
Abstract
Abstract
Background:
Cytoreductive surgery (CRS) and hyperthermic intra-peritoneal chemotherapy (HIPEC) is a complex surgical intervention with associated risks. Central venous catheter (CVC) line sepsis is one of a number of potential morbidities. The aim of this study was to calculate the incidence of catheter-related infection (CRI) in a CRS and HIPEC patient population and to assess its influence on length of hospital stay.
Methods:
Data were collected on consecutive patients who underwent CRS HIPEC between August 2013 and October 2017. Data included patient demographics, timing of CVC insertion/removal, time spent in critical care, and CVC tip/blood culture results. Charts were reviewed for patients with both positive CVC culture and positive blood cultures to assess for evidence of catheter related infection and systemic inflammatory response syndrome (SIRS).
Results:
Data on 100 consecutive CRS HIPEC operations performed between August 2013 and October 2017 was analyzed. There were 11 CRIs in 100 CVCs, resulting in a CRI rate of 16.2 per 1,000 CVC days. Patients within the CRI group had a longer high-dependency unit (HDU) stay compared with the non-septic group (6 days vs. 4.07 days, p < 0.05). The CVC duration for the CRI and non-CRI group was 8.4 and 7.6 days, respectively (p = 0.12). The CRI group also had an increased total hospital length of stay (LOS; 20.8 days vs. 15.4 days, p < 0.05). On average, CRIs occurred eight days post-operative and four days post-HDU discharge. There was no association identified with longer CVC duration (p = 0.34). There has been an annual decline in CRI rates in CRS and HIPEC patients over the duration of the study period from 19.1 per 1,000 CVC days in 2016 to 8.2 per 1,000 CVC days in 2017.
Conclusion:
This is the first study to report on CRI rates in patients undergoing CRS and HIPEC. The CRI rate of 16.2 per 1,000 CVC days is higher than the overall national figure of 5.2 per 1,000 for CVC lines inserted in the operating room. Patients who developed line sepsis had longer HDU and longer overall hospital stay. Catheter-related infection was noted post-HDU discharge in all cases. Implementation of a CVC care bundle in the later years of the study period coincided with a reduction in CRI rates.
Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is a complex surgical oncologic procedure for resection of peritoneal malignancy combined with intra-operative delivery of heated intra-peritoneal chemotherapy directly into the abdominal cavity. Cytoreductive surgery with HIPEC is currently the accepted standard of care for patients with pseudomyxoma peritoneii, primary peritoneal mesothelioma, selected patients with colorectal cancer peritoneal metastases, and advanced stage ovarian cancer [1,2]. Because of the extensive tumor resection required and the anticipated protracted recovery period, patients routinely undergo central venous catheter insertion for perioperative hemodynamic monitoring, to facilitate post-operative parenteral feeding and for delivery of medical therapy such as inotropic support. Cytoreductive surgery and HIPEC have substantial risks of morbidity and mortality with perioperative sepsis being the most common complication [3–5]. It is therefore imperative to try to reduce sepsis rates in these patients to optimize outcomes, reduce the associated economic burden, and facilitate timely discharge [6].
Catheter-related infection (CRI) is one of the most commonly encountered serious health-care–associated infections (HCAI) in post-operative patients. Catheter-related infection is defined as the presence of bacteremia originating from an intravenous catheter and accounts for 10%–20% of all nosocomial infection and may occur in and complicate the course of up to 10% of intensive care unit (ICU) patients [7]. The pathogenesis of CRI has been associated with several interconnected factors. The catheter may be involved in pathogenic pathways such as colonization of the catheter tip with skin flora; colonization of the CVC lumen caused by contamination; hematogenous seeding of the CVC from other potential infected sites; and contamination of the catheter lumen from infused contents [8–11]. Catheter-related infection-associated morbidity and expense are the most substantial adverse effect of CVCs [12,13]. As a result, the reduction of CRI has been proposed as a measure of healthcare quality internationally [14]. The majority of CRIs are associated with CVCs, and in prospective studies, the relative risk for CRI is up to 64 times greater with CVCs compared with peripheral venous catheters [15]. Factors influencing CRI rates include the underlying disease, the method of catheter insertion, the site of catheter insertion and duration, and the reason for catheterization. Additional risk factors which may be encountered in CRS/HIPEC patients include administration of parenteral nutrition through intravascular catheters, local risk factors such as poor personal hygiene due to stoma formation, Staphylococcus aureus nasal colonization, older age, lower hemoglobin level, lower serum albumin level, and recent hospitalization/ICU admission or surgery [16–19].
