
Abstract
Abstract
Background:
The present study aimed to analyze risk factors and management strategies for organ space infections (OSI) specifically after colonic resections.
Methods:
This was a retrospective analysis of all consecutive colonic resections performed between February 2012 and October 2017 in a single-center quality-improvement project. All OSIs were assessed prospectively by an independent national surveillance program (www.swissnoso.ch) and classified according to the U.S. Centers for Disease Control and Prevention (CDC) criteria (infection involves organ and spaces other than the incision), including anastomotic leaks. Risk factors for OSI were identified by univariable and multivariable analysis.
Results:
The study cohort included 1,263 patients (731 elective and 532 emergency colectomies). One hundred fifty-three patients (12%) were found to have an OSI, which occurred at median POD 8 [interquartile range 4–14]. Treatment strategies consisted of surgical management in 85 cases (56%), percutaneous drainage in 36 cases (24%), and antibiotic treatment alone in 32 patients (21%). Independent risk factors for OSI were emergency surgery (odds ratio [OR] 2.06; 95% confidence interval [CI] 1.35–3.16), operation duration >180 minutes (OR 2.10; 95% CI 1.29–3.40), and open surgery (OR 2.51; 95% CI 1.73–3.65).
Conclusions:
Organ space infections after colonic surgery were more frequent after open emergency surgery and occurred early in the post-operative course. Invasive management was required in 79% of cases.
Current recommendations for the prevention of surgical site infection (SSI) after colonic surgery focus mainly on the prevention of incisional SSI [1,2]. Whereas superficial infections have a modest impact on patients' recovery and may be treated in an out-patient setting by primary care providers, organ space infections (OSIs) usually require invasive management and have a major impact on patients and on healthcare costs [3–5]. Surprisingly, few specific data are available on the prevention and treatment of organ space infections [6,7].
The present study aimed to assess risk factors, incidence, timing, diagnosis, and treatment of OSI after colectomy.
Patients and Methods
Patients were assessed during a five-year prospective surveillance program (February 1, 2012 to October 31, 2017) by monitoring and inclusion in a national registry of colonic resections at Lausanne University Hospital (CHUV). Included were all (unselected) consecutive colonic resections at any location (total, left or sigmoidal, transverse or segmental, right or ileocecal). Stoma-related procedures were excluded (Hartmann reversal, ostomy closure, even when resection was performed) as were rectal resections. Surveillance was performed by a local committee of the Swiss National Infection Surveillance Committee (www.swissnoso.ch). The methodology of this assessment has been described [8]. Patients were treated in a standardized enhanced recovery (ERAS) pathway over the entire inclusion period [9,10].
Demographic items comprised age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) score, and the presence of malignancy, whereas surgical items described were setting (elective versus emergency, defined as surgery within 72 hours after unplanned admission), approach (laparoscopy versus open with converted procedures assigned to laparoscopy according to the intention-to-treat principle), potential additional procedures (defined as further intestinal resections or adhesiolysis for more than one hour), and procedure duration. Two further features were assessed independently by Swissnoso based on surgery reports and chart review: incision class, stratified between II (clean contaminated), III (contaminated), and IV (infectious), and National Nosocomial Infection Surveillance (NNIS) score (0–3), which is composed of the ASA score, incision class, and duration of surgery [11].
Organ space infections were defined according to the U.S. Centers for Disease Control and Prevention (CDC) National Nosocomial Infection Surveillance (NNIS) criteria [11] as any infections involving organs and spaces other than the incision that was opened or manipulated during an operation and at least one of the following:
Organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space; An abscess or other evidence of infection involving the organ/space that was found on direct examination, during re-operation, or by histopathologic or radiologic examination; Diagnosis of organ/space SSI made by a surgeon or attending physician.
Organ space infections were documented prospectively during the index hospitalization. Post-discharge, OSI were tracked and identified by the local Swissnoso committee through telephone calls on POD 30, including review of microbiologic data and treatments performed during re-admissions or emergency visits to other facilities.
