
Abstract
Abstract
Background:
Routine screening and treatment for pre-operative asymptomatic bacteriuria (ASB) before joint arthroplasty are controversial. This systematic review and meta-analysis aimed to evaluate the impact of ASB and other bacterial colonization markers (BCM) observed in abnormal urine analyses, such as positive nitrites, leukocyturia, or positive leukocyte esterase in the risk of surgical site infections (SSIs) of joint arthroplasty patients.
Methods:
Studies published between 1970 and 2017 that reported data on SSI and prosthetic joint infection (PJI) in patients after joint arthroplasty of the hip, knee, or shoulder with pre-operative ASB or BCM were included. A meta-analysis with random effect model was performed.
Results:
Eleven studies were included (29,371 patients and 35,323 joints). The main procedures were total hip replacements (53.3%) and the mean follow-up period was 21.5 months, with 12 months being the minimum time of follow-up. A total of 2,400 cases (9.5%) reported pre-operative BCM (15%) or ASB (85%). The proportion of SSI was higher in patients with ASB (2.3% vs. 1.1%) (p < 0.001) and was related to a higher risk of SSI (odds ratio [OR] 2.89; 95% confidence interval [CI] 1.36–6.17), however, in only six cases (12.7%) was the SSI micro-organism correlated with the urine culture. Finally, antibiotic treatment for ASB did not reduce the SSI risk (OR = 0.82; 95% CI 0.34–1.97).
Conclusions:
Asymptomatic bacteriuria represent a relatively common finding among these patients and is related to a higher risk of SSI. However, the poor microbiologic correlation suggests that ASB could represent a surrogate marker for other conditions correlated with bacterial infection. Therefore, systematic urinalysis screening should be discouraged, whereas a complete risk assessment that considers comorbidities and past medical history should be promoted.
S
A noteworthy risk factor might be asymptomatic bacteriuria (ASB), which refers to the presence of true bacteriuria without any signs and symptoms of urinary tract infection. It is more common in women and the prevalence increases with age. At least 20% of healthy women over 80 years are affected. Furthermore, it is present in 4%–19% of patients who undergo arthroplasty [4–6]. Asymptomatic bacteriuria theoretically may act as a potential reservoir of pathogens that increases patient morbidity [1]. The relation between urinary tract infection and prosthetic joint infection was first described in 1970 by orthopedic surgeons, however, the real existence of this relation has become a controversial issue [7]. Also, a variety of antibiotic agents are used for this condition, and there is substantial bacterial resistance to these drugs occurring worldwide [2].
Considering the potential harm of unnecessary antibiotic use and the clinical and economic impact of this practice, we performed a systematic literature review to evaluate the association between ASB or other potential bacterial colonization markers (BCM) and SSI or PJI, also analyzing the benefit/harm of treating this condition.
Materials and Methods
The present systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Statement and the Cochrane Handbook for meta-analyses and systematic reviews.
Eligibility criteria
Eligible studies corresponded to randomized controlled trials, cohorts, and case control studies that evaluated the risk of post-operative SSIs, as prosthetic joint infection, in patients who underwent joint arthroplasty of the knee, hip, or shoulder with a pre-operative report of ASB by urine culture (UC). This was defined as the isolation of a specific quantitative bacterial count (≥105 CFU/mL) in an appropriately collected urine sample obtained from a person without symptoms or signs attributable to a urinary tract infection (UTI) or any BCM defined as the following alterations in the urinalysis (UA): leukocyturia (measured in number of leukocytes per field), positive leukocyte esterase, and positive nitrites in the absence of certain features that may suggest contamination of the sample (large number of epithelial cells or quantitative bacterial counts ≥105 CFU/mL with two or more micro-organisms present). Patients included in the studies had to be followed for at least one year after the surgical procedure. Also, the studies included had to be available on full text and have been published after January 1, 1970 in English, Spanish, or Portuguese.
