
Abstract
Abstract
Background:
Post-operative anastomotic leak (PAL) is the most feared complication after abdominal surgery. Timely drainage of enteric effluent is beneficial in the healing of PAL.
Methods:
We introduced a new and feasible approach for early active drainage of PAL using fine tube bundles (FTBs). The therapeutic effects of FTBs were observed prospectively and compared with the traditional drainage tube without FTBs in a non-blinded randomized controlled trial.
Results:
Sixty patients with PAL in two tertiary hospitals in China from 2010 to 2016 were included in this study. Of these patients, 30 received FTBs and 30 were treated with a traditional drainage tube. The implantation failure rate was zero in the FTB group. No statistical difference was observed between the two groups in terms of demographic data. After these interventions, patients in the FTB group showed a faster decline in infection-related indictors, a higher ratio of spontaneous PAL closure, and shorter treatment duration of antibacterial agents compared with those in the traditional drainage tube group. Fatal complications and financial cost were also reduced in the FTB group.
Conclusion:
Fine tube bundles may contribute to the healing of PAL through active drainage. This method should be validated by further clinical trials for wider use.
Surgical procedures such as intestinal resection have increased globally mainly because of the high incidence of intestinal tumor [1] and abdominal trauma [2]. Complications have a substantial influence on clinical outcome after surgery. Post-operative anastomotic leak (PAL) is regarded as the most severe complication and the leading cause of mortality [3]. The reported incidence of PAL varies from 1%–19% [4]. This variation is possibly associated with the risk factors for PAL in different patient cohorts including patient condition, disease type, and surgical technique [5].
The management of PAL depends on whether patients show specific disorders such as diffuse peritonitis or septic shock [6]. Generally, if these disorders are present, emergency surgery is required. Otherwise, conservative treatment should be considered, including source control, antibacterial agents, and nutritional support, and glue-assisted fistula healing [7,8]. Adequate source control has a particularly important role in eliminating infections at the early stage [9], thus creating a clean environment for PAL healing. However, most post-operative drainage approaches experience an incomplete and passive process, in which the drainage force is derived from the squeeze of continuously leaked enteric effluent. Therefore, a technique that can actively and completely drain the leaked contents is clinically important and essential.
This study aimed to introduce an active drainage method using fine tube bundles (FTBs). The fabrication and use of FTBs are illustrated in the following sections. Our hypothesis is that FTBs can drain the contaminated leak site more efficiently than a traditional drainage tube.
Patients and Methods
Application of FTBs
As shown in Figure 1, FTBs are composed of two sputum suction catheters and one epidural anesthetic catheter. One of the sputum suction catheters is 6F in size (Jiangsu Huatai Medical Devices Co., Ltd., Jiangsu, China) and its function is to connect with the atmosphere, thus balancing the air pressure surrounding the PAL. The size of the other sputum suction catheter is 8F (Jiangsu Huatai Medical Devices Co., Ltd.), which is designed to drain the leaked enteric contents with a negative pressure ranging from 10 kPa to 15 kPa. The epidural anesthetic catheter (Tuoren Medical Devices Co., Ltd., Xinxiang, China) was used to transfer normal saline to the leak site. The FTBs were inserted until the tip reached the first hole at the distal part of the traditional drainage tube (Nantong Angel Medical Instruments Co., Ltd., Jiangsu, China). If the FTBs became occluded during the drainage process, they were replaced. The traditional drainage tube is an open drainage technique, connected to a pack that collects the drainage fluid. If the traditional drainage tube was occluded, it was unclogged before the fistula tract was well formed. After the formation of fistula tract, it was replaced if occluded again. Formation of the fistula tract usually took approximately two weeks.