Each suspected or diagnosed OSI was validated by a Board-certified infectious disease specialist after a full chart review. Surgeons were not involved in the prospective analysis. Microbiologic evaluation consisted of direct specimen preparation, culture, and susceptibility testing and was performed systematically during re-intervention through either open or percutaneous access.
According to institutional guidelines for all colonic resections, intravenous cefuroxime 1.5 g and metronidazole 500 mg were given within 60 minutes before incision. Alternatives in case of non-tolerance of these drugs were intravenous clindamycin 600 mg and ciprofloxacin 400 mg. Intravenous antibiotic prophylaxis was considered adequate when the following criteria were met: Completion of the infusion within 60 minutes before the surgical incision and peri-operative redosing if indicated [3]. Mechanical bowel preparation in combination with oral antibiotics was not applied.
Treatment strategies were either surgical re-intervention in the operating room under general or local anesthesia, or percutaneous drainage, performed by a Board-certified interventional radiologist, or antibiotic treatment only. All OSI were first treated empirically with co-amoxicillin or piperacillin/tazobactam according to the clinical status of the patient. Antibiotic treatment was subsequently adapted (targeted treatment) according to culture and antibiogram results.
The primary endpoint was the rate of OSI. Secondary endpoints were the timing of OSI diagnosis, treatment modalities, and re-hospitalization rate attributable to OSI.
This study was conducted as part of an institutional quality-improvement project, and data extraction was approved by the Institutional Review Board (CER-VD No. 2016-00991). The study was registered at www.researchregistry.com (UIN researchregistry 4159).
Descriptive statistics for categorical variables are reported as frequency (%), whereas continuous variables are reported as mean (standard deviation [SD]) or median (interquartile range [IQR]). Chi-square testing was used for comparison of categorical variables. All statistical tests were two-sided, and 0.05 indicated significance. Variables with p values ≤0.05 were entered in a multivariable logistic regression (based on a probit regression model) to provide adjusted estimations of the odds ratio (OR). Data analysis was performed with the Statistical Software for the Social Sciences SPSS Advanced Statistics 22 (IBM Software Group, Chicago, IL USA).
Results
A total of 1,263 patients (731 elective and 532 emergency colectomies) constituted the study cohort. Overall, 153 patients (12%) presented OSI, 61 of the total number (8%) after elective surgery and 92 (17%) after emergency resection (p < 0.001). The OSIs were diagnosed at a median POD 8 [IQR 4–14]. Demographic and surgical details are displayed in Table 1.
Demographic and Surgical Details
Intravenous antibiotic prophylaxis was considered adequate when the following criteria were met: infusion within 60 min before the surgical incision and peri-operative redosing if indicated.
Significant p values (<0.05) are displayed in boldface type.
AB = antibiotic; ASA = American Society of Anesthesiologists; BMI = body mass index; IV = intravenous; NNIS = National Nosocomial Infection Surveillance; SD = standard deviation.
The predominant pathogens retrieved from OSI cultures were Escherichia coli (32%), Enterococcus faecalis (27%), and Candida albicans (9%). Other organisms have been found less frequently (Fig. 1). Predominant were gram-negative pathogens (61%), followed by gram-positive (30%) and yeasts (9%). The source of pathogens was the digestive tract in most cases (93%).