Search strategy
The literature search was performed by two authors using Embase, EBSCOHost, MEDLINE, PubMed, the Cochrane Central Register of Controlled Trials, Scielo, and LILACS. The search algorithm used was the following:
(asymptomatic bacteriuria OR bacteriuria OR asymptomatic leukocyturia OR urine analysis OR urinalysis); (surgery OR prosthetic OR prosthesis OR orthopedic OR traumatology OR joint infection OR arthroplasty OR prosthesis-related infections OR prosthetic joint infection OR surgical site infection OR surgical infection); 1 AND 2; Results filtered to include only articles published after January 1, 1970; Results filtered to include only articles written in English, Spanish, or Portuguese; Repeated results were excluded.
Moreover, an additional search was performed in the Cochrane Library, grey literature (as repositories of university theses), and the references of the evaluated articles to include references that could have been overlooked in the search.
Study selection and data collection
The procedure for selection of each reviewer started with the title review, excluding those without any correlation with the objective of the study. Then, studies were classified as eligible, unclear, and unfit according to the fit of the eligibility criteria. Eligible included those that fulfilled all the inclusion criteria; unclear included those whose title and abstract appeared to be in accordance with the study objective but a full-text review was necessary to ensure its feasibility to be included; and the unfit included those not related to the objectives of the study. Duplicates were removed and those articles marked as eligible or unclear were selected for full-text review. The two reviewers then compared their results, resolving the differences in consensus with the supervision of a third author.
Quality appraisal and risk of bias
The quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS), which evaluates the study characteristics in the selection, comparability, and outcome/exposure domains, classifying them as having good, fair, or poor quality according to the number of stars achieved in each one.
Statistical methods
For outcomes with suitable data for combination, results were meta-analyzed using Review Manager 5.3 (Nordic Cochrane Center, Cochrane Collaboration 2009, Copenhagen, Denmark). For the risk of post-operative infection regarding the UA/UC characteristics, the odds ratio (OR) was calculated using a random effects model. An analysis per joint arthroplasty location was also performed. Heterogeneity of the study results was measured with the I2 statistic, defining low heterogeneity as less than 25%, moderate as 25%–50%, and high as more than 75%.