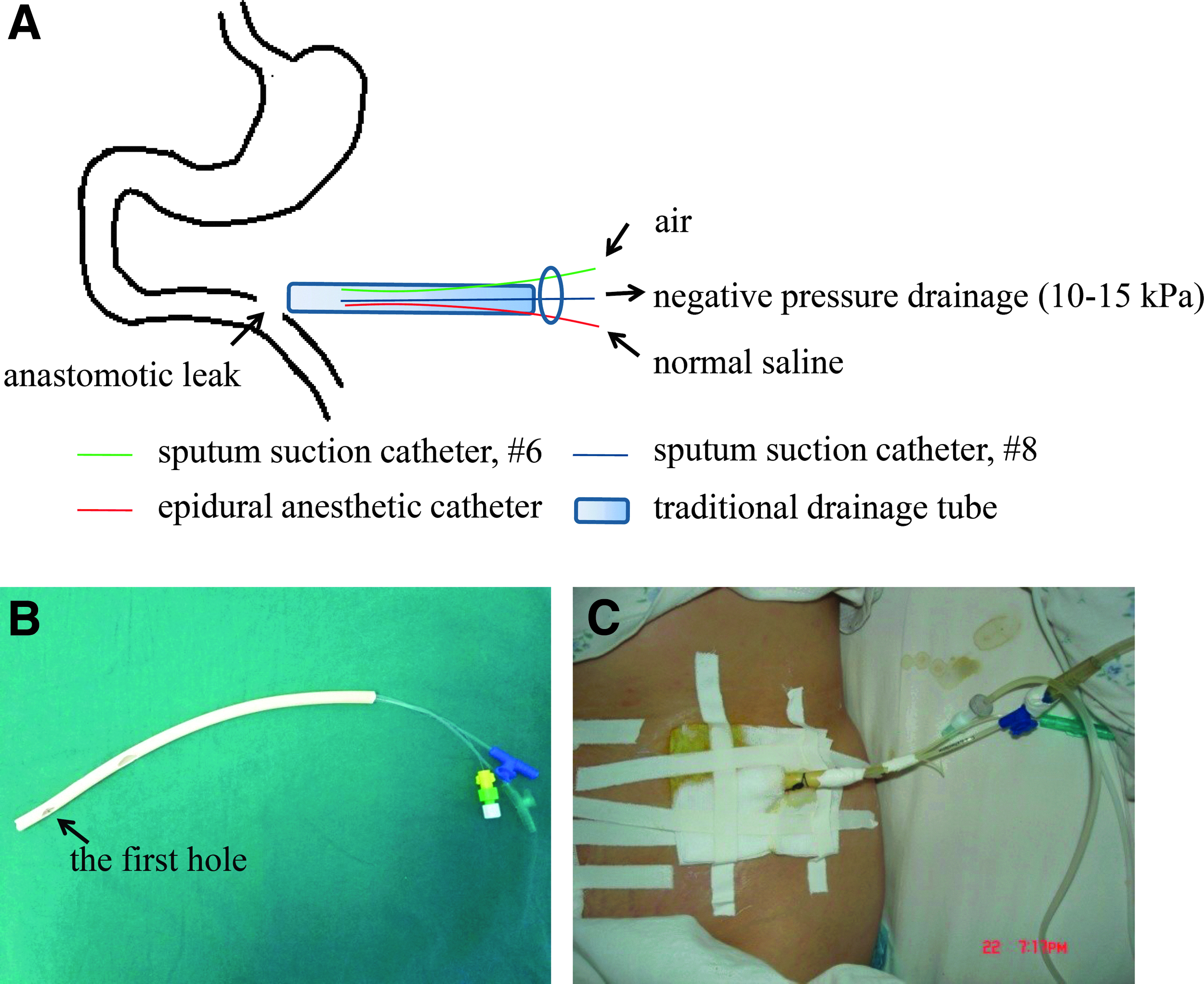
(
Inclusion and exclusion criteria
The inclusion criteria were patients aged 18 to 80 years and the diagnosis of PAL was confirmed by abdominal symptoms plus computed tomography (CT) scanning [10]. The exclusion criteria were: (1) emergency surgery was indicated because of co-existing diffuse peritonitis or septic shock when PAL was diagnosed; (2) a traditional drainage tube was not placed during surgery; and (3) patients who refused to take part in the study.