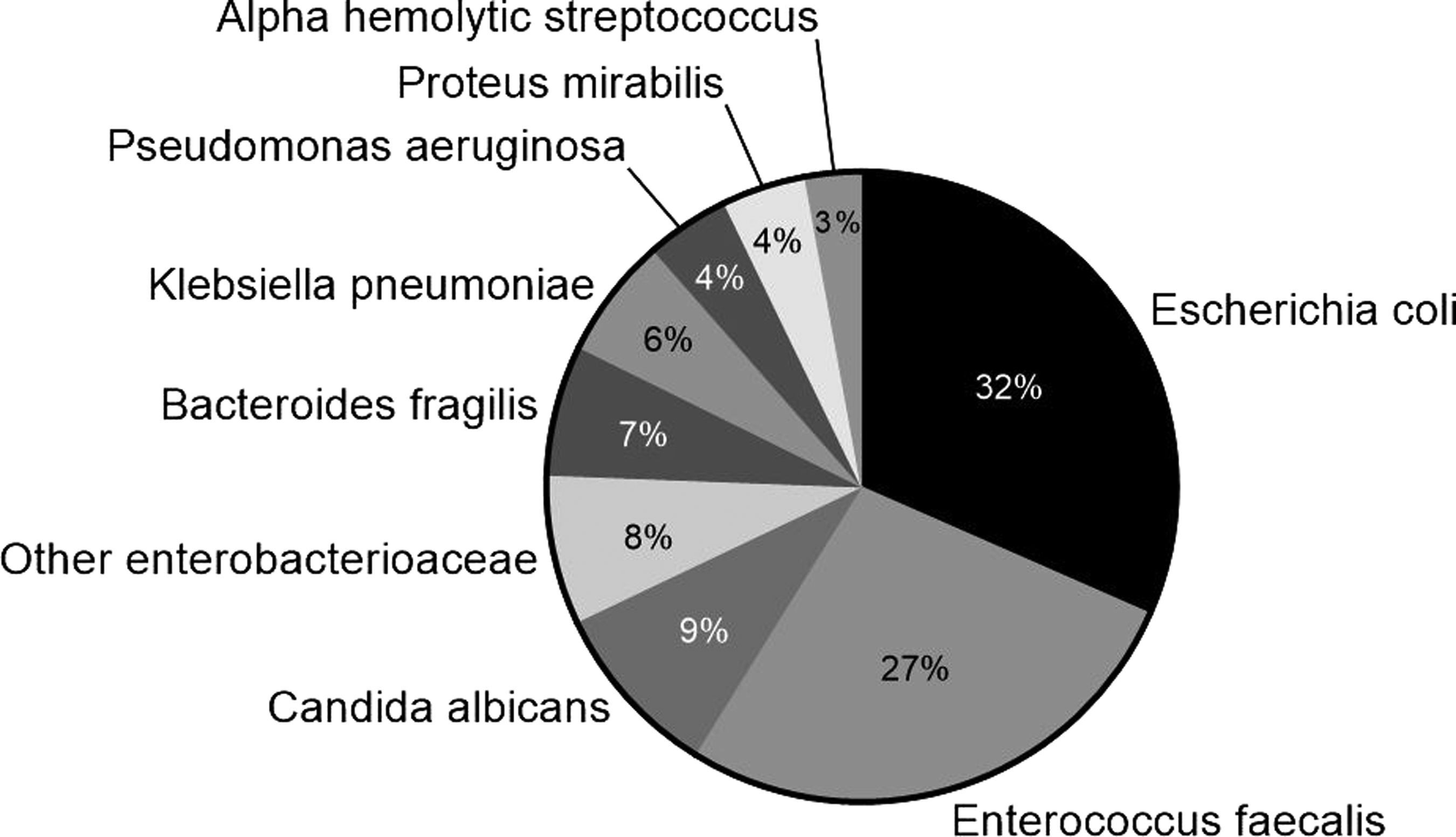
Spectrum of pathogens in patients with organ space infections.
Treatment strategies were surgical management in 85 patients (56%), percutaneous drainage in 36 (24%), and antibiotic treatment only in 32 (21%). Figure 2 gives an overview of the timing of invasive treatments. Twenty-one OSIs (14%) were diagnosed post-discharge. Re-hospitalization for OSI was necessary in 23 patients (15%), independent of whether OSI occurred during the index hospitalization or post-discharge.
