
Abstract
Abstract
Background:
Normal skin microbiota influence susceptibility to surgical infections. The distribution of skin bacteria differs by anatomic site, and given the right conditions, almost any of these bacteria can become an opportunistic pathogen.
Methods:
This paper provides a thorough review of the most commonly encountered bacteria in various regions of the body and their isolation from operative incisions at those locations. These data may be useful in optimizing targeted antibiotic therapy for surgical site infections and provide a better understanding of the skin biome distribution at specific surgical sites.
Conclusion:
Typical skin-borne flora, surgical site infections, orthopedic infections by body part, and drug-resistant pathogens are reviewed.
Understanding which microbial species are present on the skin and mucosal tissues has become a useful method for predicting which pathogens are likely to be isolated from surgical site infections (SSIs). Some species of skin-borne bacteria and fungi are found predominately at specific sites on the body; therefore, understanding their distribution will help identify whether their presence at a particular surgical site is to be expected. Knowledge of the common skin biome and the respective locations during surgical intervention will allow more informed selection of antibiotics to prevent or manage SSIs.
Normal Skin Microbiome
Roughly one trillion bacteria live on human skin. Until recently, our knowledge of the skin microbiota has depended largely on media culture assays, although it is estimated that fewer than 1% of bacterial species can be cultured [1]. Phylogenetic identification via 16s ribosomal RNA gene sequences, which carry a common threshold of approximately 97% sequence identity, allows species-specific phylotype determination [2].
Recent studies have shown significant intra-personal and inter-personal variability in the composition of bacterial communities. Fierer et al. observed that microbiota on the two hands of the same individual shared only 17% of their phylotypes, and those of different individuals shared only 13% [3]. Furthermore, it was noted that women had distinctly higher bacterial diversity than men, and community composition was affected significantly by handedness, time since last hand washing, and an individual's sex.
The most commonly characterized skin-borne bacterium is Staphylococcus aureus, which is carried by approximately one-third of the population in the anterior nares, as well as on the skin and in the respiratory tract [4–8]. Staphylococcus aureus is a commensal organism of the normal skin biome; however, if the skin barrier is disrupted, it can cause infection. Indeed, the organism is the most prevalent pathogen isolated from skin and soft tissue infections (SSTIs) [9,10]. With an estimated incidence of 32 infections per 100,000 persons, S. aureus has surpassed Streptococcus pneumoniae and Haemophilus influenzae as the most common invasive bacterial pathogen in the United States [11,12].
In general, bacterial diversity and composition are dependent on the normal physiology of the skin site, with specific bacteria associated with moist, dry, and sebaceous environments [13]. Diversity seems to be lowest around regions rich with sebaceous glands, suggesting that a specific subset of organisms can better tolerate these regions. Areas such as the back, forehead, retroauricular crease, and alar crease exhibit low phylotype diversity [13–15]. Propionibacterium species, such as P. (Cutibacterium) acnes, are the dominant organisms at these sites, which supports classical microbiological studies describing these species as lipophilic residents of the pilosebaceous unit (Table 1) [13].
Proportion of Major Bacterial Groups when Sites Are Clustered into Microenvironments
Staphylococcus and Corynebacterium spp. are the most dominant organisms colonizing moist areas, which is consistent with culture data, suggesting that these organisms prefer regions of high humidity [1,13,15]. Moist sites include the umbilicus, axilla, inguinal crease, gluteal crease, sole of the foot, popliteal fossa, and antecubital fossa. The sites with the highest bacterial diversity are the dry areas, such as the forearm, buttock, and various regions of the hand, which display mixed representation from the phyla Actinobacteria, Proteobacteria, Firmicutes, and Bacteriodetes [1,13,15].
Skin, Soft Tissue, and Surgical Site Infections
Most SSIs are associated with skin-derived gram-positive cocci, including S. aureus, coagulase-negative staphylococci (CoNS) (usually Staphylococcus epidermidis), streptococci, and Enterococcus spp. [16,17]. In addition to SSIs caused by staphylococci, gastrointestinal and some head and neck operations have a higher likelihood of being associated with infection caused by enteric aerobic (e.g., Escherichia coli) and anaerobic (e.g., Bacteroides fragilis) gram-negative bacilli [18,19].
Overall, S. aureus is the pathogen most commonly encountered in infections following surgical procedures. Table 2 outlines some of the pathogens commonly associated with various surgical procedures. From the accrued data, it appears that specific types of procedures align with specific groups of organisms [20], thus providing a possible map for use in prophylactic care.