The results of the meta-analysis were illustrated using forest plots with 95% confidence intervals for each study and a cumulative weighted mean effect for all included ones. Finally, other inconsistent variables reported were described as a systematic review.
Results
Study selection
As shown in Figure 1, 1,022 studies were obtained from the initial search of the literature, both in the databases and in the grey literature. After the initial review of the titles and abstracts was performed, 1001 were discarded because of being classified as unfit. The remaining 21 were then evaluated in full text, being finally included 11 studies the results of which are presented below (Table 1).
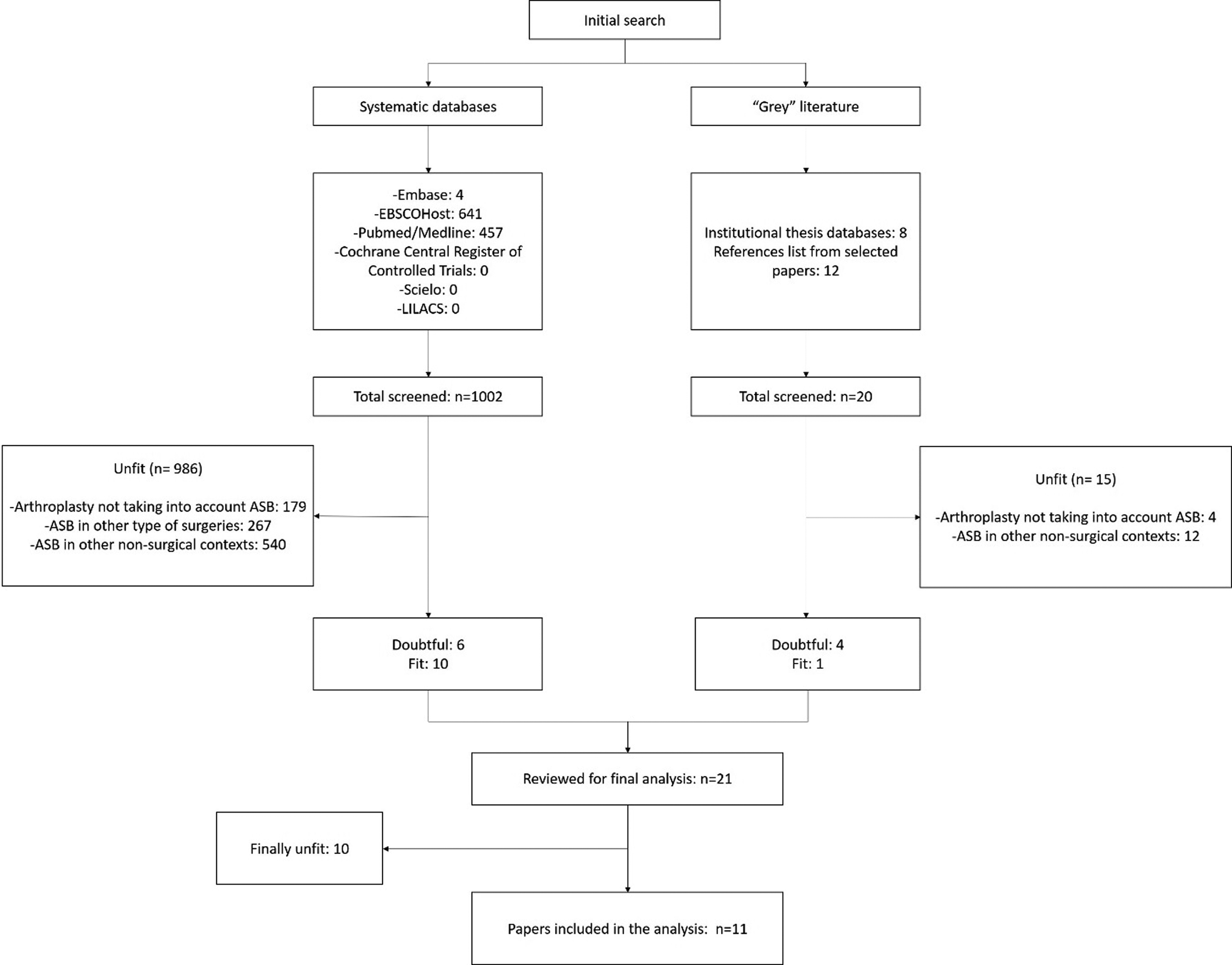
Flow chart of study selection.
Characteristics of the Studies that Evaluated Surgical Site Infections in Patients Undergoing Arthroplasty with and without Urinary Tract Colonization Markers
ASB = asymptomatic bacteriuria; PJI = prosthetic joint infection; UA = urinalysis; UC = urine culture; THA = total hip arthroplasty; HHA = hip hemiarthroplasty; TKA = total knee arthroplasty; THR = total hip replacement; TKR = total knee replacement; THPR = total hip prosthesis replacement; TKPR = total knee prosthesis replacement; IVA = instrumented vertebral arthrodesis; ASL = asymptomatic leukocyturia; POL = pre-operative leukocyturia, NS = not specified.
Patient baseline characteristics
A total of 29,371 patients and 35,323 joints were included. The individuals were predominantly females (from the studies that provided this information n = 20,468; 64%), with a mean age at the time of procedure of 67.1 years. The surgical procedures performed were mainly hip arthroplasties, with 18,818 cases (53.3%) and knee arthroplasties with 14,978 cases (42.4%). From these, 2,400 reported an abnormality in the UA or UC, with 2,043 having a confirmed ASB and 357 evidence of BCM. Risk of bias assessment for each study is presented in Table 2 [3,8–17].
Application of the Newcastle-Ottawa Scale for the Evaluation of the Methodological Quality of the Included Studies
Two studies evaluated the risk of SSI in patients with an abnormal UA, showing that almost 17.9% (from a total of 1,995) had BCM, findings usually associated with urinary infection. Regarding the infection rate, only 23 patients (1.15%) developed PJI, with only 4 (0.2%) having an abnormal UA, with no uropathogen isolated in the joint culture.