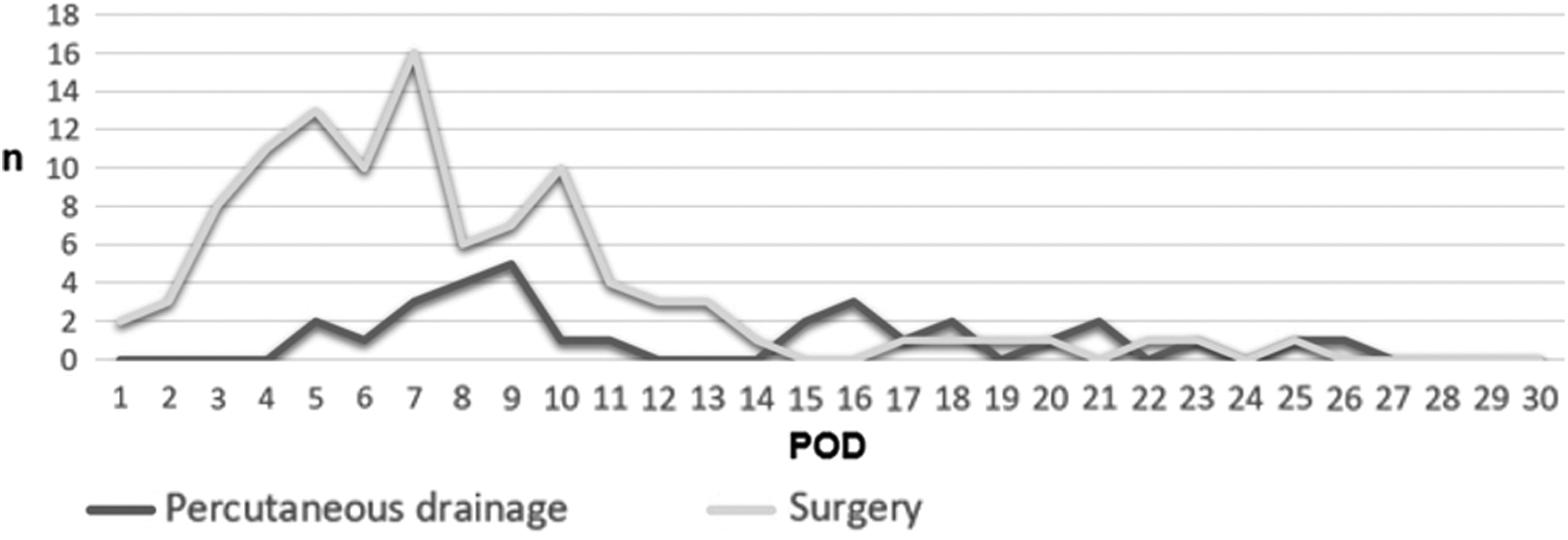
Invasive treatment strategies for organ space infections (OSI). Timing of invasive treatment strategies for OSI monitored until post-operative day 30 comparing antibiotics with percutaneous drainage (blue line) and surgical management (yellow line).
Univariable risk factors for OSI are displayed in Table 1. Independent factors were emergency surgery (OR 2.06; 95% confidence interval [CI] 1.35–3.16), operation duration of >180 minutes (OR 2.10; 95% CI 1.29–3.40), and open surgery (OR 2.51; 95% CI 1.73–3.65) (Fig. 3).