To date there is no reported study analyzing CRI rates in patients undergoing CRS and HIPEC. The aim of this study was to calculate CRI rates in a CRS/HIPEC population compared with reported national and international rates, to assess the impact of CRIs on patient recovery and discharge, and to analyze the influence of a CVC care bundle on CRI rates within our institution.
Methods
A prospectively maintained CRS/HIPEC database was searched to identify consecutive patients treated between August 2013 and October 2017. Data included patient demographics, timing of CVC insertion/removal, operative parameters, timing of high-dependency unit (HDU) discharge, and CVC tip/blood culture results. Charts were reviewed in the case of patients with both positive CVC and positive blood cultures to assess for evidence of systemic inflammatory response syndrome (SIRS) and establish a diagnosis of CRI.
Definitions
Blood stream infection
Blood stream infection was defined as one positive blood culture for a recognized pathogen or a patient having at least one of the following symptoms or signs: fever (>38°C), chills/rigors, and hypotension. Recognized bacterial or fungal pathogens were cultured from one or more blood samples. Pathogens classified as skin contaminants included coagulase-negative staphylococci, Micrococcus sp., Propionibacterium acnes, Bacillus sp., and Corynebacterium sp.
Catheter-related infections
Catheter-related infection was defined as bacteremia or fungemia in a patient who had an intravascular device and more than one positive blood culture obtained from the peripheral vein with clinical manifestations of infection (e.g., fever, chills, and/or hypotension) and no apparent source for blood stream infection (with the exception of the catheter). One of the following should be present:
A positive result of semiquantitative (>15 colony forming units (CF) per catheter segment) or quantitative (>102 CFU per catheter segment) catheter culture, whereby the same organism (species) was isolated from a catheter segment and a peripheral blood culture [20,21]. Simultaneous quantitative cultures of blood with a ratio of greater than 3:1 CFU/mL of blood (catheter vs. peripheral blood); differential time to positivity (growth in a blood culture drawn through catheter hub is detected by an automated blood culture system at least two hours earlier than a simultaneously drawn peripheral blood culture of equal volume).
Patients
All patients undergoing CRS/HIPEC during the study period were included. Patients with CVCs inserted in anatomic locations other than internal jugular/subclavian vein and patients with early non-functioning CVCs necessitating removal were excluded.
Non-antibiotic/silver impregnated CVCs were inserted at anesthesia induction under an aseptic technique using Doppler ultrasound guidance. The timing of CVC insertion was recorded in the theater maintenance system (TMS). The CVC removal time was recorded as the time documented in the patients HDU nursing notes or patient chart. Documented complications with CVC removal and external surrounding skin condition were also recorded. All patients received standard prophylactic antibiotics for 24 hours (co-amoxiclav, 1.2 g) and total parental nutrition was initiated on post-operative day one via the CVC until oral diet was established.
A dedicated CVC daily ward round was performed by an assigned advanced nurse practioneer from October 2015. This involved examining the lines and highlighting poor line care, identifying lines at risk of infection, sterile catheter flush technique, and also nursing and allied health professional education regarding line care and recognition of catheter sepsis. Furthermore, a detailed protocol was constructed by the advanced nurse practitioner with daily insertion of patient parameters (Supplementary Appendix). This was included in all patient charts recording the number of CVC in situ days, patient parameters, daily infection markers, patient temperature, antibiotic use, and type of therapy delivered via the catheter. Central venous catheter tips were sent for culture in the majority of cases. In cases of suspected CRI, peripheral and central blood cultures via the CVC were taken, the CVC was then removed and the catheter tip was sent for culture.
