found considerable differences from the clinical patterns reported for larger joints [2].
In the present study, we analyzed implant-related infections of the finger joints and the hand. We divided these infections into two categories (i.e., ORIs and ARIs) because they reflect different hosts and different clinical patterns. ORIs were comparable to those described for native small joint arthritis. Trauma was a frequent reason for implanting a device, patients typically being younger in the ORI group than in the ARI group and with a male predominance (Table 1). Both hands were almost equally affected in the ORI group. In contrast, the vast majority of patients with ARIs were females with rheumatoid arthritis with a higher median age than that in the ORI group. In comparison to PJI of hip- or knee arthroplasties, the incidence of infection in finger- and hand-joint arthroplasties is difficult to assess because different types of implants (e.g., silicone) at different locations of the hand are implanted. Over the 12-year observation period, the incidence proportion of ARIs was 0.36%. The right hand was predominantly affected in the ARI group (91% right hand, 9% left hand). We have no explanation for this finding, because the distribution of primarily implanted arthroplasties was not as uneven as the distribution of ARIs (56% right hand, 44% left hand). Interestingly, infections in the ARI group occurred significantly more often after hematogenous seeding to the implant than they did in the ORI group. This clinical pattern is not typical for arthroplasty infection in larger joints, where the infection frequently occurs in the peri- or post-operative period from an exogenous source (e.g., skin flora) [10]. One possible reason for this observation may be the high proportion of patients with rheumatic arthritis in the ARI group. Patients with this underlying disease are at risk for Staphylococcus aureus bacteremia with hematogenous seeding to bone and joint sites, in particular in the presence of an implant [11,12]. Although coagulase-negative staphylococci (CoNS) play a considerable role in exogenous PJIs of the larger joint, this was not the case in our series. In the ORI group, late infection was noted in 11 patients (79%) and an exogenous source in 13 (93%; Table 1). However, in only one patient with polymicrobial infection was CoNS isolated. In three patients, Staphylococcus lugdunensis was isolated. This micro-organism formerly belonged to CoNS but is often presented separately in infection studies because of its virulence properties [13].
Patients with ORIs had an excellent prognosis, similar to that observed in native joints [2]. Removal of the device and two or fewer debridements, followed by antimicrobial treatment, led to infection cure in 12 of 14 patients (86%); only two patients required a third surgical intervention. Although five patients (36%) developed complications in the follow-up investigations, two (14%) required surgical intervention for functional reasons. The median duration of post-operative antibiotics in that group was 5.5 weeks. In retrospect, on the basis of our previous experience with native small joint arthritis, a shorter duration of treatment after removal of the implant appears possible.
Treatment algorithms for implant retention have been published for PJIs of the hip and knee [7,14]. However, treatment concepts for hip and knee arthroplasty cannot be extrapolated uncritically to other joints, as has also been shown for infections of ankle joints [15]. In hand surgery, the implant-free interval in a two-stage procedure should be kept short because of the risk of joint contraction and spontaneous joint fusion after implant removal. Unlike the large joints, no cement spacer is used in the small joints. All patients but one with a short duration of symptoms were treated with debridement and implant retention, whereas those with a longer duration of symptoms were treated with a two-stage exchange. The success of this concept needs to be elucidated in a larger population of patients with ARIs.
The limitations of our study are its retrospective nature, with the inclusion of patients until 2013, and the use of medical records for data collection. In addition, the absolute number of patients and types of infected devices were both small, making comparisons and statistical analyses difficult. Nonetheless, to the best of our knowledge, this is the largest case series on implant-related infections of the hand and finger joints. The follow-up examinations were at less than one year in a considerable number of patients. Thus, our outcome results for cured and presumably cured may be overestimated. However, we expected patients with failures to have been referred to our center.
Our analyses support the concept of differentiating ORIs from ARIs in implant-related infections of hand surgery. Patients with ORIs have similar host and clinical patterns as in patients with pyogenic native small joint arthritis [2]. The outcome after debridement and removal of the foreign body followed by antimicrobial treatment was good in nearly all patients with ORIs. In 11 patients with ARIs, the predominant pattern was females with rheumatoid arthritis, late infection manifestations, and a hematogenous pathogenesis. In this study, treatment concepts were performed in analogy to those for larger joints. However, such concepts need to be validated and elucidated in a larger number of patients.
Footnotes
Acknowledgment
This study was presented in part at the 51st Annual Congress of the Swiss Society of Hand Surgeons in Thun, Switzerland (November 16–17, 2017), and at the 23rd FESSH congress, Copenhagen, Denmark (June 14–16, 2018).
Author Disclosure Statement
No competing financial interests exist.