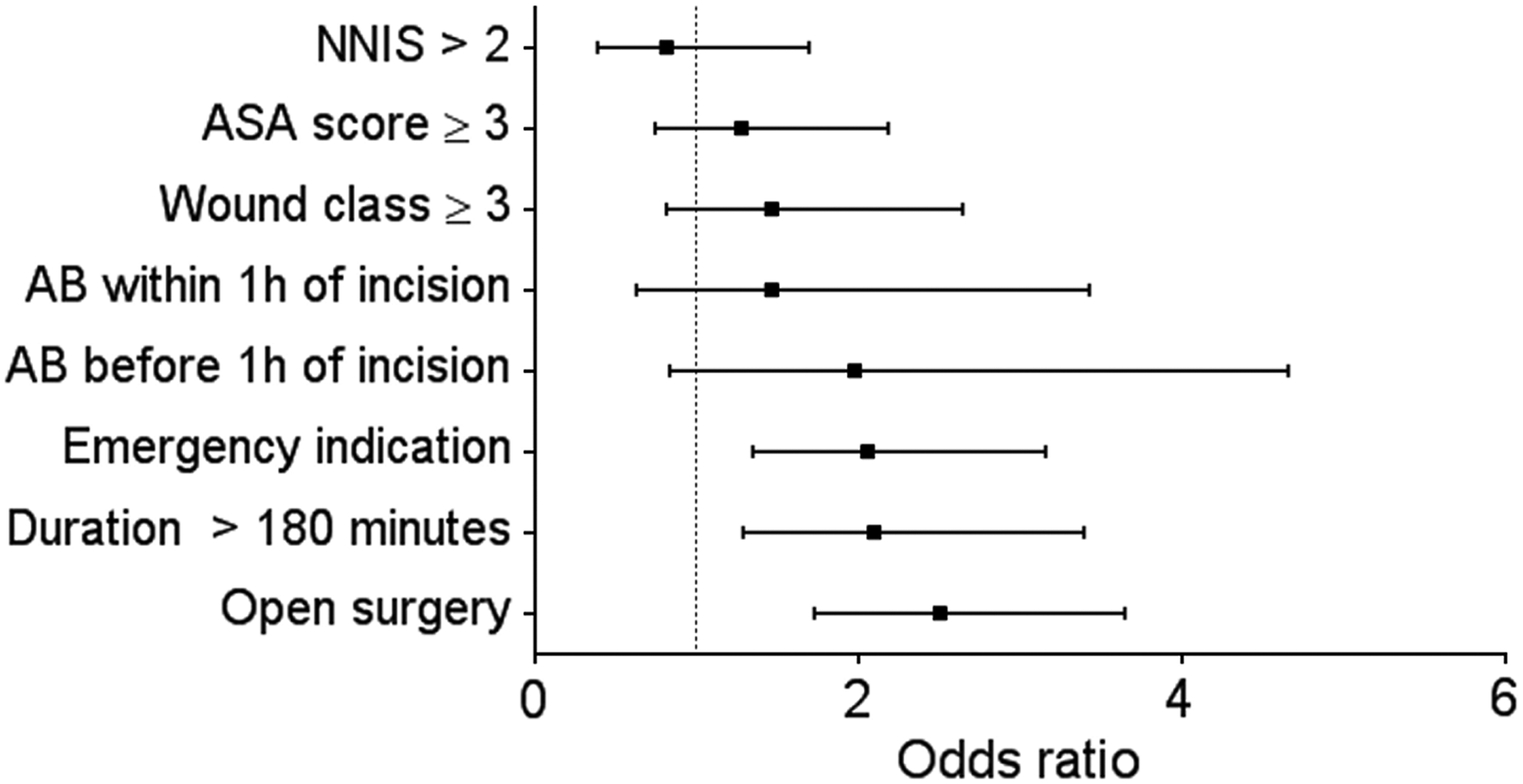
Multivariable analysis of risk factors identified by univariable analysis (p < 0.05) for organ space infections. AB = antibiotic; ASA = American Society of Anesthesiologists; NNIS = National Nosocomial Infection Surveillance score,
Discussion
The main findings of the present study specific to OSI displayed three risk factors on multivariable analysis: Emergency surgery, long operation (>180 minutes), and an open approach. This is an unselected cohort of consecutive colonic resections including 42% emergency cases. The OSIs were detected and treated rather early in the 30-day post-operative surveillance period, and 79% needed invasive treatment through either surgical re-intervention or percutaneous drainage.