Definition of terms
The American Society of Anesthesiologists (ASA) score was based on a scale of 1–5 [11]: 1, without systemic disease; 2, mild systemic disease; 3, severe systemic disease; 4, severe systemic disease that was a constant threat to life; and 5, moribund patients not expected to survive without surgery. Sepsis was defined as infection plus systemic manifestations of inflammation [12]. Spontaneous closure of PAL included complete spontaneous closure and partial spontaneous closure. Complete spontaneous closure meant that all PALs closed spontaneously, whereas partial spontaneous closure meant that part but not all of the PAL closed spontaneously, both of which were considered successful.
Study design
From January 2010 to December 2016, patients with PAL in the Affiliated Hospital of Inner Mongolia Medical University and Jinling Hospital were enrolled in this study. The patients were divided into the traditional drainage tube group and the FTB group using the table of random numbers (Fig. 2). The end point of follow-up was PAL healing or patient mortality. The entire process was non-blinded for both doctors and patients. Patient demographic data, including gender, age, body mass index (BMI), smoking status, alcohol consumption, comorbidities, etiologies, surgical types, surgical location, anastomotic number, ASA score, intra-operative blood loss, and operation duration as well as the time from surgery to PAL were collected. Patients in the FTB group received additional treatment with FTBs immediately after the diagnosis of PAL, whereas patients in the traditional drainage tube group only underwent traditional drainage tube placement. Other treatments, such as antibiotic therapy and nutritional support, were similar between the two groups. Indicators of inflammation (body temperature [BT]; white blood cell count [WBC]; C-reactive protein [CRP]) were recorded at pre-determined times. Moreover, clinical prognosis in terms of spontaneous closure, intra-peritoneal abscess, diffuse peritonitis, sepsis, duration of antibacterial agents, time to enteral nutrition, hospital stay, and expenses was compared between the two groups. Patients not achieving complete spontaneous closure received definitive surgery for their intestinal fistula after two to three months (this time period was required for fistula formation and pre-operative preparations). We also analyzed the one-month survival ratios in both groups. This study was approved by the Institutional Review Board of the Affiliated Hospital of Inner Mongolia Medical University and Jinling Hospital and was in compliance with the Helsinki Declaration. Informed consent was obtained from all participants.

The flow chart of this pilot study.
Statistical analysis
Demographic data were analyzed using χ2 test for qualitative variables and a two-sided t-test for quantitative variables. Similarly, the data on clinical outcomes in the two groups were also analyzed using the χ2 test and a two-sided t-test. The one-month survival curves were established using a life table and compared by the Wilcoxon test. SPSS version 17.0 software (SPSS Inc., Chicago, IL) was used to conduct all statistical analyses. Indicators of inflammation after diagnosis of PAL were compared between the two groups using the two-way analysis of variance (ANOVA) test with GraphPad Prism 5 software (GraphPad Software, San Diego, CA). Bonferroni post-tests were further performed to determine statistical differences in indicators of inflammation at each time point.
Results
Sixty eligible patients were enrolled in this study, 30 patients in each group. The demographic data showed no statistical differences (Table 1). The failure rate of FTB placement was zero. In the traditional drainage tube group, 15 patients (50%) experienced tube occlusion, whereas only three patients (10%) experienced occlusion of the FTBs during treatment (Table 2). This may have been caused by continuous irrigation using the FTBs that diluted the enteric contents, particularly in the lower digestive tract where the digested content was concentrated.
Demographic Data of Enrolled Patients
BMI = body mass index; ASA = American Society of Anesthesiologists.
Frequency of Tube Occlusion in Two Groups and Solutions
(—) the fine tube bundles were not unclogged but replaced.
