
Abstract
Abstract
Background:
With the prospect of antibiotic failure in the post-antibiotic era, strategies that prevent surgical site infection (SSI) are increasingly important. Current literature suggests that incisional Negative Pressure Wound Therapy (iNWPT) is a promising intervention.
Methods:
Based on published literature regarding iNPWT, its mechanisms of action, and clinical results, a narrative summary was built, including both the experimental as well as the clinical literature.
Results:
The experimental literature indicates that iNPWT provides a barrier against external contamination before re-epithelialization, increases blood flow and lymphatic clearance, and reduces edema. Meta-analyses of randomized studies indicate that iNWPT is effective in reducing SSI. We did not identify studies that assessed bacterial clearance during iNPWT in contaminated surgical sites, nor did we identify clinical studies that specified they omitted concomitant antibiotic prophylaxis.
Conclusions:
Moderate quality evidence indicates that iNWPT reduces SSI, although data without the concomitant use of antibiotic prophylaxis are lacking. The iNPWT is likely effective as a result of its barrier function and optimization of the surgical site micro-environment. For now, iNPWT is recommended for incorporation in SSI prevention bundles. The iNPWT as a substitute for antibiotic prophylaxis is not recommended currently. Further reduction of SSI by iNPWT will lessen the need for therapeutic use of antibiotic agents.
T
Conventionally, surgeons close incisional surgical sites with sutures or staples [14]. After most types of surgical procedures, it is standard practice to cover primarily closed surgical sites with a simple gauze-based dressing [15]. Many types of dressings are available, ranging from simple to more complex dressings. The latter may have absorbent or antibiotic properties, and some may interact with the wound to improve healing [15]. Nevertheless, currently there is no convincing evidence to suggest any of these types of dressings prevent SSI [16].
Introduction of Incisional Negative Pressure Wound Therapy (iNPWT)
Although NPWT has been used since the 1990s as a chronic and acute surgical site treatment [17,18], since 2001, NPWT is also being applied pre-emptively to surgical incisional sites [19]. This is often referred to as either iNPWT, prophylactic NPWT (pNPWT), or closed-incision management (CIM). On regular skin closure, the NPWT dressing is applied to the surgical site under sterile conditions, after which a continuous amount of sub-atmospheric pressure is applied for several post-operative days. Most studies report use of −80 or −125 mm Hg of sub-atmospheric pressure, for a length of five to seven days after operation [20]. Although the first reports used materials that are readily available in a regular hospital, several commercially available and disposable products that have been developed specifically for iNPWT currently areavailable [21].
Incisional Healing and SSI Pathophysiology
Surgical incisions disrupt the cutaneous epithelial layer that normally prevents bacteria from entering the body [22]. In healthy individuals, it takes at least three to six days for re-epithelialization to restore the barrier function of the skin [23]. Risk factors such as diabetes or contaminated surgical fields such as related to abdominal surgical procedures with intestinal anastomoses result in prolonged re-epithelialization [22]. In contrast to what the term primary closure implies, incisions are actually open surgical sites for a considerable time during which bacteria such as resident skin flora are free to colonize the surgical site [24]. Ostomy creation near an incision is a common procedure that superimposes a risk of colonization with fecal pathogens [25].
Post-operative colonization of surgical sites is associated with increased risk of SSI [24,26,27]. Moreover, biofilms can form within days [28]. In surgical sites, the period to re-epithelialization is therefore critical, because biofilms may further impede re-epithelialization and are difficult to treat without debridement [29]. This is of special importance in surgical procedures with implants, such as orthopedic or breast surgery [30]. Up to 5%–10% of implant-based breast reconstructions currently is reported to fail as a result of late SSI [31–33]. Whether a SSI develops is determined by the interplay of the following factors: The extent of inoculation of the surgical site, the virulence of the involved pathogens, the surgical site micro-environment, and the quality of the host defense [34,35]. Because some of these factors are modifiable, they provide windows of opportunity for strategies aimed to prevent SSI.
Barrier function of NPWT
Because of its non-occlusive nature, gauze and gauze-based dressings are permeable to bacteria [36]. An in vitro study by Lawrence [37] has demonstrated that bacteria can pass through up to 64 layers of dry gauze. In contrast, iNPWT uses a foil that is impermeable to pathogens. Although we did not identify a published article on this subject, the Food and Drug Administration summary report of one of the commercially available iNPWT devices mentions that the ability of the dressing to serve as a barrier against external contamination was verified through a Phi-X 174 bacteriophage challenge [38]. This test indicated that there was no pathogen penetration through the foil [38]. Moreover, the sub-atmospheric pressure results in close approximation of the foil to several centimeters of skin, while also approximating both incisional edges. Anything that passes through the incision is also directed away from the surgical site as a result of the direction of suction (Fig. 1).
