
Abstract
Abstract
Background:
No consensus exists regarding duration of antibiotic therapy for complicated appendicitis treated with interval appendectomy. We hypothesized that more than two weeks of antibiotic therapy does not decrease complication rates in asymptomatic patients.
Patients and Methods:
A retrospective review of all patients with complicated appendicitis treated with interval appendectomy from 2010–2015 was performed. We divided the patients in two groups (group 1, ≤2 weeks of antibiotics; group 2: >2 weeks of antibiotics). Demographics, antibiotic agents, and complications were collected. Pearson χ analysis and Student t-test analysis was performed with significance of p < 0.05.
Results:
Total of 158 patients met inclusion criteria (group 1 [47.4%] vs. group 2 [52.5%]). Mean length of stay was 7.5 days. Abscess on admission was 26% (n = 41). The groups were demographically similar. Total complication rate was 39.2% (abscess development, n = 19; re-admissions, n = 16; interval appendectomy <28 days, n = 13; unplanned emergency department visits, n = 7; fistula, n = 4, wound infection/dehiscence, n = 3; and conversion to open surgery, n = 4). All fistulas and conversions occurred in the less than two-week group. Mean course of antibiotics was 4.1 weeks. There was no significant difference in the complication rates based on duration or type of antibiotics (p = 1.0).
Conclusion:
Treatment with more than two weeks of antibiotic therapy for complicated appendicitis does not confer any clinical benefit prior to interval appendectomy. Complications were not reduced by a prolonged course of antibiotic therapy.
A
Appendicitis is considered complicated or advanced when perforation of the appendix has developed. Complicated appendicitis typically presents with classic clinical findings of acute appendicitis such as right lower quadrant tenderness, elevation of white blood cell (WBC) count, generalized tenderness/peritonitis, signs of systemic inflammatory response syndrome (SIRS), and evidence of perforation on diagnostic imaging such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI) [4–6]. Complicated appendicitis typically occurs because of delay in presentation to the emergency department or delay in diagnosis [7].
The treatment of complicated appendicitis is controversial. Some advocate that an urgent laparoscopic appendectomy results in better outcomes whereas others report a high rate of complications with urgent appendectomy and instead opt to treat patients with antibiotic agents and perform an interval appendectomy after the appendix is no longer acutely inflamed [8–15]. These patients are treated with a combination of intravenous or oral antibiotic agents and percutaneous drainage of abscess when present. This approach was believed to decrease conversions to open surgery, decrease morbidity, and decrease extensive resections (right hemi-colectomy). Although almost all patients respond well to this initial conservative management, recent data show an increased complication rate for patients treated with an interval appendectomy [16]. As part of a quality improvement project for patients with complicated appendicitis, we decided to evaluate our own experience regarding the length of antibiotic treatment needed for patients undergoing interval appendectomy. We found that the duration of antibiotic therapy in interval appendectomy was not standardized in our practice, nor is there a defined standard in the reported literature [8–15]. We aimed to determine whether duration of oral antibiotics of longer than two weeks results in better outcomes compared with less than two weeks in patients with complicated appendicitis.
Patients and Methods
As part of a quality improvement project, we evaluated the duration of discharge antibiotic therapy in patients who had been managed for complicated appendicitis. We defined our complications as re-admissions, abscess formation during treatment, return to the emergency department with abdominal pain, interval appendectomy less than 28 days, conversions to open surgery, development of fistulas, surgical site infections, and wound dehiscence. Using International Classification of Diseases (ICD) 9 codes for all forms of appendicitis, patients treated at Cardinal Glennon Children's Hospital/Saint Louis University between 2010 and 2015 were retrieved from the electronic health record (EHR) database. A total of 949 patients were treated for appendicitis in the five-year time period. A retrospective chart review of all patients who were managed for complicated appendicitis was performed. Prior to this study there was no defined criteria for complicated appendicitis, thus we used surgeon's description in the operative note or admission note describing perforation. There were 330 patients managed for complicated appendicitis. All patients who underwent appendectomy during the index admission were excluded. All patients who were considered to have perforations by surgeon and received (intravenous) antibiotic agents during the index admission with plans for subsequent interval appendectomy were included from analysis (Fig. 1). Data collected included patient demographics, presenting history and physical examination findings, laboratory examination findings, discharge antibiotic type and duration, and patient complications.
