
Abstract
Abstract
Background:
The objective of this study was to determine the clinical and laboratory features affecting mortality in Fournier gangrene.
Patients and Methods:
This retrospective case control study was designed to evaluate patients treated for Fournier gangrene in our center between 2010 and 2018. Those patients were divided into two groups: discharged patients (group 1) and deceased patients (group 2). Comparisons were made regarding clinical and demographic features; leukocyte, neutrophil and lymphocyte count results; neutrophil to lymphocyte ratio (NLR); Fournier's Gangrene Severity Index (FGSI) scores; number of debridements; complications; and mortality rates.
Results:
Twenty-three patients (19 males, 4 females) were evaluated; mean age was 65.91 ± 16.34 years. The most common cause of the disease and comorbidity were perianal abscess (n = 14; 60.9%) and type 1 diabetes mellitus (n = 11; 47.8%), respectively. Escherichia coli was the pathogen identified most often (n = 17; 73.9%). The total mortality rate was 21.7% (n = 5). Neutrophil to lymphocyte ratio, FGSI, number of debridements, and complication rates were higher in group 2 (p < 0.05). There was a substantial difference between the groups regarding perianal abscess in group 1 and rectum cancer in group 2 (p < 0.05).
Conclusion:
In conclusion, it was believed that the mortality rate could be predicted by combining the NLR value with the FGSI score.
F
Because Fournier gangrene is a rare clinical condition, the predisposing factors (such as type 1 diabetes mellitus, alcoholism, uremia, malignancy, and neurologic deficits) and factors affecting mortality have been described in a limited number of studies [3,5]. Furthermore, predictive markers of the mortality rate and prognostic factors have not yet been clearly identified in patients with Fournier gangrene. Therefore, the aim of this retrospective case control study was to address this lack of complex information in literature.
Patients and Methods
Study design and participants
The current study protocol was approved by the local ethics committee. Because the study was retrospective, written informed consent was not required. The study included patients treated for Fournier gangrene between 2010 and 2018. Patients with insufficient medical data were excluded from the study. The patients were separated into two groups as follows: group 1 (discharged patients, n = 18) and group 2 (deceased patients, n = 5)
Data collection
The data were obtained from the patient hospital records. Clinical and demographic features such as age, gender, comorbidities, etiologic factors, length of stay in hospital, platelet (reference range, 150,000–500,000 per microliter), leukocyte (reference range, 4,400–11,300 per microliter), neutrophil (reference range, 1,100–9,600 per microliter), and lymphocyte (reference range, 500–6,000 per microliter) count results, neutrophil to lymphocyte ratio (NLR), mean platelet volume (MPV), Fournier's Gangrene Severity Index (FGSI) score, number of debridements, ostomy requirement, culture test results of purulent material obtained from infected tissue, complications, and mortality rates were recorded.
Statistical analysis
Statistical analyses were applied using the Statistical Package for the Social Sciences (SPSS) version 21.0 software (IBM SPSS Statistics for Windows, version 21.0. monk, NY: IBM Corp., Armonk, NY). Descriptive data were stated as mean or median and standard deviation values. The Mann-Whitney U test and independent samples t-test were used for binary comparisons of continuous variables and the χ2 test for categorical variables. A value of p < 0.05 was accepted as statistically significant.
Results
A retrospective review was made of a total of 28 patients treated for Fournier gangrene; five patients were excluded because of incomplete medical data. Thus, 23 patients were evaluated (19 males and 4 females) with a mean age of 65.91 ± 16.34 years. The most common cause of the disease was perianal abscess (14 patients; 60.9%). The most common comorbid disease was type 1 diabetes mellitus (11 patients; 47.8%). The most frequently isolated pathogen in the wound culture was Escherichia coli (17 patients; 73.9%). The most common post-operative complication was pulmonary embolism (6 patients, 66.66%). Mortality resulting from Fournier gangrene was determined in five patients (21.7%) (Table 1, Fig. 1).