Indicators of inflammation reflect the effects of infection control on PAL [13,14]. Figure 3 shows the trend in these indicators (BT, WBC, and CRP), which decreased after integrated treatment with source control, antibacterial agents, and nutrition management, although BT and WBC were not statistically different between the two groups. The declining trend in CRP was substantially different in the FTB group compared with that in the traditional drainage tube group, especially one, three, and five days after the intervention for PAL. This not only indicated that CRP was a sensitive biomarker of infection control, but also suggested that the FTBs improved the drainage efficiency of enteric contents from the PAL and reduced inflammation.
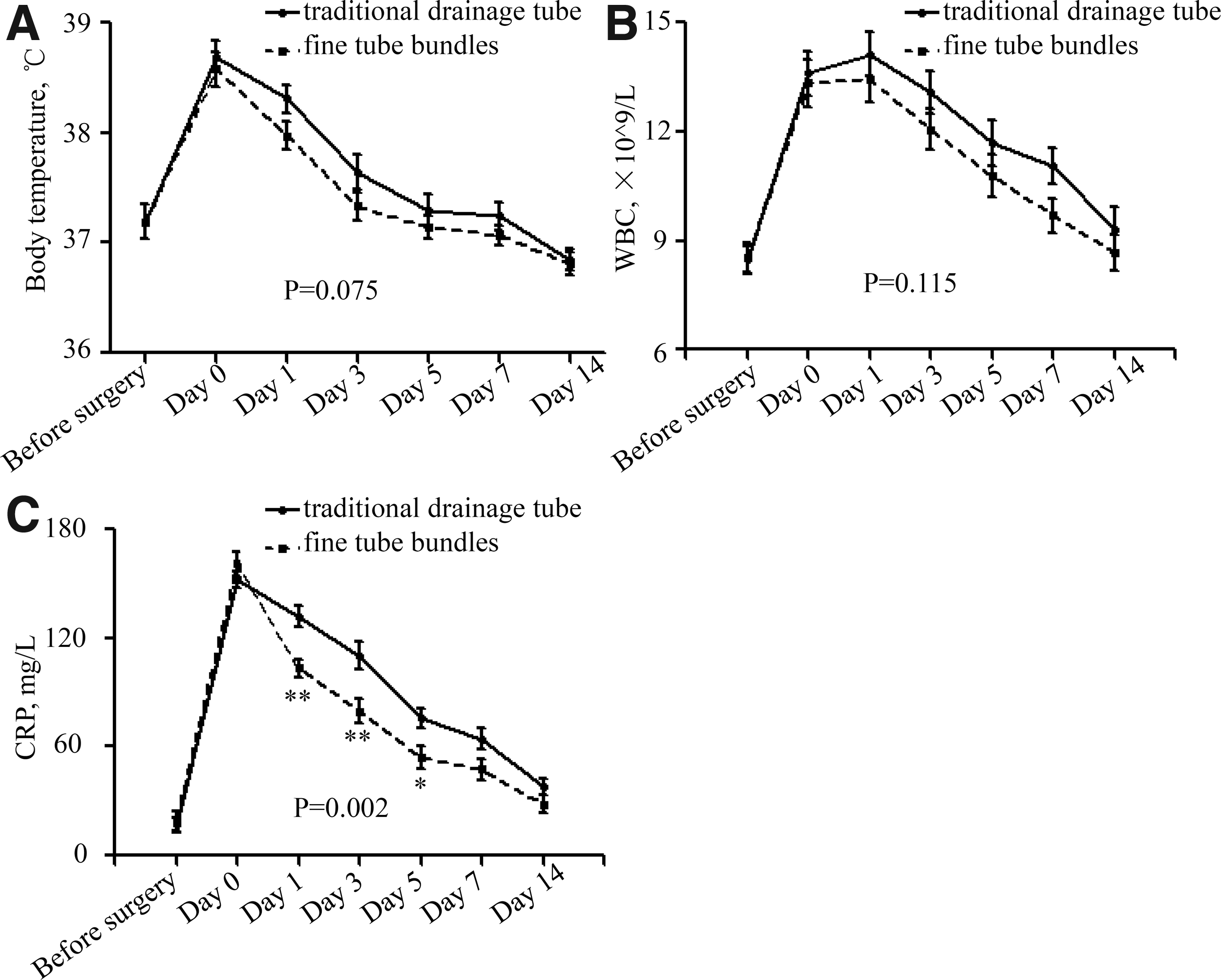
The trends of inflammation indicators before and after application of traditional drainage tubes or traditional drainage tubes combined with FTBs. (
