
Abstract
Background:
Although the survival advantage of bilateral internal thoracic artery grafting (BITA) is well known in patients undergoing coronary artery bypass grafting (CABG), this technique has not been widely adopted. This is mainly because of the increased risk of deep sternal wound infections (DSWI) associated with its use. However, in recent years the overall risk of DSWI has decreased. This is mainly because of strategies that have been adopted to decrease the risk of these infections in patients undergoing CABG.
Conclusion:
In this review we identified DSWI preventive strategies and described them in detail so that their use by surgeons can be increased. This would minimize the risk of DSWI after BITA grafting and maximize the use of this highly effective surgical technique.
The survival advantage of bilateral internal thoracic artery grafting (BITA) over single internal thoracic artery grafting (SITA) is well known in patients undergoing coronary surgery [1–12]. Bilateral internal thoracic artery grafting is associated with better long-term survival even in high-risk patients such as those with diabetes mellitus [13,14] and the elderly [15]. Despite this, BITA grafting was performed in only 4.1% of the patients undergoing coronary surgery from 2000–2009 in the United States [16]. Although increased complexity of operation and increased operating time and need of resources represent some of the factors responsible for decreased adoption of BITA grafting, the most important factor remains to be the higher occurrence of deep sternal wound infections (DSWI) associated with BITA use. Surgeons are incentivized for short-term outcomes and not long-term outcomes, and with the use of BITA grafting, surgeons pay a high immediate price for DSWI and patients receive an invisible long-term survival benefit for which the surgeon receives no credit [13]. Also, surgeons are not reimbursed for the cost of treating DSWI because it has been designated by the Centers for Medicaid and Medicaid Services (CMS) as a never event—an event that is completely preventable [13,15]. Therefore, DSWI is really the Achilles' heel of BITA grafting, limiting its well-deserved widespread adoption. The purpose of this review is to identify the risk factors for DSWI and the strategies through which the occurrence of DSWI can be minimized so that the use of BITA grafts in patients undergoing CABG can be maximized.
Declining Incidence of Deep Sternal Wound Infections
The incidence of DSWI in patients undergoing CABG has ranged from 0.23% to 3.2%, over the last 30 years [14,17]. However, the overall occurrence of post-CABG DSWI is declining because of better patient selection and improved surgical techniques such as skeletonized internal thoracic artery (ITA) harvest. Alasmari et al. [18] studied the temporal trends of surgical site infections in patients undergoing CABG; their 16-year study period ranging from 1993 to 2008 revealed decreasing trend in incidence of DSWI with incidence of only 0.4% during 2005–2008. Data from the Society of Thoracic Surgeons (STS) National Adult Cardiac Surgery Database reported an overall DSWI incidence of 0.3% for isolated CABG in 2007. This decreased further to 0.2% in the most recent 2014 report [19].
Risk Factors for Deep Sternal Wound Infections
A number of risk factors for DSWI have been identified in the literature. These include advanced age, diabetes mellitus, obesity, New York Heart Association (NYHA) classification ≥3, chronic obstructive pulmonary disease (COPD), active smoking, renal failure, pre-operative nasal carriage of Staphylococcus aureus, pre-operative hyperglycemia, intra-aortic balloon pump (IABP) use, BITA grafting, increasing number of blood transfusions, re-exploration for bleeding, increased duration of mechanical ventilation, and prolonged intensive care unit (ICU) stay [17,20]. Simek et al. [14] analyzed the risk factors of DSWI from 17 studies and identified diabetes mellitus and obesity as the common factors. Some of the important risk factors are discussed below.
Gender
Gender may play a role in development of DSWI after CABG. Interestingly, both male and female gender have been identified as risk factors for DSWI in the literature [14]. Borger at al. [21] identified male gender as an independent risk factor for development of DWSI (odds ratio [OR] = 1.8; 95% confidence interval [CI] = 0.9–3.7). The Parisian Mediastinitis Study group also showed male gender as a risk factor for DWSI after cardiac surgery (OR = 2.55; 95% CI = 1.12–5.82) [22]. However, Raza et al. [23] and Kieser et al. [24] in their studies found female gender to be associated with higher risk of DSWI. In the study by Raza et al. [23] female gender was associated with an 80% increased risk in developing DSWI (OR = 1.80; 68% CI = 1.64–1.99; Fig. 1). Identification of both male and female genders as risk factors for DSWI in the literature could be because of some interaction that exists between gender and other risk factors such as obesity or diabetes mellitus, therefore, further research is needed to clarify this.