Statistical analysis
Statistical analysis was performed using Microsoft® Excel program (Microsoft, Redmond, WA) and Minitab version 18 (Minitab, State College, PA) with a p < 0.05 considered significant. Comparison of outcomes between two groups (bacteremia vs. non-bacteremia) was performed using paired t-test and one-way analysis of variance (ANOVA) was performed to analyze the means of three or more factors within the study. Univariable and multivariable analysis was performed to examine the impact of one or multiple factors on outcome.
Results
In total, 100 CRS and HIPEC procedures were performed during the study period comprising 59 females and 41 males. The patients ranged in age from 31 to 84 years (mean, 57.2 years). All CVC lines were inserted in-theater at the time of surgery as recorded by the electronic TMS. The mean CVC line duration was 7.7 days (range, 1–18 days). The majority of patients had CVCs in situ for 7–9 days (n = 49, p < 0.05; Fig. 1). One patient had the CVC removed on the first post-operative day because of malfunction.
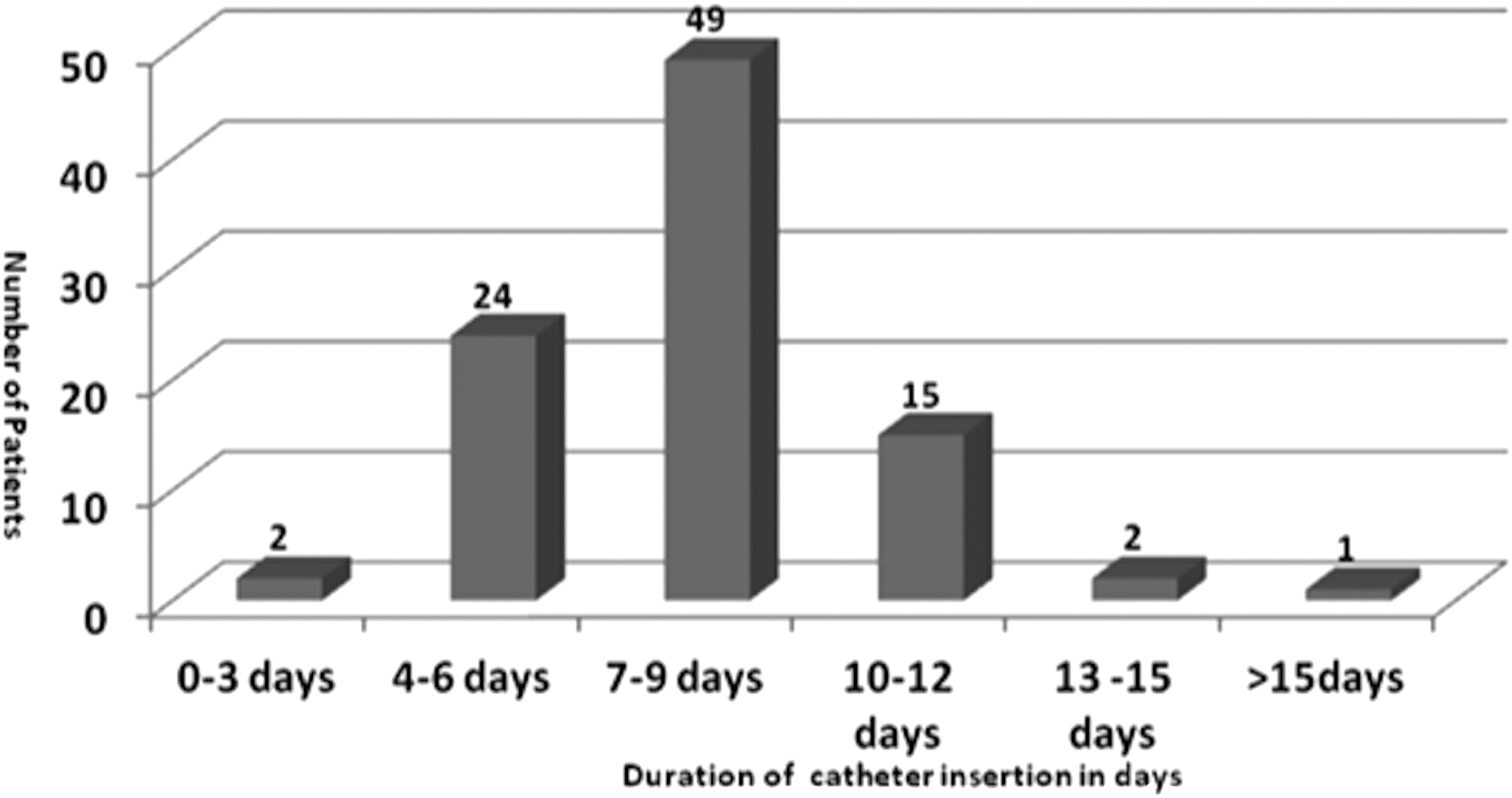
Duration of central venous catheter (CVC) in situ (p = 93). A substantial proportion of patients had CVC lines in situ for 7–9 days (n < 0.05).