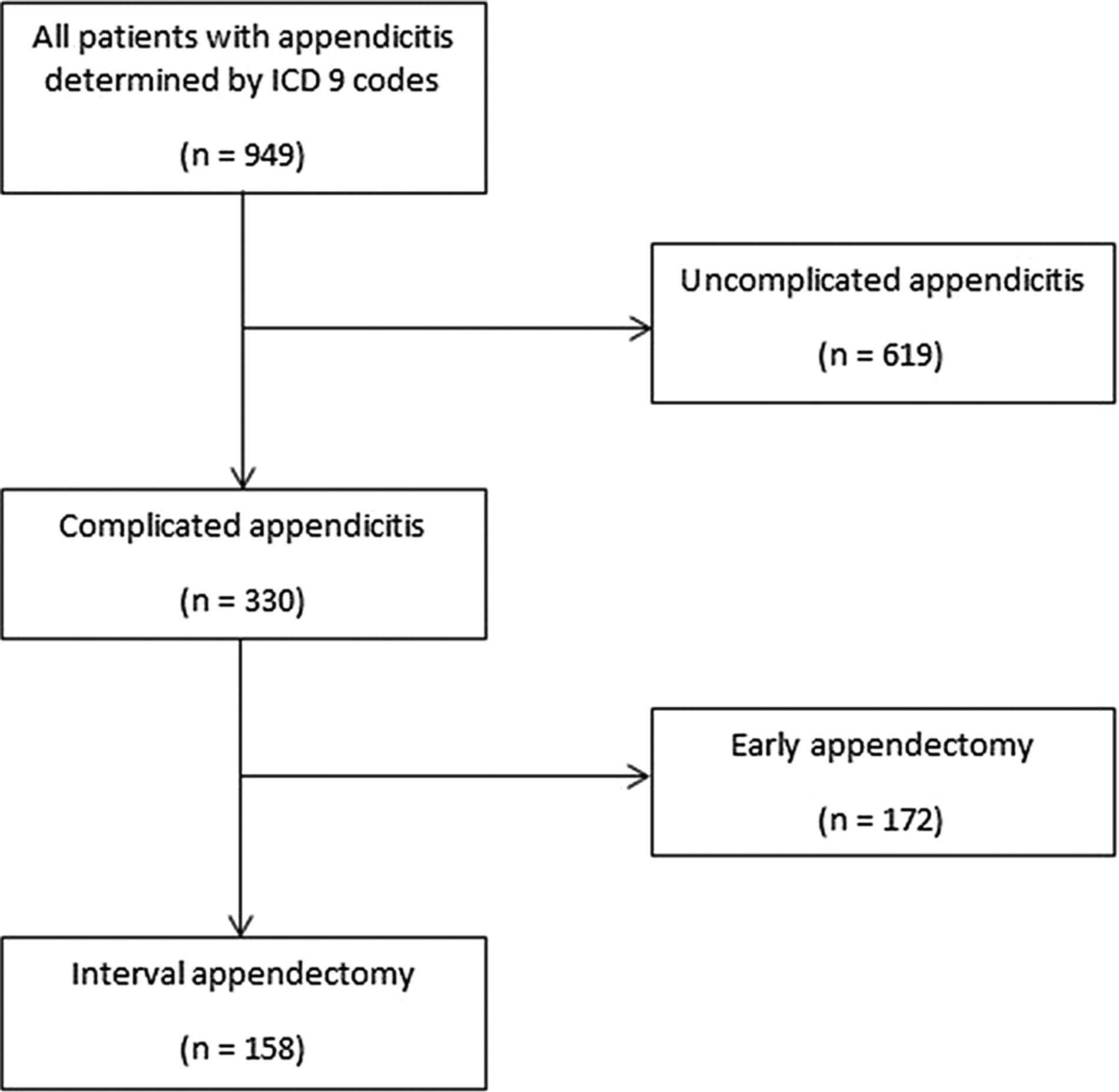
Patients with appendicitis.