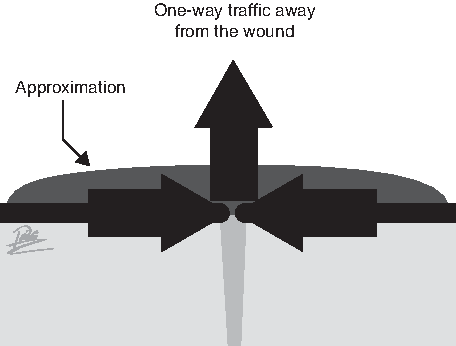
Approximation and one-way traffic through the incision as a result of suction.
Incisional NWPT thus acts as a barrier against external contamination in several ways (Fig. 2). This is in line with the clinical results of Grauhan et al. [39], who have found that iNPWT resulted in a significant reduction of SSI from (gram-positive) skin flora after cardiac surgical procedures in obese individuals (1/75 vs. 10/75, p = 0.009). Moreover, because an iNPWT dressing commonly is left in place for 5–7 days [20], less dressing changes [40] and bedside examinations take place, further decreasing the exposure of the surgical site to potential colonization.
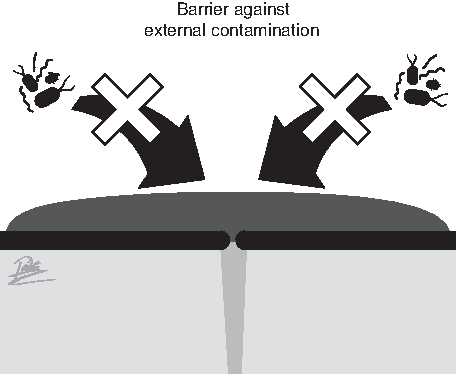
Barrier function of an incisional Negative Pressure Wound Therapy dressing before re-epithelialization.
Seroma and hematoma reduction
Seroma [41] and hematoma [42,43] formation is associated with an increased risk of SSI development. In a porcine incisional surgical site model with underlying dead space, investigators have weighted en bloc resections of these surgical sites before and after removing clot/hematoma/seroma contents and have found that iNPWT resulted in an average seroma reduction of 25 ± 8 g of clot/hematoma/seroma content (p = 0.002) [44]. Moreover, they introduce several unique isotope-labeled nanospheres into each subcutaneous dead space that can only be cleared by the lymphatic system because of their size. Because each incision has been supplied with a specific combination of isotopes, they can investigate the lymphatic clearance of specific incisions. Subsequently, they have quantified the nanospheres in lymph nodes and organs. Their results indicate that incisions treated with iNWPT display more lymphatic clearance than controls (Fig. 3) [44].
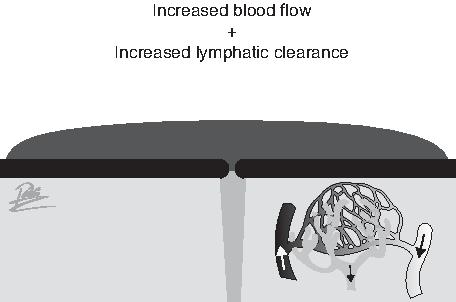
Increased blood flow and lymphatic clearance with incisional Negative Pressure Wound Therapy.
This is concordance with several studies that have assessed seroma volume with ultrasound. Pachowsky et al. [45] report a significant seroma reduction with iNPWT at post-operative day 10 (5.08 ± 5.11 mL vs. 1.97 ± 3.21 mL, p = 0.021). Others have also assessed seroma volume with ultrasound and have found that iNPWT results in a reduced seroma volume at post-operative day five (1.8 mL vs. 0 mL, p = 0.0007) and 10 (1.6 mL vs. 0.5 mL, p = 0.024) [46]. Similarly, a significant reduction of 0.257 ± 0.75 mL versus 3.995 ± 5.01 mL has been demonstrated [47]. Meeker et al. [48] have assessed hematoma formation by using cross-sectional photographs of strips of en bloc surgical site resections in a porcine model and reported significantly less hematoma formation with iNPWT-treated wounds (1.31 ± 1.7 cm2 vs. 0.937 ± 0.54 cm2, p < 0.001).