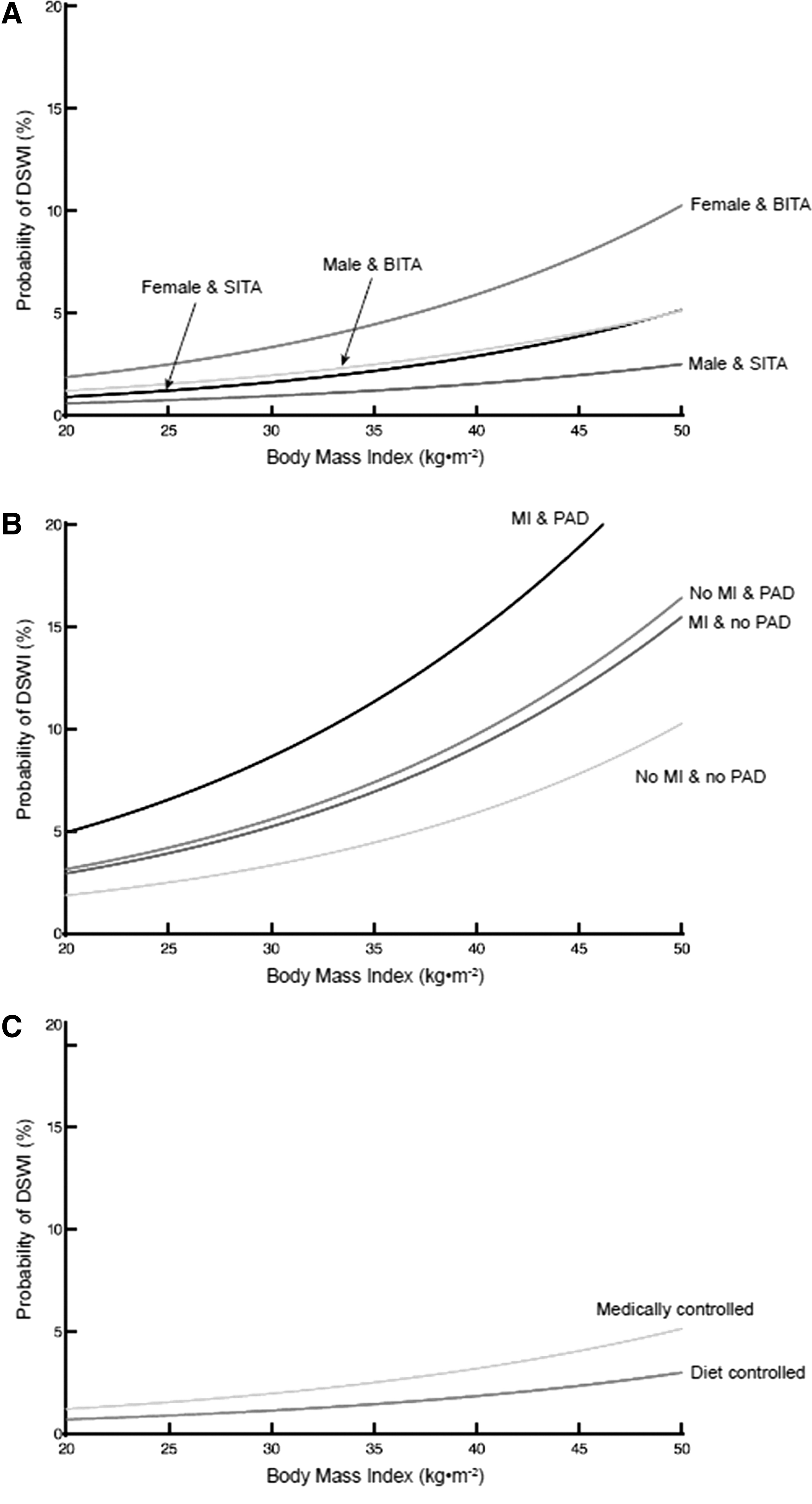
Effect of risk factors on probability of deep sternal wound infection (DSWI) across a range of body mass indexes. Simulations were based on the logistic regression model for a patient undergoing coronary artery bypass grafting (CABG) with cardiopulmonary bypass, in the past decade, with complete revascularization. Other factors are listed for the individual depictions. (
Diabetes mellitus
Diabetes mellitus is one of the strongest predictors of DSWI in patients undergoing CABG (OR = 2.6; 95% CI = 1.7–4.0) [21]. This is because hyperglycemia impedes the normal physiologic response to infection [25,26]. Also, the non-enzymatic glycosylation (NEG) of various proteins involved in wound healing impairs the healing process [25]. Non-enzymatic glycosylation also increases collagenase activity and decreases wound collagen content [26]. Moreover, affected leukocyte function also increases the risk of infection [25]. Even short-term hyperglycemia increases glycosylation which impairs complement fixation further impairing response to the infection [27]. Raza et al. [23] showed that pharmacologically treated diabetes mellitus compared with diet-controlled diabetes mellitus was associated with 73% increase in risk of DSWI (Fig. 1).