To date some of these patients were being treated with up to six weeks of outpatient oral antibiotic agents as decided by the treating surgeons. Patients were divided into two groups for analysis. The duration of discharge antibiotic agents was based on the prescribed antibiotics length, and not on the actual number of days reported by patients. Group 1 patients received two weeks or less of antibiotic agents, whereas group 2 received more than two weeks of antibiotic agents (intravenous or oral). All patients were discharged within 24 hours after achieving three uniform discharge criteria: ability to tolerate diet, resolution of abdominal pain, and no fevers in a 24-hour period. Decision regarding discharge antibiotic duration was not based on the severity of initial symptoms but rather was surgeon-specific. Groups were compared by demographic data and presenting variables. They were also compared for the aforementioned variables. Pearson χ2 analysis was performed for the categorical variables whereas Students t-test was used to analyze the continuous variables. Mann-Whitney U test was performed for non-parametric continuous data.
Results
One hundred fifty-eight patients met inclusion criteria. Of these 47% (n = 75) received two weeks or less of antibiotic agents (Fig. 2). Of the group 1 patients, 81% (n = 61) went home on oral antibiotic agents only, two patients were discharged with intravenous antibiotic agents, and 12 patients had no discharge antibiotic therapy prescribed whereas all the patients in group 2 went home on oral antibiotics only.

Patients by group.
Mean age of admission was 9.9 years (10.5 years in group 1 vs. 9.6 years in group 2). Females constituted 47% of the patients in group 1 and 40% of those in group 2. Among group 1 patients, median duration of symptoms before presentation was three days (0–21 days) compared to two days (1–28 days) in group 2. There were no racial differences in either group with 71% Caucasian in group 1 and 74% Caucasian in group 2. Mean admission weight was 41.6 kg in group 1 and 43.5 kg in group 2. There were no differences between the groups based on the mean age at admission, race, gender, admission weight, and duration of symptoms (Table 1).
Demographics
SD = standard deviation; n: number.
Mean duration of intravenous antibiotic agents was 6.6 days in group 1 and 5.8 days in group 2 (p = 0.23). Mean total length of stay was 7.8 days in group 1 and 7.2 days in group 2. Only 41 (26%) patients upon admission had imaging confirming an abscess, of which 29 (71%) required drain placement. The total complication rate was 39.2%. In group 1, complications were abscess development during or after treatment in 13 patients (11 drains placed during initial admission and 2 drains placed after discharge), interval appendectomy less than 28 days in nine patients, re-admissions in seven patients, return to the emergency department with abdominal pain in three patients, conversion to open in two patients. In group 2, complications were re-admissions in nine patients, abscess development during or after treatment in six patients (six required drain placement), interval appendectomy less than 28 days in four patients, return to the emergency department with abdominal pain in four patients, fistula in four patients, conversions to open surgery in two patients, surgical site infection in two patients, and one wound dehiscence (Table 2). Reasons for early interval appendectomy were return to the emergency department for worsening abdominal pain, fever, vomiting, or inability to tolerate diet. Between the two groups, there was no difference in the complication rates or complication types (p = 1.00). Average time to interval appendectomy was in 55.9 days group 1 and 56.8 days in group 2 (p = 0.88). During the time of interval appendectomy, 22% (n = 17) of the procedures were considered difficult per the operative note in group 1 versus 33% (n = 28) in group 2 (p = 0.58). Average discharge antibiotic duration was 1.7 weeks in group 1 and 5.8 weeks in group 2 (p < 0.001).
Outcomes and Complications
SD = standard deviation; n = number; Abx = antibiotic agents; IA = interval appendectomy; IV = intravenous.
The most common discharge antibiotic therapy was a combination of Augmentin® (GlaxoSmithKline, Philadelphia, PA) and Flagyl® (37.5%, n = 54; (Pfizer, New York, NY) versus Flagyl alone (39%, n = 56). Average time to interval appendectomy was 55.8 days in group 1 versus 56.8 days in group 2 (Table 3). Although there is a substantial difference between the types of antibiotic agents used between the two, there was no difference in complication rates based on the type of antibiotic agents used. When Flagyl is used as the sole antibiotic, it was likely that the duration of antibiotic was longer than two weeks. When patients were allergy to penicillin (<5%), other antibiotics prescribed included ciprofloxacin, clindamycin, and trimethoprim-sulfamethoxazole. Antibiotic allergy did not influence patient selection, because Flagyl was the biggest predictor of duration over 2 weeks.
Type of Outpatient Antibiotic Agents
n = number.
Of the patients with drains placed, abscess cultures were obtained in 76%. No organisms were cultured in 26%. However, when present, the most common organisms cultured were Escherichia coli and Bacteroides spp. Other organisms present were Haemophilus parainfluenzae, Candida spp., and Clostridium spp. (Table 4).
