
Abstract
Abstract
Prosthetic contamination and biofilm formation continue to plague implanted materials. With increasing resistance to traditional antibiotic regimens, alternative approaches to preventing bacterial adhesion and biofilm formation have focused on the physiochemical properties of the prosthetics. Roughness, topography, hydrophobicity, porosity, charge, stiffness, and surface area all influence the processes of adhesion and colonization leading to biofilm formation. In this review, we discuss the physiochemical properties of solid and porous prosthetic materials that influence biofilm formation at the nanometric scale.
As surgical innovation and techniques have advanced, so has the development and use of implants capable of restoring form and function to patients who would be otherwise crippled by disease. More than 65% of all human infections are estimated to be biofilm-related [1,2]. In addition, more than 12 million persons in the United States are reported to be affected by biofilm-related infections every year, with an estimated annual economic burden of $6 billion [3,4]. In 2008, more than one million knee and hip arthroplasty procedures were performed in the United States, reflecting increasing use compared with previous years [5]. Similarly, more than 300,000 incisional hernia repairs are performed each year in the United States, contributing to the more than 20 million worldwide hernia repairs [6,7]. Infection remains the leading cause of medical implant failure and a therapeutic target for morbidity reduction and outcome enhancement.
Medical device infection is intimately tied to biofilm formation and drives both peri-implant morbidity and death [8–10]. Biofilm is a heterogeneous and cooperative community of bacteria embedded in an extracellular matrix attached to a surface [11]. Comprised of a sessile adherent community of cells, as well as a free-floating planktonic segment, the biofilm micro-environment represents a protected niche for growth and diversity [12]. Through digestive enzyme elaboration, resident biofilm bacteria metabolize host proteins adsorbed to the prosthetic surface after implantation [13]. Sessile biofilm bacteria are sheltered effectively from antibiotic agent exposure by physical, chemical, and charge-based barriers. This community-based resistance to environmental stressors renders biofilm a source of difficult to treat acute as well as chronic infections [14]. Accordingly, biofilm is a major public health problem because 60%–80% of human bacterial infections are biofilm related [15].
The formal attribution of the term “biofilm” is relatively recent (1978) and has directed a host of efforts to elucidate growth and communication dynamics, as well as therapeutic approaches to clear or retard biofilm-based infection [16]. Control of material physical properties and characteristics has evolved to nanoscale level innovation. Nanotechnology is the science and engineering of materials whose design, synthesis, and characterization are conducted on the nanometer scale (1 × 10−9 m, or one-billionth of a meter). Devices constructed with nanofeatures not only fall into the realm of nanoparticle development but extend into the creation and control of nanometric elements found on biomaterials and prosthetics [17,18].
As our understanding of the interaction of bacteria and implant surfaces advances, so does our understanding of the importance of implant nanometric features. Therefore, it is appropriate to explore how recent advances in elucidating biofilm structure and function have influenced prevention of implant-based biofilm driven infection [19]. We describe the physiochemical interactions between the implant surface and bacteria at the nanometric scale that promote or retard biofilm formation.
Biofilm Formation on Implants
Medical device colonization that leads to infection often occurs at the time of implantation and involves the complex interactions of bacteria and prosthetic material with the host response [20]. The implant-associated host response of acute and chronic inflammation causes local immune suppression that predisposes the implant and peri-implant tissue to colonization. All medical implantable devices are susceptible to colonization and underpin the known infection rate even in clean cases of 1%–5% [21].
Biofilm formation begins with bacterial adhesion as a key step in the genesis of implant-related infection [22–25]. Van Leeuwenhoek provided an early description of bacterial biofilm on dental surfaces describing both attachment and growth characteristics [26]. The interactions of an implant with human or veterinary biologic systems are termed biointerfacial events. Inflammation, protein adsorption, and encapsulation occur as an attempt to develop a protective cordon between biologic systems and the foreign body [27]. Unlike the host response to bacterial invasion, biointerfacial events are influenced substantially by the nanometric physiochemical surface characteristics of the implant material. The surface structure at the nanometric scale may enhance or retard bacterial adhesion, subsequent colony formation, and ultimate biofilm formation [28]. Understanding bacterial adhesion informs the nanometric design of medical implants to mitigate against biofilm-based infection.