Of the 100 CVC lines, 77 were sent for tip culture at removal. Forty-three of these patients had concurrent blood cultures performed (Fig. 2). Thirteen patients had both positive line culture and positive blood cultures, with 11 having the same pathogen representing a CRI incidence of 11%. These 11 patients' charts were reviewed for evidence of SIRS which was identified in all cases. This resulted in a CRI rate of 16.2 infections per 1,000 CVC days in the total 100 CRS/HIPEC cohort.

Patient flow chart from a cohort of 100 patients. Thirteen patients had both positive tip line and blood cultures and 11 patients had documented evidence of systemic inflammatory response syndrome (SIRS). This results in a central venous catheter (CVC) bacteremia rate of 11% that is equivalent of 16.2 infections per 1,000 CVC days for the total cytoreductive surgery (CRS) and hyperthermic intra-peritoneal chemotherapy (HIPEC) cohort.
An analysis of organisms isolated from both CVC tip and peripheral blood cultures was performed. The organisms cultured were coagulase-negative staphylococci (n = 8), Staphylococcus aureus (n = 2), and methicillin-resistant Staphylococcus aureus (MRSA; n = 1, Table 1).
Central Venous Catheter Tip and Peripheral Blood Culture Organisms
Description of organisms cultured from both the tip of the CVC and peripheral blood culture bottles. All 11 patients displayed signs of SIRS (11%).
CoNS, coagulase-negative staphylococci; CVC, central venous catheter; SIRS, systemic inflammatory response syndrome.
There was no difference in patient age between the two groups (61.8 years vs. 59.1 years, p = 0.26; Fig. 3). The average HDU LOS for the entire group was 4.6 days. Patients with CRI had a prolonged HDU stay compared with the non-CRI group (6 days vs. 4.07 days, p < 0.05). The mean CVC duration, for the CRI and non-CRI group was 8.4 and 7.6 days, respectively (p = 0.12). The CRI group also had an increased total hospital LOS (20.8 days vs. 15.4 days, p < 0.05). On average, CRI was noted at day eight post-operative and day four post-HDU discharge. There was no association identified with longer CVC duration operative length of time, peritoneal carcinomatosis score (PCI)/surgical resection extent (p = 0.34).