Obesity
Obesity is another major risk factor for developing DSWI after CABG [17]. Raza et al. [23] found that for per-unit increase in BMI, the risk of DSWI increases by 7% (OR = 1.80; 68% CI = 1.64–1.99). Obesity increases risk of infections because capillary density in obese patients does not increase in proportion to the increase in adipose tissue resulting in vascular insufficiency. This causes relative hypoxia that likely leads to higher rates of wound infections in obese individuals. Additionally, macronutrient and micronutrient deficiency in obese individuals and abnormal population of immune mediators contribute to the lengthening of inflammatory stage during wound healing. These factors increase risk of surgical site infections in obese individuals [28].
Diffuse atherosclerotic burden
Factors representing diffuse atherosclerotic burden such as peripheral arterial disease (PAD), carotid disease, and history of stroke and myocardial infarction (MI) may also increase the risk of DSWI. Raza et al. [23] found that PAD and history of MI were associated with 58% (OR = 1.58; 68% CI = 1.39–1.80; Fig. 1) and 73% higher risk (OR = 1.73; 68% CI = 1.49–2.01) of developing DSWIs, respectively.
Bilateral internal thoracic artery grafting
Bilateral internal thoracic artery grafting is one of the strongest predictors of developing DSWI after CABG [22,24]. The ITA provides majority of blood supply to the sternum and when harvested for CABG the corresponding sternal half is substantially devascularized [29]. Removal of both ITA therefore devascularizes the entire sternum leading to wound complications and DSWI.
Strategies to Prevent Occurrence of Deep Sternal Wound Infections
Pre-operative techniques
Pre-surgical cleaning with clippers
Surgical site infections in general can be reduced by careful pre-operative preparation. This also holds true for DSWI in patients undergoing CABG. Use of clippers versus razors for pre-operative hair removal has been shown to reduce the incidence of DSWI [30–32]. Ko et al. [31] compared manual shaving with electrical clipping for hair removal in patients undergoing CABG and found a substantially higher rate of suppurative mediastinitis in manually shaved patients (OR = 3.25; 95% CI = 1.11–9.32; p = 0.024).
Bathing with chlorhexidine scrub
Pre-operative bathing with chlorhexidine might aid in reducing counts of normal skin flora colonizing sternal wounds rather than preventing surgical site contamination. In this regard various authors have provided research-based evidence to create an understanding of pathogens contaminating sternal wounds despite use of antiseptic solutions. In a systematic analysis by Kuhme et al. [33] organisms such as coagulase-negative staphylococci and Propionibacterium were frequently isolated from the skin and subcutaneous tissue of cardiac surgical sites of patients who were washed with a pre-operative chlorhexidine scrub. However, although skin preparation with chlorhexidine cannot prevent skin flora organisms from contaminating the incision and surrounding tissue during surgery, it can reduce the bacterial counts [34].
Screening for nasal carriers and use of mupirocin for positive carriers
Lazar and colleagues [34] recommended screening of Staphylococcus strains via nasal swabs or polymerase chain reaction (PCR) testing in all cardiac patients prior to surgery as an effective technique to prevent sternal wound infections. Among the general population, 20%–30% test positive for Staphylococcus aureus [35]. Because strains of Staphylococcus are often cause wound infections after cardiac surgery, the likelihood of developing an infection post-operatively is three times more among patients who are carriers of the effective organism [34,36]. Moreover, carriers of methicillin-sensitive Staphylococcus aureus (MSSA) carries a high risk for developing methicillin-resistant Staphylococcus aureus (MRSA) among ICU dwelling patients [37].