Type of Organisms Cultured from Abscess by Group
n = number.
Discussion
Uncomplicated appendicitis is a common diagnosis in pediatric patients with most patients managed successfully with early appendectomy. However, the management of complicated appendicitis remains controversial, despite most recent literature [16–18]. Whereas early appendectomy should be the rule for treatment for all types of appendicitis, the role of interval appendectomy should not be eliminated from the armamentarium of pediatric surgeons. We believe that this option will likely benefit a small subset of patients in whom duration of symptoms and presence of abscess could be taken into consideration. Our institutional practice is for patients undergoing interval appendectomy to be treated with intravenous antibiotics, with or without IR drain placement until discharge criteria is met. The discharge criteria include: ability to tolerate diet/oral antibiotic agents, lack of fevers for at least 24 hours, and resolution of abdominal pain. Patients were then discharged with varying duration of oral antibiotic agents, usually based on surgeon's preference without clear reason or definition.
Some of the main arguments for extended antibiotic therapy include decreased re-admission rates, decreased return to emergency department, decreased need for drainage, and less technically demanding operation on interval appendectomy. No data exist regarding length of therapy for this subset of patients. When we looked at our own institutional data, we noted a wide range of antibiotic choices and duration for patients undergoing interval appendectomy. In this study, antibiotic duration was decided based on the prescribed length, not on the actual number of days taken. We were not able to guarantee that the patients actually took the antibiotic agents as prescribed, because of the retrospective nature of the study.
The patients studied were divided into two groups based on the post-discharge intravenous or oral antibiotic duration. There was no difference in their pre-admission duration of symptoms, presence of abscess upon admission, or their total hospital length of stay. The groups were also similar in the types of organism cultured from abscess and the most commonly cultured organism was E. coli and Bacteroides species.
We found no statistical differences between complication rates regardless of the duration or antibiotic regimen chosen. Also, no differences were found in the reported difficulty of the procedure at the time of interval appendectomy. Commonly used antibiotic regimen included Augmentin only, Flagyl only, and Augmentin and Flagyl combination. Flagyl was the most common antibiotic used and was associated with an extended antibiotic course. However, absence of Flagyl in the shorter antibiotic course does not seem to worsen complication rates in our study population. More importantly, Augmentin alone is more effective in covering both aerobic and anaerobic bacteria. Based on these findings we concluded that there was no difference in outcomes with extended antibiotic therapy (>2 weeks) or type of antibiotic used. We believed this is important for patients and their families, because a shorter duration of antibiotic theapy reduces medication compliance issues and time away from school/work caused by medication side effects (nausea, diarrhea, etc.).
This study shows that duration of post-discharge antibiotic therapy of two weeks or less is sufficient for patients being managed with interval appendectomy. The major limitations of our study include; the non-standardization of patient selection process, given that this is a retrospective review and the lack of a pre-operative definition for complicated appendicitis. It is important to note that patients who were directed into the interval appendectomy pathway were based on individual surgeon preference with no pre-defined criteria. However, given the similarity in patient demographics, we believe that these potential biases are limited. Third, as mentioned before, a major limitation was the prescribed antibiotic length versus actual taken by the patient. Groups were divided based on the prescribed antibiotic length because we did not know or have the actual number of days that the patients took the medication because of the retrospective nature of this study. Another important question for future research is the length of antibiotic therapy for patients with source control after drainage. The Study to Optimize Peritoneal Infection Therapy (STOP-IT) trial found no substantial advantage with extended antibiotic course longer than four days for patients with intra-abdominal infections who have undergone a successful source-control procedure [19]. These findings could potentially have impacted both groups, although these findings have to be validated in children.
On the basis of these results, a quality improvement project is being undertaken at our institution with well-defined parameters for placement of patients into the interval appendectomy pathway. We are also instituting a standardized total of two-week course of antibiotic agents (intravenous/oral) in the interval appendectomy pathway patients.
Conclusion
Interval appendectomy is a useful management tool for complicated appendicitis. However, almost half of these patients will have complications despite the type or duration or antibiotics used. As such, when interval appendectomy is planned, there are no substantial benefits from an extended antibiotic course.
Footnotes
Author Disclosure Statement
No competing financial interests exist.