On the other hand, nine studies included patients with an ASB by UC, including 32,164 joints. From these, only 2,043 had a proven ASB, representing a prevalence of 6.3% of the total cases. Moreover, the overall infection proportion was 1.1% (338 cases), with only 47 (0.1%) having evidence of ASB.
Meta-analysis
The analysis was divided according to the type of abnormality (ASB or BCM) and the joint involved. First, an overall analysis was performed including all the patients with UA/UC abnormalities (Fig. 2). Moderate heterogeneity was observed (I2 = 67%), so a random effects model was used to pool the results. Prosthetic joint infection was found to be more common in patients in the ASB group compared with the control group (OR = 2.38; 95% CI, 1.21– 4.67). This effect persisted in the subgroup analysis of studies that evaluated only ASB patients (Fig. 3), in which the risk of SSI was slightly higher for the ASB group compared to those without a UC abnormality (OR 2.89; 95% CI 1.36– 6.17). We also aimed to analyze the studies that evaluated the potential benefit of treating ASB regarding post-operative SSI (Fig. 4). Four of the included articles described separate groups of treated and untreated bacteriuria, showing a higher rate of infection in patients who were treated compared with those who were untreated (1.7% vs. 1.1%, respectively), highlighting the lack of benefit of treating this condition (OR = 0.82; 95% CI 0.34–1.97).

Overall analysis of the risk of surgical site infection (SSI) in patients with pre-operative asymptomatic bacteriuria (ASB) or bacterial colonization markers (BCM).
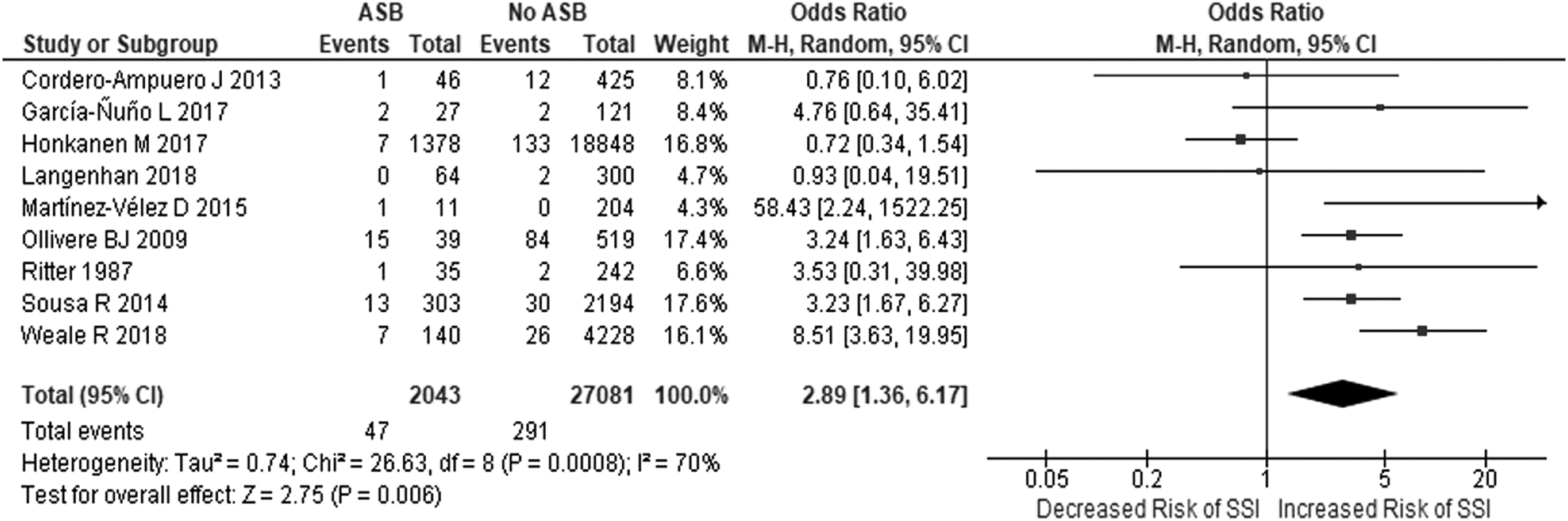
Overall analysis evaluating the risk of surgical site infection (SSI) in patients with pre-operative asymptomatic bacteriuria (ASB).