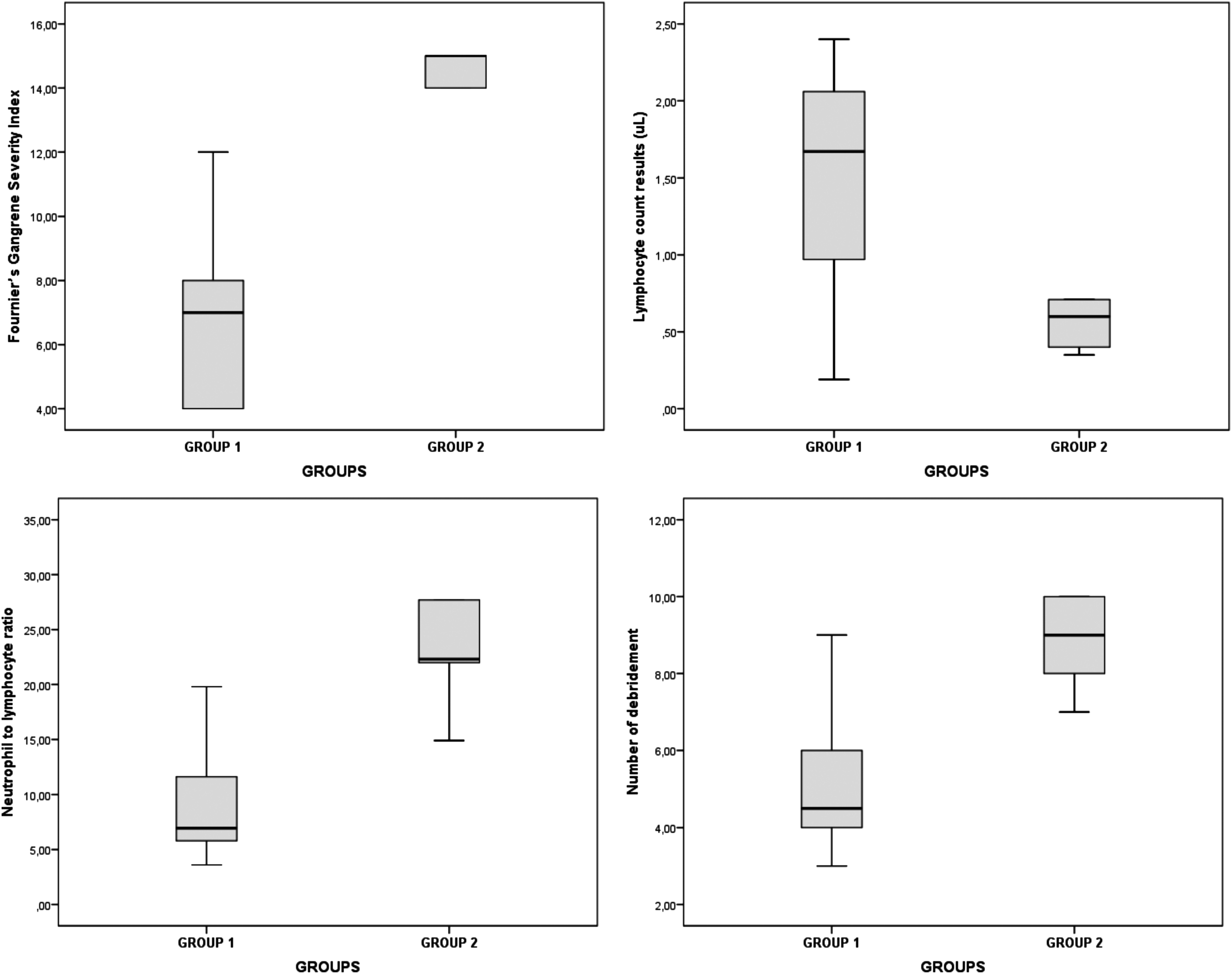
The Fournier's Gangrene Severity Index scores, lymphocyte count, neutrophil to lymphocyte ratio and number of debridements for each group.
The Clinical and Demographic Features of All Participants
TTH = time to hospital (time from symptom onset to hospital admission); DHS = duration of hospital stay; DM = type 1 diabetes mellitus; COPD = chronic obstructive pulmonary disease; CAD = coronary artery disease; Coag (-) staph = coagulase-negative staphylococci.
The NLR (p = 0.003), FGSI (p < 0.001), number of debridements (p = 0.001), complication rate (p = 0.003) values, and the duration of hospital stay (p = 0.020) were found to be higher in group 2 patients, and the lymphocyte count results were higher in group 1 patients (p = 0.016). In the analysis of etiologic factors for the development of Fournier gangrene, there was a difference between the groups regarding perianal abscess in group 1 and rectum carcinoma in group 2 (p = 0.030) (Table 2).