Bacterial adhesion is divided into two stages—the first being a reversible, non-specific binding to the surface and the second being a non-reversible, specific attachment [29]. Initial attachment is mediated by non-specific forces such as Van der Waals, electrostatic, and acid base interactions. In this setting, the bacteria function like colloidal micro-particles attracted to an abiotic surface and to each other [29,30]. Surface charge, chemistry, wettability, and topography all play a role in this adaptive physiologic process (Fig. 1).
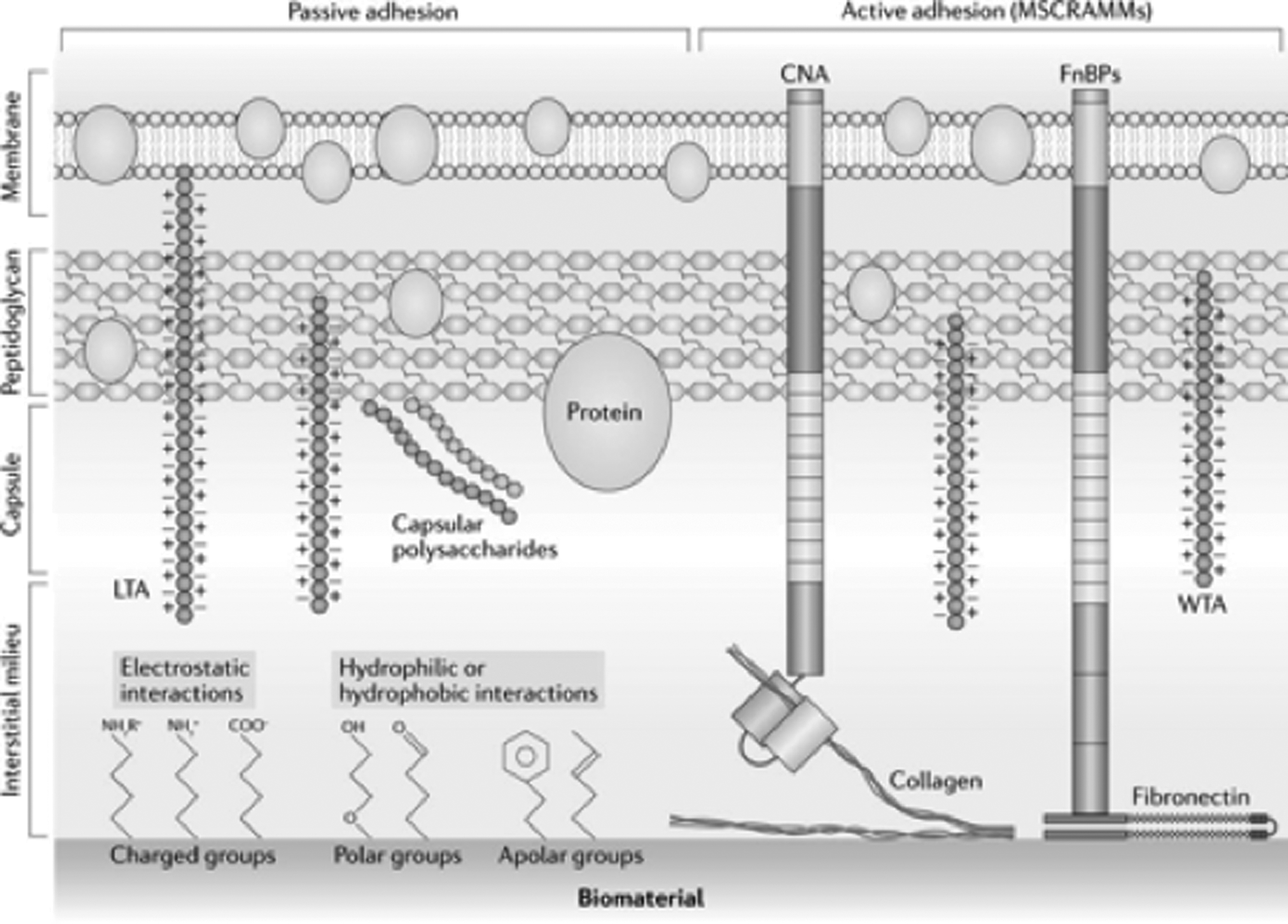
Adhesion of Staphylococcus aureus to implant surface. Bacterial adhesion on the biomaterial surface results from a combination of reversible passive mechanisms and irreversible active mechanisms. The latter involves microbial surface components recognizing adhesive matric molecules (MSCRAMMs), such as the collagen-binding adhesion (CNA) and the fibronectin-binding protein (FnBPs), which are expressed by most Staphylococcus aureus strains and can bind collagen and fibronectin, respectively.