Mupirocin has emerged as a preferred choice of treatment for nasal disinfection pre-operatively in Staphylococcus aureus-colonized patients. Results from studies concluded that among non-colonized patients the topical use of mupirocin had marginal effects [34]. Therefore, analysis from data is only suggestive for using mupirocin among patients whose swab cultures are not available at the time of surgery or who tested positive for staphylococcal colonization. However, it is reported that intra-nasal administration of mupirocin causes prompt decolonization among MSSA in more than 90% of positive cases but only 40%–50% of cases colonized with MRSA show effect [38–40].
Our practice is that we test the patient pre-operatively for Staphylococcus aureus and if a carrier, mupirocin ointment is used before surgery. If positive for MRSA, then intravenous vancomycin is given along with intravenous cefuroxime on anesthesia induction at surgery.
Malnourishment with low albumin status
Pre-operative hypoalbuminemia is another risk factor associated with high mortality and DSWI among patients undergoing cardiac surgery [41–43]. Patients with hypoalbuminemia, loss of body weight more than 10% within a six-month time frame, and muscle wasting are candidates for pre-operative nutritional support preferably through the enteral route [43,44]. In such patients, surgery should be delayed for 7 to 10 days if possible [44].
Smoking cessation
Smoking is a major risk factor involved in DSWI predisposition and is also associated with high mortality rates during cardiac surgery. Therefore, the data from previous studies recommend cessation of smoking at least one month prior to surgery [45–49]. In this regard, aggressive pulmonary hygiene is advised for active smokers and patients with COPD [34].
Weight reduction
Obesity is an established risk factor for DSWI [23,28]. Increased technical difficulty during surgery, failure to increase the antibiotic dose used in prophylaxis in an obese patient, nature of adipose tissue as a substrate for bacteria, difficulty with skin disinfection reaching the depths of skin creases, and the increased likelihood of comorbidities such as diabetes mellitus and vascular disease with obesity are possible reasons. Pre-operative weight reduction can reduce the incidence of DSWI in patients undergoing elective or non-urgent CABG. However, the degree of weight loss required to achieve reduction in DSWI rates still needs to be established [50].
Antibiotics and infection prevention
Peri-operative antibiotic agents administered within 60 minutes before incision and up to 48 hours post-operatively are used routinely in cardiac surgery [51]. Guidelines published by the Society of Thoracic Surgeons Workforce in 2006–2007 recommends using first-generation cephalosporin (cefazolin) or second-generation cephalosporin (cefuroxime) intravenously. However, the dose should be given in accordance with weight. Vancomycin is not a preferred option for prophylaxis of cardiac surgical procedures alone, instead its use is restricted in patients who are allergic to β-lactam antibiotics or where suspicion of MRSA is high and is usually administered within 60 to 120 minutes before surgery. For a broader gram-negative coverage, aminoglycosides are given with vancomycin but because of their combined toxicities, one dose peri-operatively and a second dose of ≤4 mg/kg is advised [52,53].
It is also recommended to recognize and treat remote extrathoracic infections in elective cardiac surgery patients to prevent DSWI. Delaying the procedure until resolution of remote infection is considered a safer option in such patients [45,46]
Intra-operative techniques
Skeletonization of ITA grafts: The way forward
The skeletonized approach of ITA harvest is one of the most important techniques that can be used to reduce the risk of DSWI in patients undergoing BITA grafting. Sternal blood supply is through the sternal and anterior intercostal branches of the ITA, which originate either directly or as a common trunk from the ITA. After removal of the ITA, if the sternal-anterior intercostal trunk remains intact substantial collateral blood flow to the sternum can be maintained [54]. Pedicled harvesting of ITA substantially reduces the vascular supply to the sternum whereas the skeletonized approach preserves it. In pedicled harvesting the ITA is isolated from the chest wall as a pedicle, together with the vein, fat, muscle, and fascia; electrocautery is also used, which damages the sternal blood supply [55]. However, in the skeletonized approach the ITA is gently isolated with the use of scissors and silver clips without the use of cautery, therefore, the common trunk is preserved [54] and damage to sternal blood supply is minimal resulting in preservation of collateral blood flow as well as the added advantage of having a longer graft [55]. Skeletonization of ITA has been shown to be associated with lower incidence of DSWI in a number of studies. Fouquet et al. [56] showed that skeletonized approach to BITA grafting not only reduces sternal complications but also reduces pulmonary complications and decreases post-operative pain. A large meta-analysis of studies comparing the skeletonized versus pedicled approach to BITA grafting found a lower rate of DSWI with the skeletonized approach [57].