Pathogens Commonly Associated with Different Surgical Procedures
CoNS = coagulase-negative staphylococci [17].
The SENTRY Antimicrobial Surveillance Program database provides a long-term analysis of the microbial causes of skin and soft tissue infections in hospitalized patients [21]. The pathogens most consistently encountered over time are S. aureus, Pseudomonas aeruginosa, E. coli, and Enterococcus spp.
The microbiology of SSTIs can differ remarkably with the means of entry (Table 3) [22]. The cause of SSTIs may be normal host flora transferred from an instrument or from the environment [23,24]. Etiologies can differ significantly between hospital-acquired and community-acquired SSTIs. As mentioned, hospital-acquired SSTIs are caused predominantly by S. aureus, whereas community-acquired SSTIs typically are caused by β-hemolytic streptococci, usually Lancefield groups A, C, and G, with group B being seen in patients with diabetes mellitus and in the elderly [25–29]. Clinically, the microbial etiology of SSTIs often can be predicted with some accuracy. Localized pus-producing lesions such as boils, abscesses, and carbuncles usually are staphylococcal in etiology. Alternatively, rapidly spreading infections such as erysipelas, lymphangitis, and cellulitis typically are caused by β-hemolytic streptococci [25], which also are prevalent in cases of necrotizing fasciitis.
Etiologic Risk Factors for Skin and Soft Tissue Infections and Their Associated Bacterial Causes
Data from reference 19.
Orthopedic Infections
Orthopedic-specific procedures make up a significant number of all operations. For example, when Molina et al. surveyed the American College of Surgeons' National Surgical Quality Improvement Program (NSQIP) to quantify the number of orthopedic procedures performed between 2005 and 2011 in more than 400 hospitals around the world [30], they found that orthopedic procedures accounted for roughly 7% of all operations. Of these, total knee arthroplasty (TKA), total hip arthroplasty (THA), and knee arthroscopy with meniscectomy comprised 55% of all orthopedic procedures, which matched the numbers reported by the American Academy of Orthopaedic Surgeons in their 2014 practitioner census [31]. Other frequently performed procedures are laminectomy and nerve root decompression, total shoulder arthroplasty, and revision TKAs and THAs. Among the most frequently performed procedures, those investigators found a 5% complication rate [30].
As the United States' population continues to age, the prevalence of age-related disorders, such as osteoarthritis, will continue to rise. According to the Centers for Disease Control and Prevention (CDC), the total number of THAs and TKAs performed has been increasing. In 2010, approximately 332,000 primary THAs and 719,000 primary TKAs were performed on patients 45 years or older [32]. Kurtz et al. project that by 2030, the demand for THAs will increase by 174% and the demand for TKAs by 673%, accounting for roughly 3.48 million surgical procedures annually [33].
As the total number of orthopedic procedures increases, a concurrent rise in the number of SSIs is expected. Furthermore, the incidence of musculoskeletal infection, including peri-prosthetic joint infection, soft tissue infection, septic arthritis, and osteomyelitis, is increasing in proportion to the aging population and higher rates of diabetes mellitus and obesity [34]. Therefore, a thorough understanding of which types of bacterial infections are most prevalent at each surgical site can benefit subsequent intervention greatly. Figure 1 describes some of the most common surgical interventions at each anatomic site, as well as the pathogens most commonly found in the associated SSIs.