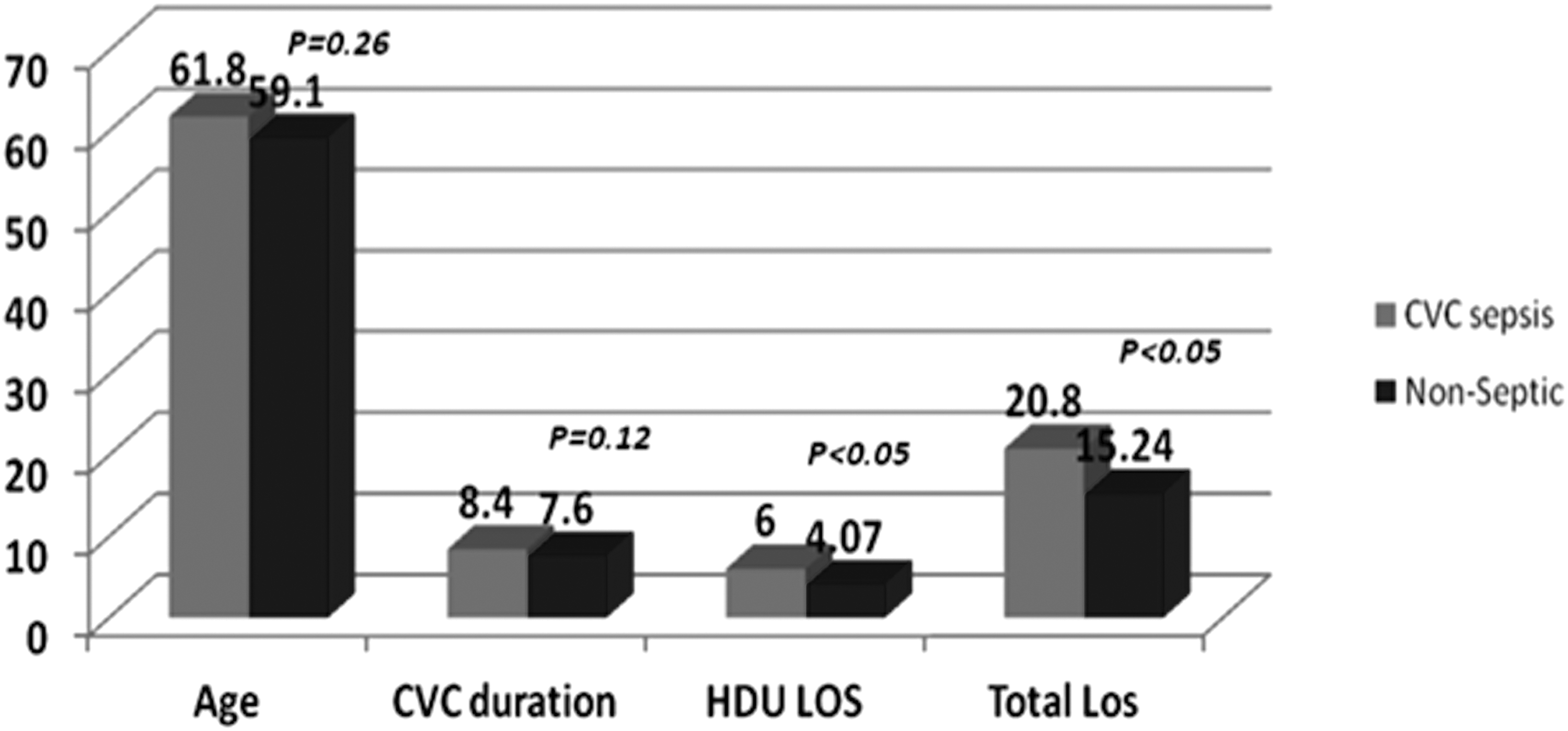
Parameters of patients who did not develop central venous catheter (CVC) sepsis in comparison to those who did. Patients who developed CVC sepsis had increased high-dependency care unit (HDU) stay (6 vs. 4.07 days) with an increased total length of stay by 5.6 days (p < 0.05).
There was a substantial annual decline in CVC sepsis rates in CRS/HIPEC patients over the duration of the study period from 19.1 infections per 1,000 CVC days in 2016 to 8.2 infections per 1,000 CVC days in 2017 (p < 0.05; Fig. 4). This has coincided with the formulation of a CVC care bundle and institution of a critical care advanced nurse practitioner in October 2015.