The skeletonized approach has also reduced the incidence of DSWI after BITA grafting in patients with diabetes mellitus and studies suggest DSWI rates comparable to SITA when the skeletonized approach is used in patients with diabetes [58–62]. Tang et al. [20] found decreased rates of DWSI in patients with diabetes mellitus with skeletonized BITA grafts. In their study, the risk of DSWI in patients with diabetes mellitus with skeletonized BITA grafts was similar to that in patients without diabetes mellitus (1.3% vs. 1.6%, p = 0.8). A large meta-analysis of patients with diabetes mellitus undergoing CABG by Deo et al. [63] also revealed that skeletonized ITA harvesting with attention to preservation of sternal blood flow can minimize DSWI in patients with diabetes mellitus.
Modified surgical and sternal closure techniques
Some modified surgical and sternal closure techniques have also been shown to be associated with lower occurrence of DSWI. Sakic et al. [64] showed that skeletonization of BITA grafts along with augmented sternal wires is highly effective in preventing DSWIs. Friberg et al. [65] compared the use of extra sternal wires (seven or more) with standard technique (six or less) in terms of effect on DSWI rates and concluded that incidence of DSWI was reduced with use of additional fixation wires at lower sternum. Kamiya et al. [66] found a protective effect of extra sternal fixation wires (seven or more compared with six or less) against sternal infections and sternal instability in high-risk patients (patients with diabetes mellitus; diabetes mellitus and COPD; COPD and renal insufficiency; and diabetes mellitus and COPD plus renal insufficiency). In patients with diabetes mellitus, sternal closure with eight or more wires had an advantage over seven or more wires [66]. Also, Song et al. [67] found sternal closure with rigid plate fixation to be superior to standard wire closure, resulting in substantially reduced incidence of DSWI.
Avoiding BITA grafting in patients at the highest risk of developing DSWI
Patient selection has the potential to make a difference in reducing the incidence of DSWI. Avoiding BITA grafting in patients at high risk of developing DSWI could reduce the overall occurrence of DSWI in patients undergoing CABG. Obese females with diabetes mellitus with diffuse atherosclerotic burden represent the patient population at the highest risk of developing DSWI. Therefore, this is the patient population in which it may be best to avoid BITA grafting. Studies show that obese patients with diabetes have a 7.7-fold increase of risk of DSWI after BITA grafting than non-obese patients without diabetes [66]. The addition of female gender to this combination further increases the risk [23,24,58,69]. The study by Matsa et al. [69] showed that the combination of obesity, diabetes mellitus, and female gender was associated with a 10-fold increase in DSWI (15% vs 1.4% in patients with diabetes without this combination of risk factors).
Topical and intravenous antibiotic agents
Research data from various studies have shown a 16% reduction in sternal wound infections if additional dosing of intravenous cefazolin is given during surgeries exceeding four hours and in cardiopulmonary bypass procedures after two hours [70,71]. Implantable gentamycin-collagen sponges have also been widely recommended to prevent sternal wound infections after sternotomy and the results have been promising [72]. Kowalewski et al. [73] recently published results of their meta-analysis on the use implantable gentamicin-collagen sponges after heart surgery and concluded that this strategy substantially reduced the risk of sternal wound infections. Benefits of these methods for patients with diabetes mellitus who are at high baseline risk for DSWI have not been demonstrated clearly [74]. Kieser et al. [24] in their attempt to reduce the incidence of DSWI in patients with diabetes mellitus undergoing CABG evaluated several measures and showed that key measures were chlorhexidine-alcohol skin preparation and avoidance of BITA grafts in obese, female patients with diabetes mellitus, which dramatically reduced their rate of DSWI toward zero.
Bone wax complications
Bone wax is not ideal for prevention of DSWI and must be avoided among patients undergoing median sternotomy. Instead topical vancomycin can be applied on the cut edges of the sternum as a hemostatic agent that will simultaneously reduce incidence of DSWI. Being a foreign entity, bone wax prevents the union of bones and can result in wound dehiscence after sternotomy [75–77]. No definite data are available to support the use of bone wax in prevention and treatment of sternal wound infections.