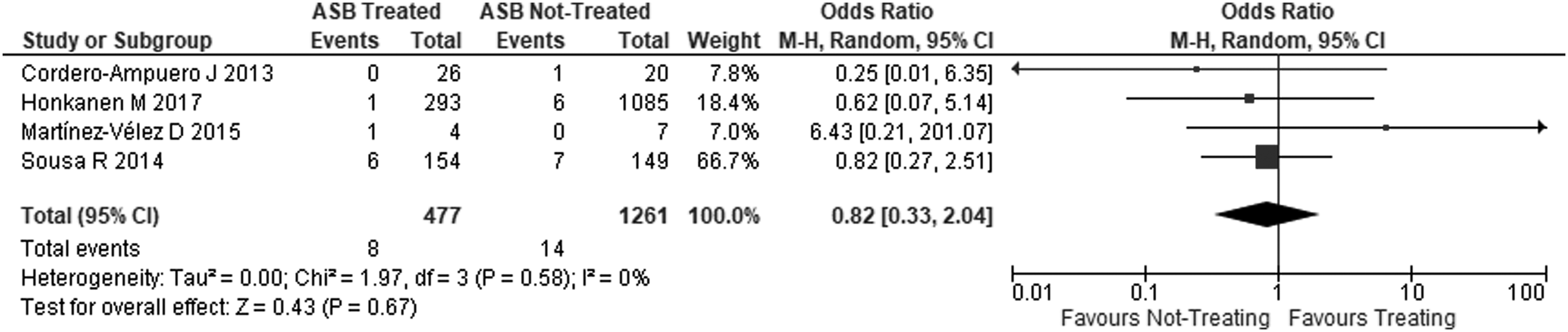
Analysis of the risk of surgical site infection (SSI) in patients with treated versus untreated pre-operative asymptomatic bacteriuria (ASB).
Regarding the correlation between the pathogens isolated in the pre-operative UC and those isolated in the SSI culture (when available), we found few matches. The same micro-organism was found in both samples in only six cases (12.7%) from the total of 47 patients with ASB and an SSI. The main UC micro-organism was Escherichia coli, whereas the gram-positive cocci were the predominant pathogens in the SSI cultures. The cases in which the information of both pathogens was reported are summarized in Table 3.
Correlation between the Urine Culture and the Surgical Site Infection Isolated Pathogens
NS = not specified; UC = urine culture.
Sensitivity analysis
A sensitivity analysis was performed to evaluate the robustness of the study results. For this purpose, each study was omitted one at a time of the analysis, observing the changes in the overall result. Unfortunately, after omitting the study of Ollivere et al. [13] there were no differences among the groups; therefore, the meta-analysis results were not robust.
Publication bias was assessed. The funnel plot used for this purpose is presented in Figure 5. There was no funnel plot asymmetry for the evaluated association, with the p value for Egger's regression asymmetry test being 0.511, indicating a low risk of publication bias.