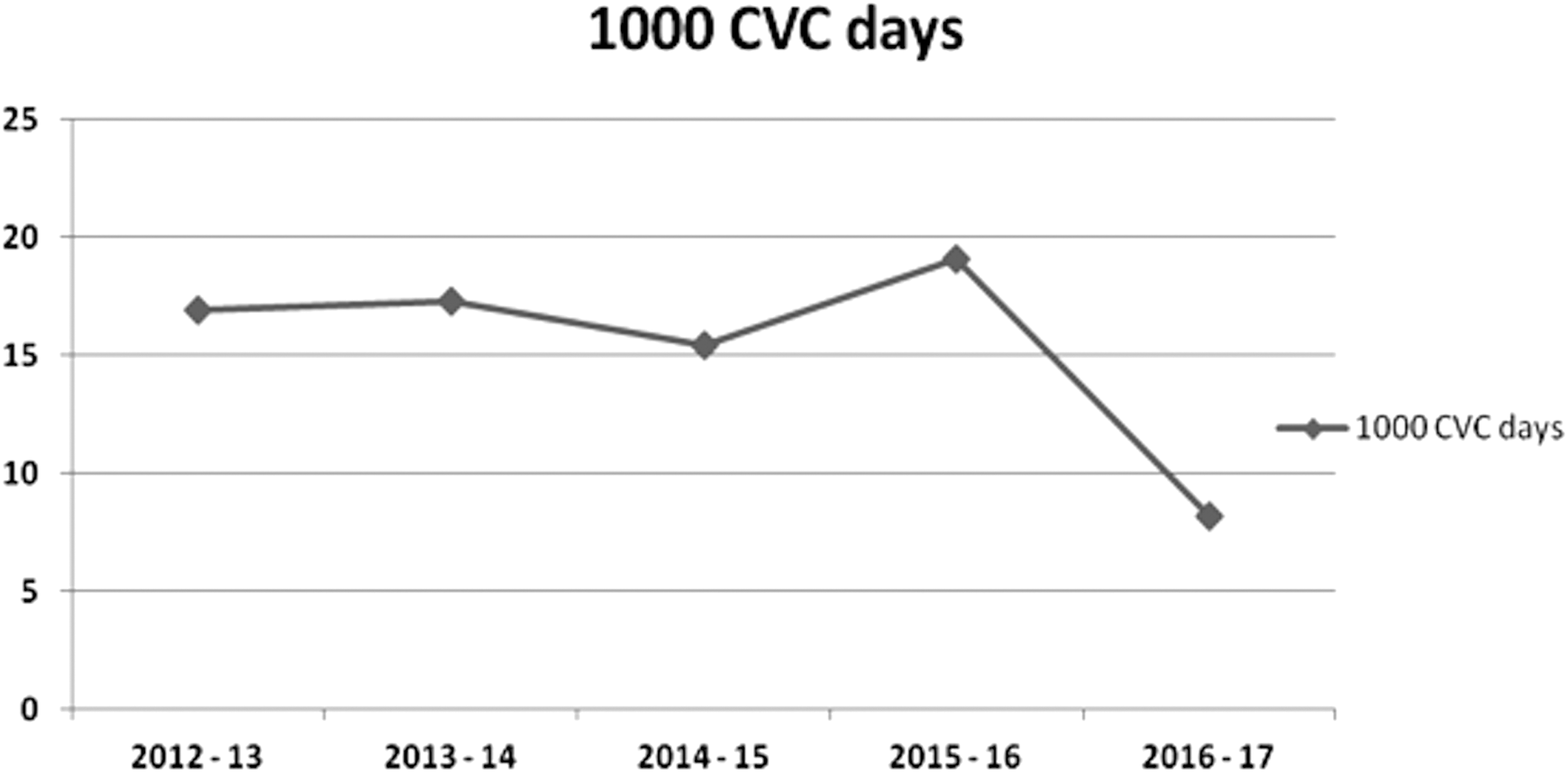
Annual catheter-related infection (CRI) rates 2013 to 2017. The CRI rates reduced from 19.1 infections per 1,000 central venous catheter (CVC) days in 2016 to 8.2 infections per 1,000 CVC days in 2017 (p < 0.05).
Discussion
To date this is the first report to highlight an increased incidence of CRI among patients undergoing CRS and HIPEC. In this study of 100 patients undergoing CRS and HIPEC, 13 patients had both positive tip line and blood cultures with 11 patients having documented evidence of SIRS resulting in a CRI rate of 11%, which is equivalent to 16.2 infections per 1,000 CVC days for the total CRS and HIPEC cohort. The organisms cultured were coagulase-negative staphylococci, followed by Staphylococcus aureus and MRSA. The findings show increased CRI in this patient population compared with other non-HIPEC patients receiving total parenteral nutrition (TPN) at our institution. In addition CRI of 16.2 infections per 1,000 CVC days compared national reported figures of 5.2 infections per 1,000 CVC days. The current internationally reported overall CRI rates are 1.7–11.3 cases per 1,000 CVC days [22–24]. Within the CRS and HIPEC cohort CRI was noted at a mean of eight days post-operative and four days post-HDU discharge. Catheter-related infection was associated with increased length of HDU and overall hospital stay. There were no CRI-associated deaths in the current study.