Moreover, the occurrence of intra-peritoneal abscess was less common in the FTB group (Table 3). Other fatal complications such as diffuse peritonitis and sepsis were also reduced, although the differences were not statistically significant in this small sample study. The duration of antibiotic use was shorter and enteral nutrition was administered earlier in the FTB group. Consequently, the one-month mortality rate in the FTB group was lower (Fig. 4), and a higher proportion of patients obtained spontaneous closure after the application of FTBs (Fig. 5). Hence, patients in the FTB group were discharged from hospital earlier and had lower hospitalization costs.
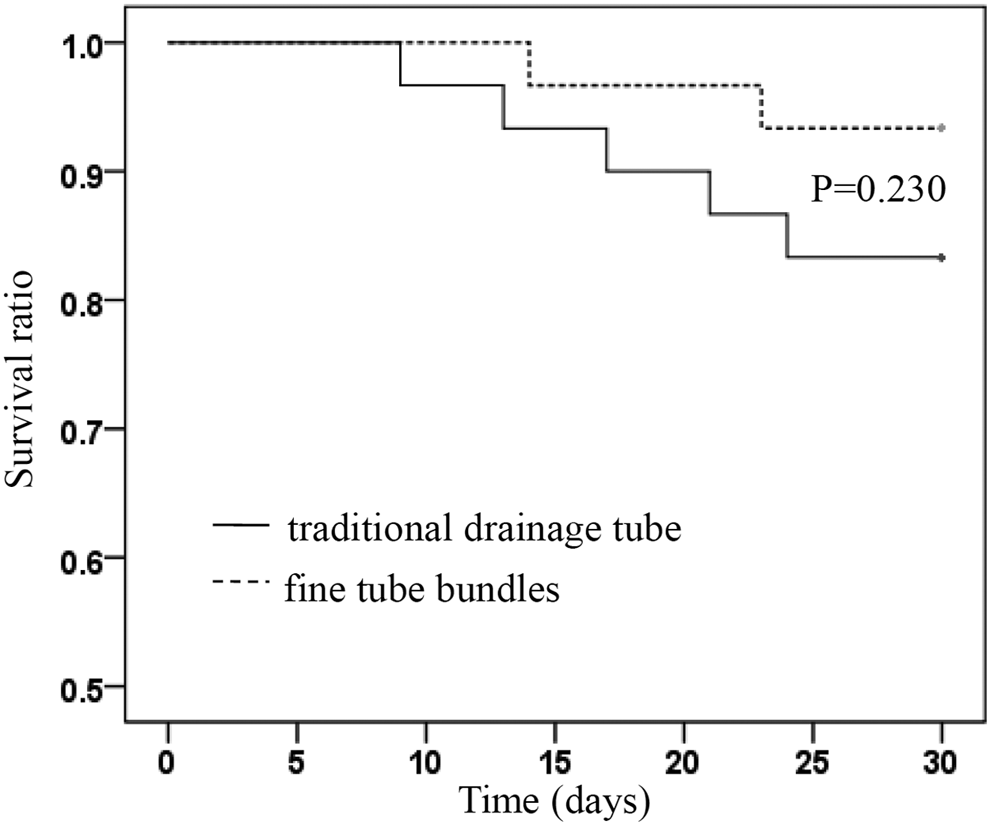
The cumulative survival ratio in the fine tube bundle (FTB) group and in the traditional drainage tube group, respectively.