A previous meta-analysis of randomized hip arthroplasty studies reported a significant seroma reduction with iNWPT (relative risk [RR] 0.48, 95% confidence interval [CI] 0.27–0.84, two studies with 40 patients in total) [49]. We updated meta-analyses and identified 11 observational studies (from nine articles [50–59]) that reported a decreased incidence of seroma with iNPWT, whereas six studies (from five articles [57,60–64]) reported no effect. Taken together, these observational studies indicate a significant seroma reduction with iNPWT (odds ratio [OR] 0.44; 95% CI 0.23–0.86; p = 0.02). We also found four randomized clinical trials (RCTs) [45,65–67], of which two reported decreased seroma incidence with iNWPT [45, 66]. Taken together these studies suggest that iNWPT is associated with a non-significant reduction of seroma (OR 0.67; 95% CI 0.15, 3.04; p = 0.61). We identified eight observational studies reported in seven articles that show a decreased incidence of hematoma with iNPWT.[52,53,57,60,61,63,64] Two studies did not report an effect.[51,68] Taken together, these studies indicate that iNPWT results in a nearly statistical significant reduction of hematoma (OR 0.49; 95% CI 0.23, 1.03; p = 0.06).
We identified three RCTs [65–67], of which one reported an effect [67], and two did not [65,66]. Pooling of the three randomized trials did not display a clear effect on hematoma formation (OR 0.88; 95% CI 0.07,11.03; p = 0.92) [65–67]. An overview of the updated meta-analyses is presented in Table 1.
Summary of Updated Meta-Analyses of Incisional Negative Pressure Wound Therapy versus Standard Care
iNPWT = incisional Negative Pressure Wound Therapy; SSI = surgical site infection; RCTs = randomized controlled trials; WD = wound dehiscence; obs = observational studies. Updated up to December 15, 2017.
Edema reduction
Excessive accumulation of interstitial fluid is generally viewed as detrimental to tissue function because of the increased diffusion distance for oxygen [69]. Because oxygen is essential for bacterial clearance [70,71], edema is thought to impair resilience against infection [72]. In a randomized study, Perry et al. [73] have investigated the influence of iNWPT versus conventional dressings on post-operative edema in a veterinary clinic that treats dogs and cats with limb fractures. In all limbs of the control group, circumference increased as a result of post-operative edema, whereas limb circumference of extremities managed with iNPWT was significantly reduced. This suggests that iNPWT is effective at reducing edema, which plausibly increases tissue oxygenation and thereby possibly bacterial clearance. We did not identify studies that assessed the influence of iNPWT on edema in humans.
Effect of iNPWT on perfusion and necrosis
Adequate perfusion of the surgical site micro-environment is an important contributory factor to the resilience of a surgical site against infection [70,71]. Knighton et al. [70,74,75] have assessed the effect of increased oxygenation on infection resilience compared with antibiotic prophylaxis in animal models, where they demonstrated that improved tissue oxygenation was as effective as antibiotic prophylaxis. Meta-analysis of peri-operative administration of 80% FiO2 versus 30%–35% FiO2 also indicates that improved oxygenation increases SSI resilience [76].
Moreover, adequate perfusion is essential for proliferative surgical site healing to develop [77–79]. Already in the first animal study on NPWT, Morykwas et al. [18] have shown that the cutaneous application of NPWT onto ischemic skin flaps resulted in a significant reduction of cutaneous necrosis in their porcine model. Correspondingly, cutaneous application of NPWT results in a perfusion increase when applied to intact skin of healthy volunteers [80]. Moreover, iNWPT results in significantly increased perfusion at post-operative days four, seven, and 21, as measured with laser Doppler perfusion imaging in a porcine incisional wound model [81]. This is in concordance with other clinical studies showing that iNPWT results in a significant perfusion increase at post-operative days four [82] and five [83].