As the implant becomes rapidly coated in host proteins from blood and interstitial fluids, its surface becomes indistinguishable from the host tissue, driving the use of alternative adhesion mechanisms such as bacterial pili and filamentous cell appendages functioning as adhesins [31]. These more specific binding interactions are characteristic of bacteria such as Staphylococcus aureus, which have a cell-wall anchored microbial surface component recognizing adhesive matrix molecules (MSCRAMMs) and secretable expanded repertoire adhesive molecules (SERAMs) [32,33]. Similarly, collagen binding proteins and fibronectin binding proteins also contribute to the specific binding of biologic tissue coating the implant as it becomes incorporated into the surrounding tissues (Fig. 1).
After adhesion, biofilm begins to form through the aggregation of bacteria coupled with extracellular matrix production. Biofilm maturation establishes macro-colonies presenting as towers that undergo internally driven re-modeling. When colony density reaches a pre-determined threshold—generally identified by quorum sensing proteins—some of the colony disperses with disruption of the matrix and release of bacteria into the surrounding environment (Fig. 2). The entire biofilm may also disperse in response to detachment signals from external conditions including starvation, oxidative or nitrosative stress, host factors such as bile salts, and availability of oxygen, iron, and carbon sources [34].
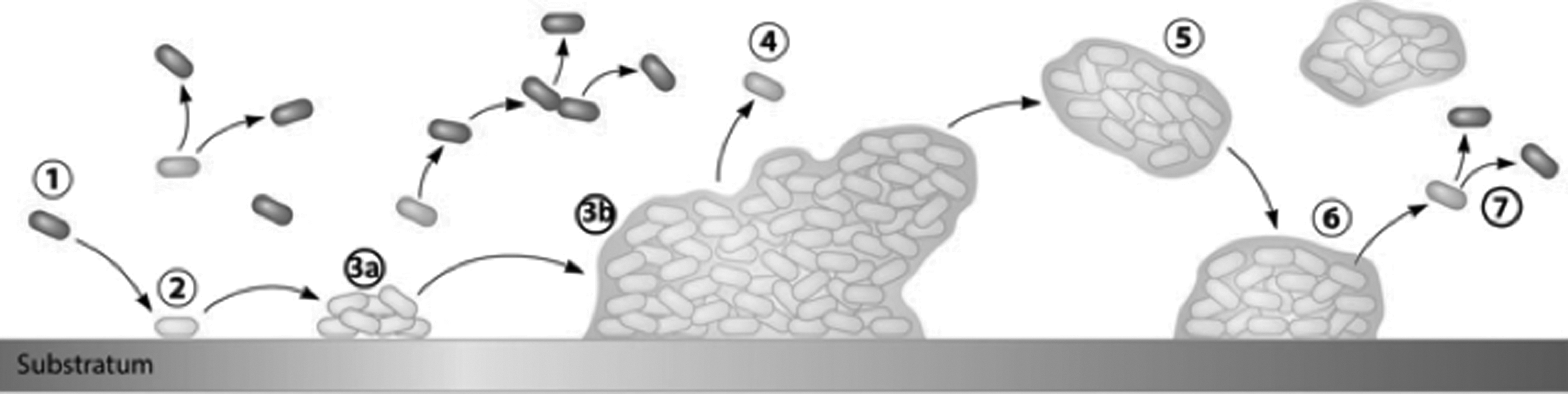
Phases of bacterial adhesion and biofilm formation. The three phases of bacterial (1) colonization and biofilm formation are illustrated. Host factors lead to initial bacterial attachment (2) leading to cell-cell adhesion (3a) and ultimately proliferation (3b). This is followed by microcolony formation (4), biofilm maturation (5, 6) and cellular detachment (7).