Many studies have reported an association between increased indwelling catheter duration and CRI rates, however, within our cohort the duration of CVC did not influence overall rates of CRI [25,26]. Other independent risk factors for CVC colonization are trauma or absence of septic shock at ICU/HDU admission, femoral or jugular insertion, and absence of antibiotic therapy at CVC insertion. Our patients undergoing CRS and HIPEC have CVCs inserted in the jugular vein and antibiotic therapy is commenced post-induction of anesthesia and CVC insertion. Moreover, a proportion of patients within the CRS and HIPEC group would have received chemotherapy/radiotherapy and additionally the use of post-resectional intraperitoneal chemotherapy may result in a degree of immunocompromise.
A number of studies have reported an increased risk of CRI in patients undergoing chemotherapy [27,28]. In a study examining CRI in 371 patients with cancer the authors identified three factors that remained noteworthy for CRI development in a multivariable analysis [29]. One factor was delivery of TPN (odds ratio [OR], 28.5; 95% confidence interval [CI], 4.2–200). All patients in the current study received TPN because of an anticipated delay in return of gastrointestinal tract function as a consequence of underlying ileus secondary to prolonged surgical procedures and intraperitoneal chemotherapy. This association between TPN use and CRI has been shown in other studies in patients with colorectal cancer and it is postulated that it is related to increasing catheter manipulation and consequent catheter contamination [30,31].
Saint et al. [32] documented the economic and clinical burden of CVCs and reported that in patients with standard, non-coated CVCs in place for an average of 8 days, 24.7% developed catheter colonization (95% CI, 22.0%–27.5%) and approximately 5.2% developed catheter-related blood stream infection (CRBSI). Patients who developed CRI in our study had an increased HDU care (6 vs. 4.07 days) with an increased overall hospital LOS by 5.6 days. It has been widely documented that CRI independently increase hospital cost and LOS [18,19,33,34]. In the United States it is estimated that the additional cost of CRI ranges from $6,005 to $9,738 [32]. Similarly, a study in 2005 reported that CRI was associated with a 12-day increase in the total duration of hospitalization, with 8 of these days being in the ICU [35].
It has been recognized that some factors attributed to CRIs are modifiable and this in turn has led to the development of CVC care bundles. The application of such care bundles has been shown to reduce risk, costs, and associated hospital LOS [36]. During the study period in the current experience a care bundle was initiated in October 2015 led by a specialist nurse led service for education and CVC line inspection. This care bundle may have been a factor in the reduction of CRI within the CRS and HIPEC cohort from 19.1 infections per 1,000 CVC days to 8.2 infections per 1,000 CVC days. The bundle combined hand hygiene, maximal barrier precautions upon CVC insertion by the physician inserting the catheter, use of a 2% chlorohexidine gluconate (CHG) in 70% ethanol scrub for the insertion site, and optimum catheter site selection such as subclavian vein followed by the internal jugular vein where appropriate. Daily examinations of the central line, surrounding skin, and dressings was performed by the specialist nurse to identify patients at-risk of CRIs and ensure optimum hygiene use by ward nursing staff. Catheters were cleaned daily with ethanol swabs and early removal was promoted when the CVC was no longer in use. A prospective chart was maintained in all patient notes that included daily documentation of details such as patient vital signs, duration of catheter insertion, and instillation therapy (Supplementary Appendix).
Our study has limitations inherent to its single-center experience with relatively small numbers. We have, however, identified a higher rate of CRI in patients undergoing CRS HIPEC for advanced malignancy. Risk factors for CRI in this cohort may include the use of parenteral nutrition and perioperative immunocompromise. The application of a dedicated CVC care bundle may have contributed to the reduction in the rate of CRI noted during the study period. We have uniformly adopted this bundle and will continue to monitor rates of CRI closely in this high risk group of patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.