We did not identify studies that assessed bacterial clearance during iNWPT in contaminated surgical sites. We did not identify a previous meta-analysis that assessed skin necrosis as an outcome. Yet, we identified five observational comparative studies that assessed the occurrence of skin necrosis with iNPWT, indicating a non-significant reduction of skin necrosis (OR 0.50; 95% CI 0.24,1.07; p = 0.07) [51,52,54,61,84]. Three RCTs including 281 patients also indicate a non-significant reduction of skin necrosis associated with iNPWT (OR 0.31; 95% CI 0.06,1.53; p = 0.15) [66,85,86]. Although these meta-analyses are not significant, which may be because of the limited amount of studies and included patients, the direction of the summary estimates is concordant with the notion that iNWPT improves perfusion [51,52,54,61,66,84–86]. An overview of the updated meta-analyses is presented in Table 1.
Wound dehiscence
Wound dehiscence increases the risk of surgical site contamination and therefore increases the risk of infection [87]. The biomechanic effects of iNWPT on incisions have been evaluated with computer models, indicating that iNPWT reduces the amount of lateral stress on incisions [88, 89]. These studies also demonstrate that an increased amount of force is needed to disrupt an incision that is treated with iNPWT [88,89]. Moreover, several animal studies have demonstrated that iNPWT increases the tensile strength of healing incisions [48,81,90]. Together, these findings imply that iNPWT reduces wound dehiscence. A previous meta-analysis of RCTs indicated that iNWPT resulted in a non-significant decrease of wound dehiscence (RR 0.69; 95% 0.47–1.01) [49]. We identified 15 observational studies that indicate that iNPWT significantly reduces the occurrence of wound dehiscence (OR 0.52; 95% CI 0.32,0.85; p = 0.009) [19,39,51–53,57,59,60,62,64,91–94]. We also identified 10 RCTs that indicated that iNPWT reduces wound dehiscence, but here the effect did not reach significance (OR 0.68; 95% CI 0.43,1.07; p = 0.10) [65–67,82,85,86,95–98]. An overview of the updated meta-analyses is presented in Table 1.
SSI
Incisional NPWT acts as a barrier that prevents further inoculation of the surgical site with bacteria before re-epithelialization [38] and improves blood flow [81–83] and lymphatic clearance [44], reduces hematoma, seroma, and edema formation in dead space [44,46–48,73,88,89]. Taken together, iNPWT seems to tilt the balance away from the onset of SSI in several ways, preventing the need for antibiotic agents. This suggests that iNPWT is a favorable prevention strategy to consider, in both present times as well as in a future characterized by even more microbial resistance.
This is substantiated in part by the clinical data available, as assessed in meta-analyses that show that iNPWT reduces SSI. A previous meta-analysis from our research group found six RCTs (562 patients) and 15 observational studies (5010 patients), where both the observational studies (OR 0.30; 95% CI 0.22–0.42) and the RCTs indicated a significant SSI reduction (OR 0.56; 95% CI 0.32–0.96).[20] These results are in concordance with other meta-analyses [49,99]. Results of iNPWT seem consistent for both clean (potentially) contaminated sites, as well as among several types of surgical procedures, including vascular, abdominal, cardiac, and breast operations [20]. This suggests that iNPWT is effective in reducing the risk of SSI in all types of surgical procedures, and likely even in the types of operations where no clinical data exist yet. Because of these results, the World Health Organization recommends to consider iNPWT for all high-risk surgical sites [76].
We updated existing meta-analyses and found 17 RCTs that indicate that iNPWT significantly reduces SSI (OR 0.56; 95% CI 0.38, 0.82; p = 0.003) [65–67,85,86,95–98,100–107]. A forest plot of this meta-analysis is presented in Figure 4. In summary, the RCTs indicate that iNPWT reduces SSI rates from 15% to 9% [65–67,85,86,95–98,100–107]. We also identified 37 observational studies that indicated iNPWT is effective in reducing SSI (OR 0.35; 95% CI 0.20, 0.62; p = 0.0003) [19,39,51–62,84,91–94,108–123]. An overview of the updated meta-analyses is presented in Table 1. We did not identify studies, however, that specified use of iNPWT while omitting antibiotic prophylaxis.
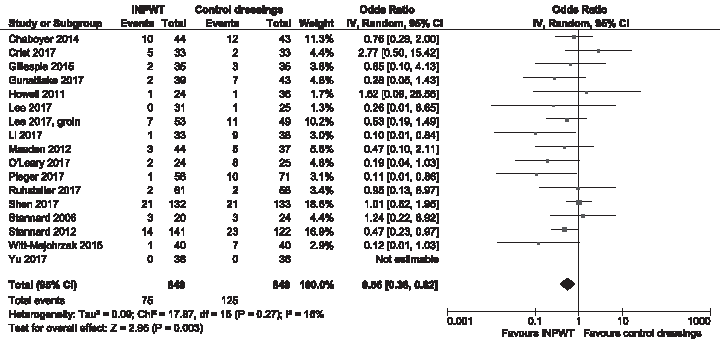
Forest plot of randomized controlled trial meta-analysis with surgical site infection as outcome. iNPWT = incisional Negative Pressure Wound Therapy; CI = confidence interval.