The present study focused entirely on OSI, while surprisingly, the literature focuses rather on superficial SSI. There are two good reasons for this: Consistently, OSIs represent the most frequent SSI after colonic surgery; and they have a major impact on patient recovery, morbidity, and length of stay [12]. Different rates of OSI were described in a recent multi-center study when comparing colonic (8%) and rectal (12%) procedures, with some differences in risk factors and outcomes [7]. Notably, the study of Gomila et al. displayed oral bowel preparation combined with antibiotic treatment as protective factors in both colonic and rectal resection [7]. A recent meta-analysis including 38 randomized studies and 8,458 patients showed that mechanical bowel preparation with oral antibiotics was associated with the lowest rate of SSI, reducing both incisional infection and OSI, but there was no difference in the rates of anastomotic leak, re-admission, or re-operation [13]. The present study focused only on colonic resections, as they were systematically and prospectively monitored by the local branch of the Swiss National Infection Surveillance Committee over the five-year study period. All colonic resections, including emergency procedures, were treated according to ERAS guidelines, hence without any mechanical bowel preparation [15]. However, these practices should be revisited considering the growing body of evidence from randomized trials and population-based studies on the utility of mechanical bowel preparation and oral antibiotics before elective colorectal surgery.
The observed rate of OSI (12%) in the present cohort is high compared with that in the literature, where the rate is around 10% [15–17]. Of note, those studies included either only elective surgery [15] or 20% emergency cases only [16]. The present cohort was unselected, with a high rate of emergency procedures (42%) in association with contamination class III and IV, as assessed by the Swissnoso surveillance team. The OSI rate of elective surgery in the present study was 8%, lower than what is described in the literature [15, 16].
An important finding of the present study was the confirmation of the need for invasive treatment in 79% of OSIs, a demonstration of its challenging nature. A detailed overview of surgical and radiologic re-interventions on a day-by-day basis demonstrated peaks during the first 10 days of the 30-day surveillance period (Fig. 2). The low OSI readmission rate, only 15%, confirmed that treatment was performed during the index hospital stay in most cases, similar to the results of Silvestri et al., who treated 92% of infections during the primary stay [17]. Strategies for OSI management after elective colorectal surgery were assessed by a large Spanish multicenter study [3]. Of the 81% patients with OSI (9%) who needed source control, 60% required re-operation and 21% percutaneous drainage, which is congruent with the findings of the present study. Further, the study by Gomila et al. displayed an overall OSI treatment failure rate of 34%. In their study, failure was defined as signs or symptoms of SSI or death by 30 days post-surgery, data that were not available from our surveillance [3].
The existing guidelines on infection prevention were applied in the present Institution, and this may be a limiting factor without auditing compliance [6]. Thus, the observed rate of prophylactic antibiotic administration outside the recommended one-hour window (34%) was considered high and obviously leaves room for improvement, provided it was not attributable to a simple reporting problem. A previously published study described a wide variation among surgeons regarding strategies and adherence to current guidelines [18]. Some recommendations such as the timing and type of antibiotic prophylaxis or use of minimally invasive approaches are evidence based [19], whereas others are rather opinion based, including pre-operative hygiene and site care [2,6]. Moreover, the individual surgeon was identified as an independent risk factor for SSI, probably reflecting differences in the provision of gentle tissue handling and good surgical technique [20].
Several limitations of the present study need to be addressed. Available demographic and surgical data were limited, and other potential confounding factors were not available. On the other hand, data were issued from an independent Swiss national registry and were assessed prospectively in consecutive patients without exclusion. Surgeons were involved in neither data acquisition nor data management, thus eliminating inherent selection bias. Another limitation was that there were no data available on treatment success or long-term outcome. Specifics of ostomy creation and anastomotic leaks as surrogate measures of OSI were not available either.
Conclusions
Organ space infections after colonic surgery were frequent, especially in emergency situations. They usually occurred within 10 days of surgery and needed invasive management in 79% of cases. Risk factors for OSI were prolonged or emergency surgery and an open approach.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.