Besides biologic signals such as proteins and adhesion molecules, physical and chemical cues of the implant itself have been recognized as important factors that can influence cell behavior [35–37]. Understanding these aspects supports the intelligent and deliberate design of prosthetics to retard bacterial adherence while supporting native tissue ingrowth and prosthetic incorporation to reduce infection potential both during and after implantation.
Nanometric Characteristics of Solid and Porous Prosthetic Surfaces
The physical and chemical properties of the implant surface drive the interaction of the host and bacteria to promote or prevent the colonization and maturation of biofilms on implants. Surface roughness, topography, and stiffness are physical properties that impact the adhesion of host cells and bacteria. The surface tension, polarity, charge, and wettability are chemical characteristics that play roles in the initial adhesion of bacteria to an implant surface (Fig. 3) [38–41]. While these features, inherent to the implant material, are engineered to work collectively to promote implant incorporation, they each possess properties that can be tailored to retard or prevent bacterial adhesion and biofilm formation.
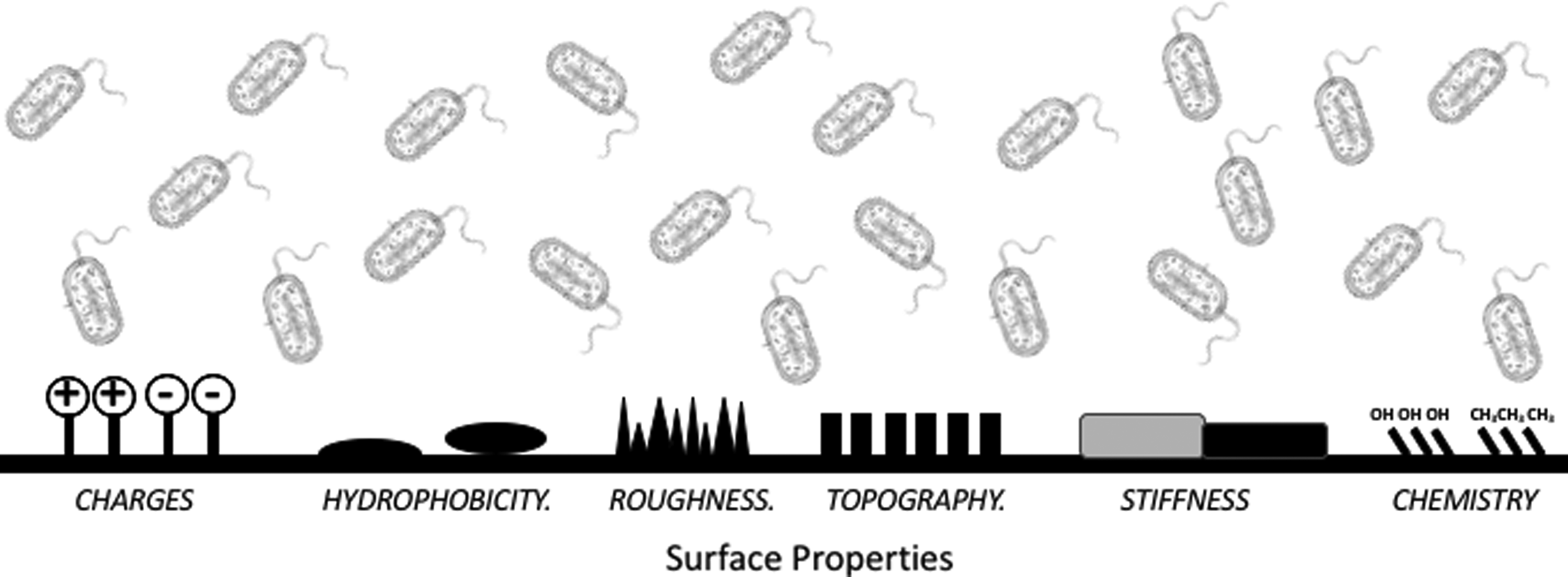
Schematic illustration of bacterial adhesion and the effects of material properties in complex environments. The effects of surface charge, hydrophobicity, roughness, topography, and stiffness are discussed in this review.