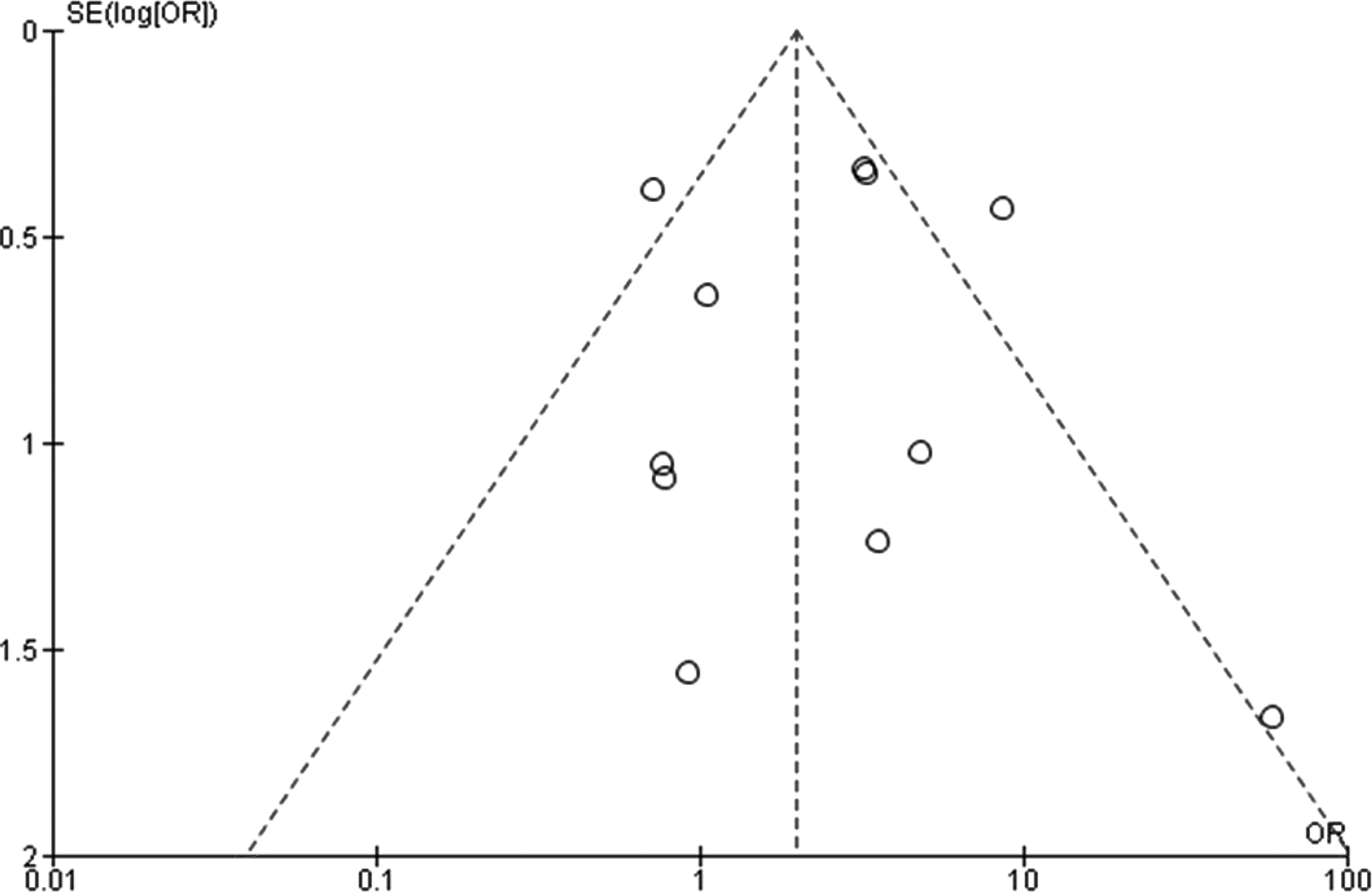
Funnel plot of included studies.
Discussion
Although there are several studies available on this subject, they have different conclusions. Our primary objective is to provide the highest quality conclusion considering the best and latest evidence, especially when including studies with opposite conclusions. Our results are in agreement with those reported by Sousa et al. [3], demonstrating an increased risk of SSI in patients with ASB compared with non-ASB carriers. However, based on poor microbiologic correlation among SSI culture and pre-operative UC (in only 12% of the cases were isolated bacteria the same), we support the hypothesis that ASB is a surrogate marker more than an actual directly related risk factor for SSI. Potential true risk factors that may increase both the SSI and ASB rate are obesity, diabetes mellitus, end-stage renal disease, and female gender, among many others commonly identified [18]. Unfortunately, most of the included studies did not consider these variables as confounding factors when performing the statistical analyses, potentially contributing to the apparent effect of ASB in the rate of SSI. An exception was observed in the study of Sousa et al. [3], which indeed considered these variables for analysis. Therefore, their results cannot be attributed to such factors; thus, there is clear evidence suggesting the existence of other factors, which may increase the risk for both conditions.