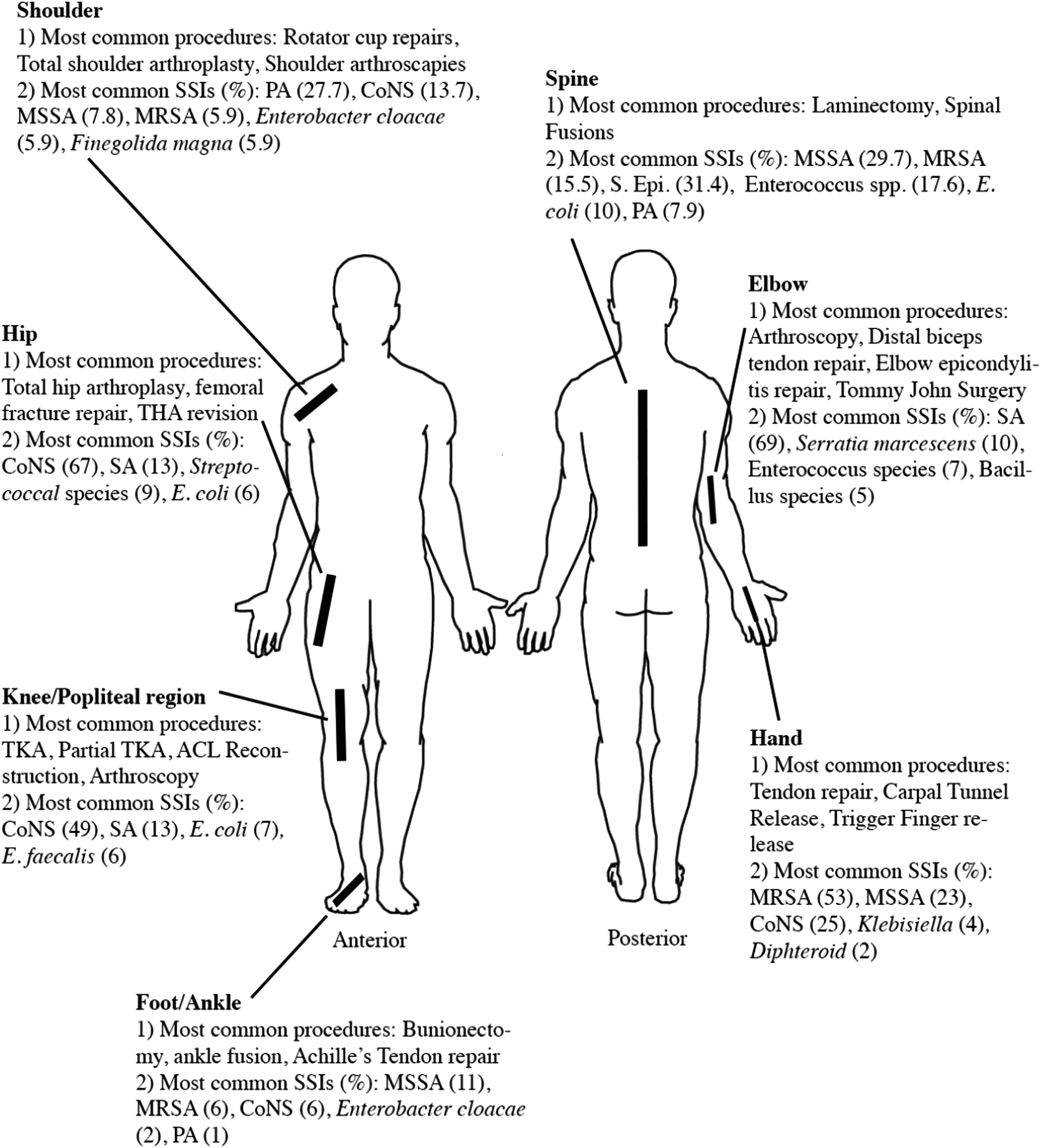
As Figure 1 details, frequent surgical sites, including the spine, shoulder, elbow, hand, hip, knee, and foot and ankle, are associated with various commonly cultured pathogenic species when post-surgical infection occurs. These data are represented in Table 4.
Pathogen Species Most Commonly Isolated from Infections after Non-Emergency Spinal Surgery by Site
Staphylococcus aureus is the most common pathogen in infections of the spine, elbow, hand, and foot and ankle, accounting for 45.2%, 69%, 76%, and 17% of infections, respectively (Table 4) [35–38]. Although they share the most common etiologic agent, the incidence of SSIs at these sites differs greatly. In spine surgery, for example, the overall incidence of SSIs ranges from 0.5% to 18.8% [39]. In contrast, because of its thin soft-tissue envelope, SSIs resulting from surgical intervention on the elbow are frequent, with an incidence of 4.5% [40]. Rates of post-operative infection in hand surgery are poorly documented but include a wide range of both emergency and non-emergency procedures. The incidence of SSIs in hand surgery has been reported to be as high as 9.7% [41]. Lastly, because of the wide array of procedures involving the foot and ankle, the incidence of SSIs associated with these interventions ranges from 1% to 8% [42].