Surface roughness
Surface roughness is a parameter that measures variability of feature heights above and below mean surface level, as well as the lateral separations between these features [42]. For more than three decades, the relationship between surface roughness—also termed porosity—and bacterial adhesion has been studied [43]. Early studies were hampered because of device surface topography variability as a reflection of device manufacture technologic immaturity. More recently, technology that enables nanoscale imaging and surface analysis has also improved device manufacture surface topography control [44,45].
Decreased roughness, or increased surface regularity, decreases bacterial adhesion. Conversely, increased surface roughness, or surface irregularity, promotes bacteria adhesion [46]. Roughness is represented by Ra, which is the average of a set of individual measurements of the peaks and valleys of a surface. An increasing Ra indicates increasing surface roughness, and surfaces with a Ra value >0.8 mcm appear more susceptible to bacterial adhesion on the basis of exposed and non-uniform surface geometry [46]. In addition, such surfaces also present pits in which bacteria may evade environmental control measures such as [47].
When extruded, fimbrae enhance adhesion, rendering either blockade of fimbrae extrusion, or retraction of existing fimbrae, a therapeutic target to exploit in reducing implant-related infection. Increased surface roughness increases the production of fimbrae in Escherichia coli adhering to solid surfaces. As a proof of concept investigation, Hsu et al. [47]. demonstrated that with increasing surface roughness, E. coli developed a greater quantity of thicker fimbrae.
Relatedly, bacterial adhesion is impacted by a biologic interface such as protein (such as fibrin) between it and an implanted device. Unsurprisingly, surface nanoroughness inversely impacts surface protein adsorption. Doubling titanium oxide (common in orthopedic implants) surface nanoroughness from 15–30 nm decreases protein binding affinity and total adsorbed protein [48]. Unfortunately, the features that retard the adhesion of bacteria to implant surfaces similarly retard the binding of proteins and thus limit the ability of the implant to become incorporated with the surrounding tissue. This is clinically relevant in abdominal wall mesh implantation where incorporation is required for a successful repair. The interplay of tissue incorporation and bacterial adhesion resistance informs both product design and deployment.