Incisional NPWT as an Alternative to Antibiotic Prophylaxis?
With so little new antibiotic gents being developed [124] and the prospect of antibiotic failure because of microbial resistance [1,2], the proverb “prevention is better than cure” is more relevant than ever. This applies both to the prevention of SSI as well as to the prevention of further microbial resistance. Yet, a review of meta-analyses on antibiotic prophylaxis illustrates that antibiotic prophylaxis is quite effective at reducing SSI [125]. For example, colorectal studies from the 1980s that compared antibiotic prophylaxis with no peri-operative administration of antibiotic agents demonstrate that antibiotic prophylaxis reduces SSI rates from 32%–39% to 2%–9% [126–128]. As mentioned earlier, we did not identify studies that used iNPWT while omitting antibiotic prophylaxis. Although much may have changed since the 1980s and current data suggest iNPWT is an effective SSI prevention strategy, SSI prevention in the post-antibiotic era may prove to be challenging with iNPWT alone; the extent of the reduction of SSI by iNPWT is less than that reported for antibiotic prophylaxis in earlier days.
Current studies also put forward that focusing on single strategies may be of limited advantage for the reduction of SSI [129–131]. This suggests that policy makers should not aim for the implementation of specific prevention strategies, but rather should aim for the implementation of a bundle of several strategies. This is substantiated by reports that suggest that the implementation of bundles results in more favorable SSI rates [132–134]. We propose that iNPWT should be incorporated in such bundles. The decreased incidence of SSI that is likely to result from such interventions will prevent the need for further therapeutic use of antibiotic agents, because SSI are often managed with antibiotic agents. We do not recommend using iNWPT without the concomitant use of antibiotic prophylaxis at this moment.
Cost-effectiveness
Microbial resistance is a costly problem [10–12], as are SSIs [135–137]. As a result of reduced SSI and other surgical site complications, a reduced length of stay, and less dressing changes, iNPWT is likely to save costs in a variety of situations. Cost-effectiveness analyses have assessed iNPWT use for several types of surgical procedures, including primary hip and knee arthroplasty [40], laparotomy in obese/co-morbid individuals [138,139], caesarean section in obese women [140], and general, cardiac, gynecologic, and orthopedic procedures [141]. Use of iNWPT is cost-effective to a range of sensitivity analyses in most cases. A meta-analysis by Strugula et al. [99] demonstrated that iNWPT results in a reduction of length of stay of half a day per treated patient (−0.47 days [95% CI −0.71 to −0.23] p < 0.0001), implying that per two treated patients, one patient can be discharged one day earlier.
Conclusion
Moderate quality evidence indicates that iNWPT reduces SSI. Although data without antibiotic prophylaxis are lacking, it is likely that iNPWT is an effective intervention even in the post-antibiotic era as a result of its barrier function and optimization of the wound micro-environment. For now, iNPWT as a substitute for antibiotic prophylaxis is not recommended, but incorporation of iNPWT in SSI prevention bundles is. Further reduction of SSI by iNPWT will reduce the need for therapeutic use of antibiotic agents.
Footnotes
Acknowledgments
We want to thank our clinical librarian Faridi van Etten-Jamaludin for her help in constructing search strategies.
Part of this work has been presented at the 31st European Annual Congress on Surgical Infections of the Surgical Infection Society Europe, Athens, Greece, June 2018, and includes the literature up to December 15, 2017.
Author Disclosure Statement
This work was supported by an institutional grant from Acelity/KCI, San Antonio, TX.
M.A. Boermeester reports institutional grants from J&J/Ethicon, Acelity/KCI, Allergan/LifeCell, Ipsen, Baxter, Mylan, Bard, and is an advisory board member of J&J/Ethicon, Acelity/KCI, Bard, and Allergan/LifeCell, for research and expertise. P.R. Zwanenburg is a speaker for GD Medical Pharma BV and Hospithera NV (Negative Pressure Wound Therapy distribution companies). For B.T. Tol and F.E.E. de Vries, no competing financial interests exist.