The cumulative ratio of patients whose post-operative anastomotic leak (PAL) was not closed in the fine tube bundle (FTB) group and in the traditional drainage tube group, respectively.
Clinical Outcomes of Enrolled Patients
Days from diagnosis of PAL to administration of EN.
PAL = post-operative anastomotic leak; EN = enteral nutrition.
Discussion
This study describes a novel active drainage approach and validates its efficacy in improving the clinical outcome of PAL. Compared with a traditional drainage tube, placement of FTBs eliminated the enteric contents by lavage and drainage, thus creating a suitable environment for PAL healing. The safety of FTBs was also considered by adding a sputum suction catheter 6F, which maintained a stable pressure and prevented gastrointestinal damage caused by extra suction pressure. In addition, FTBs reduced the risk of occlusion, and catheter care was convenient. More importantly, it did not produce additional discomfort, therefore, this method was well tolerated by the patients.
The procedures used to manage PAL have not been clearly defined. In 2008, Weidenhagen et al. [15] described a new technique to treat anastomotic leak after anterior resection of the rectum using Endo-SPONGE® (B. Braun Medical Inc., Bethlehem, PA), a vacuum-assisted treatment designed specifically for small leaks. During this procedure, negative pressure was applied to drain the contaminated fluids, thus benefitting PAL healing. Based on this theory, vacuum-assisted techniques were further applied in patients with esophageal, gastric, small bowel, and colorectal leaks [16–18], which were successful in promoting PAL repair without additional surgical procedures. Moreover, in order to treat PAL in patients with Crohn disease, image-guided percutaneous drainage was performed in these patients [19]. The clinical outcomes suggested that this method was effective and safe with low rates of complications and re-operation. The above-mentioned studies illustrate the importance of adequate source control (removing the leaked enteric contents) in the acceleration of PAL repair and their findings were consistent with ours. A traditional drainage tube was prophylactically placed to remove the residual blood and fluids and to drain the leaked enteric contents. In combination with FTBs, this drainage mode was transformed to “active” from “passive” and exhibited satisfying results.
Our study also identified CRP as a highly efficient indicator of inflammation, which reflected therapeutic response to the two drainage methods. In previous studies, CRP was regarded as a useful biomarker in predicting PAL in esophago-gastric surgery [20] and colorectal surgery [21,22]. After the diagnosis of PAL, the decline in CRP also reflected adequate source control and favorable clinical outcomes and had more value than other indicators such as BT and WBC. Other infection biomarkers such as interleukin (IL)-6 and procalcitonin were not measured in the present study, which have been reported to have higher sensitivity and specificity [23,24].
There are some limitations to this study. First, the sample size was small, thus, some of the parameters measured did not show statistical differences. Larger randomized multi-center studies are required to further confirm our findings. Second, because anatomic factors such as tension and ischemia [25] can influence the occurrence of PAL, patients may need to be sub-grouped according to anastomotic locations during follow-up.
Conclusion
Fine tube bundles are a feasible and useful approach to achieve active drainage. The application of FTBs may further promote spontaneous closure of PAL and reduce the formation of intra-peritoneal abscess. This approach showed a tendency to reduce the duration of antibiotic use and hospitalization costs. Therefore, FTBs are worthy of further investigation and promotion.
Footnotes
Acknowledgments
Feng Wang and Ren Jianan designed the study. Feng Wang, Gefei Wang, and Xiuwen Wu collected the patient data. Feng Wang and Zhiwu Hong analyzed the data and wrote the manuscript. Huajian Ren monitored the study and provided advice on research. Feng Wang revised this manuscript.
This research was funded by the National Natural Science Foundation of China (grant no. 81571881) and Key Project of Jiangsu Social Development (grant no. BE2016752).
Author Disclosure Statement
We declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.