Surface topography
Surface topography, or the pattern of a material surface, is less well studied than is surface roughness [19]. Topography describes the distribution of peaks and troughs across the surface as a measure of surface variability. Hou et al. [49] explored E. coli adherence and biofilm formation on various micro-topographic patterns by using a combination of silicon wafer etching and photolithography to pattern polydimethylsiloxane (PDMS) surfaces. The PDMS surfaces consisted of 10-mcm tall ordered squares where the lateral dimensions (2–100 mcm) and pattern periodicity (5–20 mcm) were varied. They discovered that biofilm preferentially formed between protruding features even when the tops of the pillars were significantly larger than the dimensions of the valleys, suggesting that micro-topographic confinement promotes bacterial adhesion. (Fig. 4)
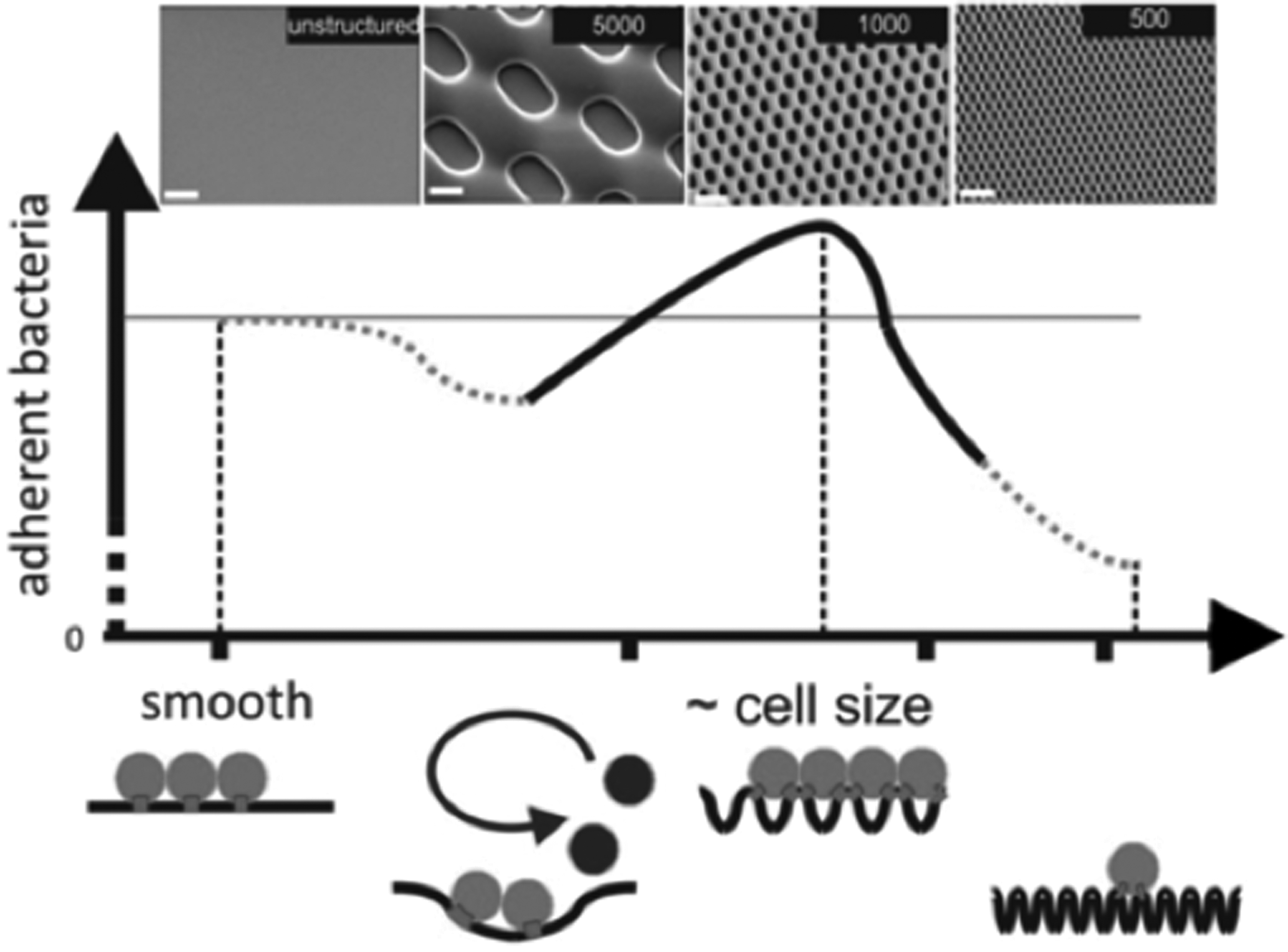
Schematic representation of the dependency of the structure topography on initial bacterial attachment. As the surface topography changes, so does the adherence of bacteria, indicating that smaller features confer bacterial adhesion resistance.