Post-operative prevention
External chest support devices
External chest support devices in cardiac patients may aid in preventing DSWI, wound dehiscence, and hospital stay [34,78]. In this regard, various authors have argued the significance of using external chest support pads to limit the incidence of deep sternal wound complications post-sternotomy.
In two multicenter randomized controlled trials, Gorlitzer et al. [79,80] observed and discussed options such as post-sternotomy vests and elastic bandages and their efficacy in limiting sternal wound complications and re-procedures because of these complications after cardiac surgery. In one study they reported that during a 90-day follow-up period, the rates of re-procedures were much less for patients wearing post-sternotomy vests compared with patients wearing elastic bandage (0.6 vs. 3.9% p = 0.05). In their other research analysis that included 2,539 patients, they reported that only 1.04% of patients who developed sternal wound complications were a part of an external support chest group as opposed to an elastic bandage group in which 2.27% of patients were affected (p = 0.017).
Tewarie et al. [81] also emphasized the effectiveness of the sternum external fixation (Stern-E-Fix) corset in preventing DSWI post-sternotomy as opposed to the use of elastic bandages. Post-operatively, only one patient was reported to undergo a second operation because of sternal wound complication in a eight-week follow-up. However, with similar sternal closure technique and antibiotic regimen, 22 patients in the elastic bandage group required a re-operation. Moreover, a notable reduction in hospital stay was observed among patients given the Stern-E-Fix corset (12.5 days vs. 18 days [p = 0.002]) versus patients discharged with elastic bandage.
Other best practices
In addition to the strategies mentioned above, emphasis should also be given to other best practices such as pre-operative and intra-operative glycemic control, double gloving, atraumatic chest opening and closure, vest for chest support post-procedure, and much irrigation to minimize the risk of DSWI.
Glycemic control
Elevated mean blood glucose levels within the first 48 hours after surgery are associated with increased risk of DSWI [26]. Incidence of DSWI in patients with diabetes mellitus can be reduced by maintaining glucose level belows 200 mg/dL in the immediate post-operative period [26]. Furnary et al. [25] found that continuous insulin infusion to maintain glucose level below 200 mg/dL decreased the risk of DSWI by approximately 66%. Glycemic control by continuous infusion substantially reduces the incidence of DSWI compared with sliding-scale insulin [82]. Kramer et al. [83] developed a tight glycemic control program that replaced text-based instructions with a color-coded nomogram for the orders of continuous insulin infusion to make it easier to be implemented. An educational program was also initiated to highlight the impact of hyperglycemia on post-operative cardiac surgery patients and its impact on infection. At the same time, the blood glucose level range was reduced from 80–150 mg/dL to 80–120 mg/dL. After 18 months of implementation of the program, DSWI rates decreased substantially from 2.6% to 1%, representing a 62% decrease in DSWI [83].
Treatment
Culture-directed antibiotic agents and thorough surgical debridement are the standard treatment of DSWI [84]. Vacuum-assisted closure (VAC) is also a common therapy in the treatment of DSWI. It not only assists in definitive closure but can act as bridge to reconstruction. The use of VAC therapy has also shown to improve survival in patients with DSWI [85,86]. However, to prevent complications short-term use is advised [87,88]. Flap reconstruction is the standard therapy for DSWI, the use of which promotes early wound closure and reduces major complications and mortality [84]. In patients with diabetes mellitus, omental transposition has been used as an initial surgical therapy based on its advantage of decreased need for flap revision. Recently, sternal plating has been used and is beneficial in stabilizing the sternum in select patients [84].
Conclusion
Given that the risk of DSWI has decreased substantially in recent years and that a number of DSWI preventive strategies that have shown promising results are now available, BITA grafting should be used more frequently in patients undergoing CABG. Cardiothoracic surgeons should make themselves aware of and utilize all strategies that have the potential to decrease the risk of DSWI. With careful patient selection and effective use of these preventive strategies, the risk of DSWI can be reduced to zero. This would in turn lead to the maximization of use of BITA grafts in patients undergoing CABG. Given the well-established survival benefit, we believe that coronary revascularization involving BITA grafting should be a common operation for the majority of patients and may also be a quality metric in patients at low risk of developing DSWI. However, it may be best to avoid BITA in obese females with diabetes mellitus with diffuse atherosclerotic burden because these patients are at the highest risk of developing DSWIs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.