The Neutrophil to Lymphocyte Ratio, Fournier's Gangrene Severity Index, Number of Debridements, Complication Rate and the Duration of Hospital Stay Were Found To Be High in Group 2 Patients and Lymphocyte Count Results Were High in Group 1 Patients
Mann-Whitney U test and independent samples t test (p < 0.05).
Mean ± standard deviation.
Discussion
Fournier gangrene develops as a result of multiple micro-organisms creating severe infection and extensive tissue damage. Therefore, Fournier gangrene necessitates urgent and aggressive surgical treatment [6,7]. In addition to surgical therapy, electrolyte regulation, fluid resuscitation, and broad-spectrum antibiotic agents are of paramount importance [8]. The recommended empirical antibiotic therapy comprises gentamicin, clindamycin, and ampicillin-sulbactam or third-generation cephalosporin, and the specific antibiotic therapy should be given according to the culture results [9]. Escherichia coli has been found to be the most frequently isolated factor in many studies [10,11]. In the present study, perianal abscess, scrotal abscess, and pressure ulcers were most common etiologic factors and Escherichia coli (73.9%), which was probably the underlying causes of Fournier gangrene, was the most commonly detected pathogenic agent.
Management of Fournier gangrene is important to reduce mortality rates. Because the clinical presentation of Fournier gangrene is quite heterogeneous, determination of the degree of Fournier gangrene is the first step of the treatment regimen. In this context, the FGSI, a valid and reliable scoring system, is used commonly in clinical practice [12–14]. In the present study, the FGSI score, NLR, and number of debridements were found to be high whereas lymphocyte count values were low in Group g patients and these findings could be interpreted as a sign of severe infection. Therefore, mortality could be said to be strongly related to the low lymphocyte count values and the high NLR. From these results, it was concluded that in the deceased patients group, the immunologic and cellular inflammatory reactions could not save the patients from the severity of the microbiologic toxins effectively. Furthermore, it was observed that the number of debridements did not improve the mortality rate. Because the lymphocyte count values were low in group 2 patients, this suggests that the cellular immunologic responses (such as T-helper lymphocyte response, natural killer cell function, etc.) may be suppressed by some factors (such as comorbid diseases, genetical abnormalities, etc.) in these patients. However, these hypotheses could not be discussed in this study because of insufficient data. Therefore, there is a need for further studies to investigate why this increased inflammatory response is not sufficient in the treatment of these patients. The duration of hospital stay in group 2 was longer than that of group 1 patients, which was attributed to the greater number of debridements and increase in complications.
Although a cutoff value for the predictive use of NLR for mortality could not be determined because of the small sample size, it could be interpreted as a sign of severe infection in these patients. Therefore, it was concluded that further studies analyzing the diagnostic accuracy of NLR in Fournier gangrene are required to confirm these results, although the higher NLR value was statistically significant in the sample size of this study. In literature, overall mortality rates have been reported to be 20% in patients with Fournier gangrene despite surgical debridement in all patients in addition to supportive care such as hyperbaric oxygen therapy. In those studies, type 1 diabetes mellitus was the most common predisposing factor and the authors suggested that the treatment of type 1 diabetes mellitus has an effect on mortality and prognosis [14–16]. The results of the current study, which are consistent with literature, indicated that Fournier gangrene has a high mortality rate (21.7%) despite aggressive medical and surgical treatment regimens. Nevertheless, comorbid disease, especially type 1 diabetes mellitus, was not determined as a predisposing factor for the mortality rate. Therefore, these findings strongly indicate a need for detailed investigation of the physiopathogenesis of Fournier gangrene in future studies.
Limitations
There are some important limitations to this study, namely the small sample size and retrospective design. Another limitation was the lack of regression analyses to determine the risk factors.
Conclusion
In light of the results of this study, it was concluded that the mortality rate of Fournier's gangrene could be predicted by combining the NLR value with the FGSI index. However, these findings need to be confirmed by further studies.
Footnotes
Acknowledgments
The preliminary results of this study were presented at the 21st National Surgery Congress, Antalya, Turkey, in 2018.
F.P. and O.A. designed the study and analyzed the data. F.P. and O.A. wrote the article.
Author Disclosure Statement
The authors have no conflict of interests to declare.