Surface topography modification may reduce bacterial conjugation, a process that enhances antibiotic resistance through plasmid-based transfer of antibiotic resistance genes [50]. One study demonstrated how surface topography affected conjugation-based horizontal gene transfer between E. coli in biofilms on PDMS surfaces. Compared with smooth PDMS, hexagon-shaped patterns with 15 mcm side lengths and 2 mcm inter-pattern distance reduced E. coli biofilm formation. Biofilm formation was promoted when E. coli were grown on surfaces with square patterns with side lengths 20, 50, and 100 mcm, and inter-pattern distances ≥10 mcm. Higher conjugation frequency was noted on pattern sides suggesting potential structural design planning (small and closely spaced surface features) to impede biofilm formation [59].
These findings have clinical relevance when considering both temporary and permanent bioprosthetics including vascular and urinary catheters. The majority of vascular or urinary catheters are designed using smooth surface elements. Given the focus on eliminating central line-associated blood stream infection as well as catheter-associated urinary track infection, surface feature design may warrant re-configuration, and clinical investigation [51,52].
Patterned geometries and pillar-valley design guide both gram-positive and gram-negative bacteria organization by aligning individual cells with the pattern direction [49]. These findings, though, may not translate to other organisms involved in prosthetic contamination. For example, surface feature dimension—relative to organism size—correlated with biofilm formation above or within valleys. The S. aureus and Pseudomonas aeruginosa (∼1 mcm in diameter) tended to be retained within the 2 mcm surface pores while Candida spp. (∼5 mcm in diameter) was found uniformly across a porous surface. This suggests that topographic patterns may be organism or species specific and should be considered when designing new materials. To address this, one may consider a “multi-modal” approach to material design that address the vulnerabilities of culprit species involved in prosthetic contamination.
Surface hydrophobicity
Surface hydrophobicity plays a critical role in the adsorption or repulsion of proteins and bacteria. Hydrophobicity is a physical property describing the ability of a molecule to repel rather than absorb or dissolve water [53]. This explains the increased affinity of proteins to hydrophilic surfaces and decreased affinity for hydrophobic surfaces. Enabling strong protein adsorption will also promote bioprosthetic tissue incorporation. Unfortunately, the same process that enhances protein adsorption also enhances bacterial adherence.
Implanted mesh infection may be catastrophic leading to multiple interventions, hospitalizations, disability, reduced quality of life, and in some circumstances, death. Absorption profiles and bacterial adhesion mitigation varies between commercially available mesh products. In one study, hydrophobic mesh composed of polypropylene or expanded-polytetrafluoroethylene (ePTFE) demonstrated the least adhesion while polyester mesh had the greatest adhesion of S. aureus and E. coli [54,55]. Relatedly, hydrophobic polypropylene mesh more readily cleared methicillin-resistant S. aureus compared with hydrophilic polyester mesh [56].
The addition of composite biomaterials, such as collagen, glycosaminoglycans, and extracellular matrix proteins reduce polypropylene mesh hydrophobicity and attenuate bacterial adherence resistance, underscoring the potentially deleterious impact of mesh enhancement with biomaterials [57]. It is important to understand the potential impact of specific mesh design to inform optimal mesh selection when faced with a clean as opposed to a clean-contaminated operative site that requires or would benefit from mesh reconstruction.
Stiffness
Stiffness describes the extent to which a material resists deformability and has not been well explored with regard to biofilm promotion or retardation [58]. Bacterial attachment to materials of different stiffness including stainless steel, glass, and organic polymers is well chronicled in the context of manufacture as well as surgical site infectiom [59]. Bacteria may detect and differentiate surface mechanical properties by sensors located on flagella or pili [60–64]. Indeed, adhesion of S. epidermidis and E. coli correlates with the stiffness of polymer substrate where growth decreases as stiffness increases [55,61]. More importantly, bacteria attached to less stiff surfaces demonstrated enhanced antimicrobial susceptibility [61,65]. While reduced stiffness may be useful in vascular implants and urinary catheters, it is likely impractical for joint reconstruction or fracture repair hardware. Other elements may instead be modifiable in such circumstances, including surface chemistry and charge.