Currently, CoNS are the most common pathogen in SSIs of the hip and knee, accounting for 67% and 49% of post-operative infection at these sites, respectively. At both sites, S. aureus is the second most commonly isolated pathogen but is becoming increasingly implicated in infections (Table 4) [43,44]. With regard to hip surgery, the rate of infection differs significantly depending on the procedure, with SSI rates reported to be as low as 1% for non-emergency cases [45]. Likewise, the incidence of SSIs during knee surgery is low, ranging from 0.86% to 2.5% [46].
The incidence of SSIs in shoulder surgery ranges from 0.76% to 5.8% [47]. In contrast to the sites discussed earlier, SSIs after shoulder surgery are not caused predominantly by S. aureus or CoNS but rather often by P. acnes, the most commonly isolated pathogen in shoulder-related SSIs, accounting for roughly 27.5% of such infections [48,49]. Propionibacterium acnes requires 14 days to culture, and contamination often is mistaken for pathogen growth. Because it is notoriously difficult to culture and quantify, P. acnes typically is underdiagnosed as a cause of infection. Additionally, the organism has shown resistance to commonly used skin preparation agents, such as chlorhexidine gluconate [50]. Thus, it is possible that the prevalence of P. acnes in shoulder SSIs is underestimated.
Skin Preparation Prior to Incision in Orthopedic Surgery
A plethora of skin preparation solutions are currently used prior to incision, with the goal of removing skin-dwelling bacteria to prevent inoculation of the incision during surgery. Because the skin microbiome differs across locations, it is reasonable that different skin preparation methods are favored depending on the operative site. Commonly used preparations include ChloraPrep, which is 2% chlorhexidine gluconate and 70% isopropyl alcohol (BD, Franklin Lakes, NJ); DuraPrep, 0.7% iodophor and 74% isopropyl alcohol (3M, Chelmsford, MA); povidone–iodine scrub and paint (0.75% and 1.0% iodine, respectively); Techni-Care, 3.0% chloroxylenol (Care-Tech Laboratories, St. Louis, MO); Betadine 10% povidone–iodine; and 2% chlorhexidine gluconate (CHG) cloth.
In shoulder surgery, ChloraPrep is more effective than both DuraPrep and povidone–iodine scrub and paint at removing bacteria from the region, with post-treatment positive-culture rates of 7%, 19%, and 31%, respectively. Although ChloraPrep and DuraPrep are more effective than povidone–iodine at eliminating CoNS from the shoulder, all are equally able to remove P. acnes. Of note, there was no difference among the preparation agents in the post-operative infection rate [51].
Similarly, ChloraPrep is more effective than DuraPrep and Techni-Care at eliminating bacteria from the skin prior to foot and ankle surgery. However, ChloraPrep still was associated with a high post-application positive culture rate, 21%, and there were no significant differences in the rate of post-operative infections among the three agents [52].
When comparing Betadine, DuraPrep, and Chloraprep as preparation for hand surgery, the overall culture rates are 43.2%, 30.4%, and 40%, respectively. Both Betadine and DuraPrep are more effective than ChloraPrep at removing Bacillus, but this organism rarely causes SSIs [37,53]. All three solutions yield equally low rates of positive CoNS and P. acnes cultures. Similar results were obtained in shoulder and foot and ankle surgery; the three preparations did not differ in the post-operative infection rate [53].
In the lumbar spine, ChloraPrep and DuraPrep yield similar post-preparation positive culture rates: 0 and 6%, respectively. Pathogens present on the skin after DuraPrep application were Propionibacterium and Peptostreptococcus [54]. However, on the upper back, where P. acnes commonly resides, ChloraPrep is ineffective at penetrating deep into the dermal layer, and persistence of P. acnes is seen in as many as 70% of patients [55].
With hip and knee surgery, at-home use of a 2% CHG cloth prior to surgery shows additional benefits. Applying this cloth to the surgical site the night before and the morning of surgery reduced the infection rate by half (3.19% to 1.59%) [56]. The rate of SSI after total hip arthroplasty was reduced further when the cloth was applied to the whole body as opposed to only the hip. Additionally, two at-home total body 2% CHG applications followed by DuraPrep application in the operating room consistently resulted in fewer SSIs than DuraPrep alone [57,58]. However, it is unclear which pathogens contributed to SSI and which were eliminated by skin preparation.