We also found lack of benefit in treating patients with ASB pre-operatively, with similar rates of SSI among the treated and untreated groups. An absence of heterogeneity among the studies that evaluated this parameter revealed that even when treating the bacteriuria, the SSI rate would be unaffected, highlighting the need for identifying and focusing on a series of underlying factors during the pre-operative assessment of the patient. In conclusion, ASB could represent a confounding factor for the poorer physiologic status of an individual affected by some sort of immunocompromise, as yet to be determined definitively.
A plausible explanation may lie on a molecular level in toll-like receptors (TLR), which represent a vital component of the initial response against invading micro-organisms by recognizing the pathogen and initiating the inflammatory response to destroy the exogenous threat and promote the tissue repair. In this case, some studies have described TLR–2 and TLR–4 variants as a risk factor for ASB [19,20]. Regarding TLR-2, polymorphism TLR2_G2258A was associated with a decreased lipopeptide-induced signaling, showing an increased risk of ASB in a cross-sectional analysis of women aged between 18 and 49 years (OR 3.44, 95% CI 1.65–7.17). Remarkably, this polymorphism was not associated with a history of UTI or pyelonephritis in the same evaluated cohort [21]. Also, another study performed in 124 children found an association between this polymorphism and the ASB, suggesting that TLR-2 signaling may regulate the establishment of bacteriuria, influencing the susceptibility to UTIs at an early stage [19,22]. On the other hand, TLR as TLR2 are recognized as contributors to the degenerative and destructive process of the arthropathy that may derive from joint infection, reflecting the progression of the infection in the host [23].
Finally, the clinical guidelines have recently considered the available evidence for changing the recommendation of obligatory urinary screening and the management of pre-operative ASB. Some have even stated that urinary screening was not useful before joint replacement, except for patients with a history of frequent urinary infections or symptoms suggesting active infection [24]. For example, the Infectious Diseases Society of America and the National Institute for Health and Care Excellence suggested that patients with ASB do not need corresponding antibiotic treatment, except for pregnant women. However, these recommendations were not explicitly designed for arthroplasty patients [25,26].
Study limitations
There are certain limitations to our study. First, there is no standardized definition for PJI, favoring a lack of uniformity in the selection of patients. Moreover, the small number of patients with ASB and the considerable heterogeneity in follow-up times among included studies were limitations for performing an optimal analysis. As mentioned, few studies considered comorbidities, specifically diabetes mellitus and obesity in their analyses. Also, not all studies randomly assigned the treatment and, in some, specific treatment was unknown. Furthermore, although treatment indication was given, in most studies it was not possible to assess adherence to such therapy by patients. Additionally, treatment effectiveness was not confirmed (using post-treatment/pre-surgery urine culture) in the majority of articles. Finally, there are some identified conditions associated with higher risk of SSI that were not explicitly assessed in any study, namely malnutrition, alcohol consumption, smoking, human immunodeficiency virus (HIV) or hepatitis C infections or warning signs of primary immunodeficiency [18].
Conclusions
The prevalence of ASB among joint arthroplasty patients was not found to be negligible, being related to a possible higher risk of SSI. However, the poor microbiologic correlation and the potential confounding variables not analyzed in the evaluated studies may suggest that ASB could represent a surrogate marker for other conditions correlated with a poorer physiologic status of the immune system. Therefore, systematic UA screening should be discouraged, whereas a complete risk assessment that considers comorbidities and past medical history should be promoted.
Footnotes
Acknowledgments
No external funding was needed for the completion of this study.
Author Disclosure Statement
The authors declare that there are no conflicts of interest relevant to this work. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines. The authors confirm that the approval of an Institutional Review Board or patient consent was not required for this work.