Surface chemistry and charge
Surface charge determines the binding force between the surface and bacteria and plays an important role for bacterial adhesion and biofilm formation. Because bacteria generally are negatively charged, a positively charged substrate surface enhances bacterial adhesion and a negatively charged one reduces adhesion [66]. While cell repulsion appears intuitively ideal, not all surfaces may be manufactured with a positive charge. Instead, surface modification with cationic groups such as quaternary ammonium and polyethylenimines demonstrated antimicrobial activity resulting in attached bacteria death [67]. Nonetheless, surface negativity alone may be insufficient to retard adhesion and biofilm formation.
P. aeruginosa biofilms growing on negatively charged surfaces elaborated increased cyclic diguanylate monophosphate, a key inducer of extracellular matrix production, compared with neutral or positively charged surfaces. This suggests that these bacteria can evade surface charge-based repulsion and establish viable biofilm [68]. Of course, Pseudomonas may not be the sole bacterium to evidence this ability; such capacity should be considered a virulence factor when evaluating invasiveness and the duration of therapy required for bacteria control or eradication [61,62]. Present manufacturing capability exists to coat medical implants with charge-tunable polymers to alter surface chemistry and charge.
Surface area and porosity
The pore size, surface area, and filamentous structure of surgical meshes must also be taken into consideration when assessing for elements that potentiate or retard bacterial adhesion and proliferation. “Lightweight” meshes tend to have larger pore sizes, smaller surface areas, thinner filaments, and greater flexibility compared with their “heavyweight” counterparts and also appear to stimulate a less robust inflammatory reaction [69]. While lightweight has not been clearly defined in the literature, loosely it refers to mesh with larger pores and thus lower surface area [70].
Porosity is the main determinant of tissue reaction, and pores must be more than 75 mcm to allow infiltration by macrophages, fibroblasts, blood vessels, and collagen. Smaller pore size is also associated with mesh infection, because pores less than 1mcm allow the passage and proliferation of bacteria while preventing infiltration of host defenses (namely, macrophages and neutrophils), and potentially large and highly charged anti-microbial agents [59,71,72]. Theoretically, meshes with pores >75mcm may allow for infection eradication without mesh explantation [73].
Mesh morphologic features that are modifiable as part of the manufacturing process also impact bacterial adherence. Unsurprisingly, meshes with large surface areas bear the highest risk for bacterial adherence and infection [34,64]. In this way, multi-filament mesh construction increases interstices across a greater surface area that further supports bacterial attachment, growth, and evasion of both host defense and exogenous agents. Relatedly, monofilament have less surface area compared with multi-filament meshes. Therefore, monofilament mesh constructed with large pore sizes and relatively small surface areas appear the most bacterial adherence resistant and are often termed lightweight [69].
Unlike the high porosity of woven polymer meshes, ePTFE is a chemically inert hydrophobic fluoropolymer with a negatively charged surface; ePTFE is known to undergo encapsulation by the host. The ePTFE microporous nature allows bacterial passage into its interstices, but prevents immune detection and effector cells, such as macrophages, to enter. Accordingly, ePTFE demonstrates the highest rates of bacterial adherence, biofilm propagation, and infection compared with woven mesh [74,75].
Conclusion
Bacterial infection from biofilm formation on medical implants and prostheses remains a leading cause of implant failure. Physical and chemical nanometric features of implant materials such as roughness, topography, hydrophobicity, porosity, charge, stiffness, and surface area individually and collectively influence bacterial adhesion and biofilm formation. Understanding how bacteria interact with specific implant features should inform the design of prostheses that effectively prevent biofilm formation through a priori suppression of bacterial adhesion rather than by using salvage maneuvers. Nanoscale feature control remains an under-explored and under-utilized avenue for medical device implant preservation and post-implant surgical site infection mitigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.