Drug-Resistant Bacteria Strains
Clinically important drug-resistant bacteria that commonly cause nosocomial infections include methicillin-resistant S. aureus (MRSA), methicillin-resistant CoNS, vancomycin-resistant enterococci, and multi-drug-resistant gram-negative bacilli, including strains of Pseudomonas aeruginosa and E. coli [59]. Each of these will be considered in turn, with a special focus on MRSA S. aureus.
Methicillin-resistant Staphylococcus aureus (MRSA)
In orthopedics, staphylococci are the primary cause of implant-related infections, being responsible for nearly 80% of all prosthetic infections [60]. Although initially considered primarily a nosocomial pathogen, MRSA has become increasingly prevalent over the last several years. The CDC reports that 0.8% to 1.5% of the general public is now colonized by MRSA, which accounts for nearly 60% of all S. aureus isolates recovered from hospital intensive care units [61]. At present, it is projected that MRSA infections account for more than 100,000 hospitalizations each year in the United States [62].
Considerable variation in the resistance rate of S. aureus to methicillin has been noted between countries and continents, with the highest rate in North America (35.9%), followed by Latin America (29.4%) and Europe (22.8%) [21]. The MRSA strains are further classified into either community-acquired (CA) or healthcare-acquired (HA), with each type differing in pathogenicity, virulence, antibiotic resistance profile, and the patient population affected [63]. However, the boundaries between HA-MRSA and CA-MRSA are becoming blurred because of the movement of patients between hospitals and the community [64,65]. For example, there are many documented HA outbreaks of CA-MRSA following the admission of colonized or infected patients [65]. In the United States, where CA-MRSA is becoming common, it is increasingly difficult to distinguish between CA- and HA-MRSA on clinical and epidemiologic grounds [64,66]. Because HA- and CA-MRSA strains often are genotypically and phenotypically different, the microbiological characteristics of the isolates may help to distinguish between the two types of infection [27,67]. Methicillin-resistant S. aureus colonizes the anterior nares, throat, rectum, and skin (axilla, inguinal area, and perineum) [5–8, 68–71]. Roughly 10% of healthy individuals in the United States are colonized with MRSA, and the prevalence has increased significantly over the past decade, accompanied by an increase in MRSA infection rates [68,72]. Whereas notable risk factors for acquiring HA-MRSA include antibiotic use, MRSA carriage, proximity to infected individuals, prolonged hospitalization, intensive care admission, and hemodialysis, CA-MRSA typically is associated with skin and soft-tissue infections in young and healthy individuals with no recent healthcare exposure [63,73–79].
Although CA-MRSA always has been a prominent cause of staphylococcal skin and soft-tissue infections, this drug-resistant pathogen has become increasingly prevalent recently. In a review of MRSA SSTIs in South Texas, there were fewer than 10 cases reported annually throughout the 1990s, but by 2003, roughly 500 cases were being reported each year [80]. By 2005, several centers across the United States reported that CA-MRSA accounted for nearly 75% of all staphylococcal infections [81]. With such unexpectedly high rates of CA-MRSA, changes in empirical antibiotic therapy were needed whenever MRSA was suspected, particularly for SSTI, among which more than 50% were caused by CA-MRSA [80–85]. A retrospective review of more than 40 tertiary-care children's hospitals in the United States identified almost 60,000 children with S. aureus infections from 2002 to 2007. Of those, 51% were infected with MRSA. Over the course of the years studied, MRSA rates increased significantly, whereas rates of methicillin-sensitive S. aureus infection remained stable. Of the nearly 40,000 patients whose type of infection was identified, 61% had SSTIs. As a result, the authors deduced that the increasing rate of MRSA infections is driven largely by an increase in SSTIs [88].
Children and African Americans are disproportionally affected by increases in CA-MRSA [87–89]. Additionally, military personnel, prisoners, and athletes exhibit larger numbers of SSTIs caused by CA-MRSA [76,89–95]. In each of these high-risk groups, the risk factors for infection are close contact, compromised skin integrity, and an increased prevalence of colonization. Furthermore, outbreaks often are linked to periods of more common colonization or exposure to specific strains of S. aureus, such as USA300 CA-MRSA [96].
Multi-resistant and opportunistic pathogens
Overall, antibiotic-resistant pathogens other than MRSA, namely, methicillin-resistant CoNS, vancomycin-resistant enterococci, and extended spectrum beta-lactamase-producing gram-negative bacteria, have been associated increasingly with healthcare-acquired infections [97, 98]. Moreover, there are various other bacterial pathogens known to be opportunistic infectious agents, especially in orthopedics.
Pseudomonas aeruginosa typically is present on the skin (Proteobacteria). The organism is most commonly associated with infections in immunocompromised individuals and burn victims and often is multi-drug resistant [99]. Although P. aeruginosa typically is not enteric, it has been identified recently as a gastrointestinal source of blood stream infections after hematopoietic stem-cell transplantation [100].
Serratia is another gram-negative opportunistic pathogen of the Enterobacteriaceae family that typically is spread by hand-to-hand contact. Serratia marcescens is the most pathogenic species within the genus and a frequent cause of healthcare-acquired infections, particularly after spinal surgery. The bacterium is prevalent in the environment and causes a wide range of healthcare-acquired infections, such as respiratory tract infections, osteomyelitis, urinary tract infections, and endocarditis [101–105].
Enterococcal species, such as vancomycin-resistant Enterococcus faecalis (VRE) and Enterococcus faecium, are gut bacteria that frequently colonize orthopedic and soft tissues and typically spread through direct contact. Enterococci have become the second most common organisms recovered from nosocomial urinary tract and wound infections and one of the most common causes of nosocomial bacteremia in the United States [106].
Escherichia coli also accounts for many soft tissue infections. This organism has been identified as a causative agent of many conditions, including, but not limited to, cellulitis localized to the lower or upper limbs, necrotizing fasciitis, surgical site infections, and infection after burn injuries [107–112].
Fungal pathogens
Several common fungal pathogens are opportunistic infectious agents.
Candida albicans is a commensal fungus that resides mainly on human mucosal surfaces. It is a known opportunistic pathogen in immunocompromised individuals and commonly is associated with biofilm formation, making it difficult to eradicate [113]. It is the third leading cause of infections associated with intravascular catheters, having the second highest rate of colonization transitioning to infection and the highest overall crude mortality rate [114,115]. Notably, C. albicans can colonize prosthetic devices either endogenously or exogenously. Other Candida species notable for healthcare-acquired infections are C. glabrata, C. parapsilosis, C. krusei, and C. tropicalis [116–120].
Cryptococcus neoformans is an encapsulated fungus that causes life-threatening meningoencephalitis in immunocompromised individuals. It colonizes and subsequently forms biofilms on various prosthetic devices, including ventricular shunts, peritoneal dialysis fistulas, and cardiac valves [121–124].
Although normally it is a benign fungus, some species of Trichosporon can disseminate in immunocompromised hosts, leading to systemic disease. Trichosporon has been associated with infections related to devices such as catheters, breast implants, and cardiac grafts [125–127].
Lastly, various fungi have been isolated as opportunistic agents in specific situations. Blastoschizomyces capitatus has been associated with catheter-related fungemia, and M. pachydermatis has been isolated from infected patients receiving parenteral nutrition. The baker's yeast Saccharomyces cerevisiae has been found in association with the dentures of patients with stomatitis, and persistent meningitis has been linked to a C. immitis biofilm at the tip of ventriculoperitoneal shunt tubing [117,128–130]. Aspergillus fumigatus has caused infections of medical implant devices, including cardiac pacemakers, joint prostheses, and breast implants [131,132].
Conclusion
During surgical interventions, understanding which species of flora-bacteria are already present on the skin and mucosal tissues at various anatomic sites can help prepare providers for post-operative surgical infections. Furthermore, this knowledge allows surgeons to implement more specific and effective preventative measures in the pre-operative stages. Orthopedic-specific operations make up a significant number of all surgical procedures, and these numbers are expected to rise considerably over the next several years. Better recognizing which pathogens are typically found at specific anatomic sites and during specific procedures may improve surgical and medical interventions for peri-operative infections.
Footnotes
Acknowledgements
We thank Diane N. Weiss and the Sipprelle Family Foundation for their continued support.
Author Disclosure Statement
Dioscaris R. Garcia holds equity in BI Medical, LLC. Adam E. M. Eltorai, MSc receives royalties from LWW and Springer. John D. Jarrell holds equity in and is a Board member of Biointraface, Inc. and holds equity in and is a consultant for BI Medical, LLC. Christopher T. Born holds equity in and is a board member of Biointraface, Inc. and holds equity in and is a consultant for BI Medical, LLC and Illuminoss, LLC. David Deckely, Carole SL Spake, Jack M. Haglin, Toby Emanuel, and Cory Mayfield have no disclosures.