
Abstract
Abstract
Background:
This study was performed to investigate the combination of admission serum procalcitonin (PCT) and albumin (alb) concentrations as a diagnostic predictor for discriminating patients with nosocomial blood stream infection (BSI) among those with spontaneous intra-cerebral hemorrhage (ICH).
Methods:
We conducted a retrospective study on patients with ICH and hospital-acquired BSI. Clinical and microbiological data were compared in patients who experienced nosocomial BSI during a hospital stay and those who did not. Multivariable logistic regression analyses were used to identify independent risk factors for nosocomial BSI. A receiver operating characteristic (ROC) curve analysis was performed to compare the predictive accuracy of the albumin:PCT ratio.
Results:
Patients with nosocomial BSI had lower albumin:PCT ratios than those without BSI (11.739 [3.192–38.452] versus 200.000 [40.634–417.500]; p < 0.001). Multivariable logistic regression analysis revealed that the albumin:PCT ratio (odds ratio [OR] 1.006; 95% confidence interval [CI] 1.002–1.011; p = 0.001], white blood cell count (OR 1.129; 95% CI 1.044–1.220; p = 0.002), and shock (OR 4.504; 95% CI 1.774–11.435; p = 0.002) were independent predictors of nosocomial BSI, allowing distinction of patients with the infection from those without. The area under the ROC curve for the albumin:PCT ratio was 0.830 (95% CI 0.768–0.892; p < 0.001). The cut-off value of the albumin:PCT ratio was <1.087 with a sensitivity of 90.6% and a specificity of 98.8%. In the subgroup of 85 patients with nosocomial BSI, the albumin:PCT ratio in patients with shock was lower than that in those without shock (7.154 [2.975–26.267] vs 28.000 [3.818–57.812]; p = 0.027).
Conclusion:
The albumin:PCT ratio can be used as an early diagnostic predictor for nosocomial BSI in patients with ICH. Additionally, BSI patients with lower albumin:PCT ratios are more likely to experience shock. The albumin:PCT ratio is expected to be a rapid and low-cost tool for clinical practice.
Spontaneous intra-cerebral hemorrhage (ICH) accounts for approximately 10%–20% of strokes and has a poor prognosis and high morbidity and mortality rates throughout the world [1–3]. Because of the various catheters that are an indispensable part of current medical practice, patients with ICH have a greater risk of actual or potentially life-threatening infection and sepsis, which require prompt diagnosis and appropriate antimicrobial therapy to reduce the associated morbidity and death [4]. The 2016 European Centre for Disease Prevention and Control (ECDC) Annual Epidemiological Report showed that 6% of patients admitted to an intensive care unit (ICU) for more than two days suffer pneumonia, and 4% and 3% exhibited blood stream infection (BSI) and urinary tract infection (UTI), respectively [5]. Nosocomial BSI is an important issue in ICH patients because of the secondary brain damage, severe complications, and increased morbidity and mortality rates in patients with neurologic disorders [6, 7].
In therapeutic decisions, the ability to discriminate ICH patients with nosocomial BSI immediately from those without is important, as by providing appropriate treatments for these patients, sepsis-related organ failure can be avoided. However, it is time-consuming to diagnose BSI if it can be confirmed only by blood culture [8]: depending on the time required to obtain culture results, BSI diagnosis will take at least 48 to 72 hours. In addition, false-positive results may occur as a result of contamination. Therefore, rapid and efficient diagnostic methods are necessary for discriminating patients with BSI among those with ICH.
In the last decade, procalcitonin (PCT) has been recommended as a biomarker for bacterial infection and sepsis in critically ill patients and may help to predict bacteremia [9–11]. Furthermore, PCT-guided strategies have reduced antibiotic use significantly [12,13]. The test for PCT exhibits good sensitivity but occasional poor specificity [14]. Some studies have observed that PCT concentrations can increase under noninfectious conditions and may remain low during actual infections [15]. Albumin is another a powerful marker of clinical disease outcomes, because its concentration tends to decline during acute-phase infections [16–18].
The correlation between albumin and PCT in the early diagnosis of BSI in patients with ICH still is not clear, and there is no relevant research report at present. We hypothesized that the albumin:PCT ratio could be a predictive indicator for the early diagnosis of BSI in ICH. The purpose of this study was to investigate the application of the albumin:PCT ratio as a predictive factor for the early diagnosis of nosocomial BSI among patients with ICH. We compared the albumin:PCT ratio with currently available biomarkers such as blood leukocyte counts, neutropenia, and C-reactive protein (CRP) concentration.
Patients and Methods
This retrospective study selected 170 patients with ICH admitted to the ICU of our tertiary-care university teaching hospital from January 2010 to May 2018. The adult ICU of this hospital admits both medical and surgical patients and has 26 beds. The number of annual patient admissions was 1,002; among these patients, 25% had severe ICH. Patients were enrolled if they fulfilled the criteria of age above 18 years and admission within 24 hours after ICH. Patients with past febrile diseases, burns, immunosuppressive therapy, antibiotics used for three days before admission, and death within 48 hours after admission and those with ICH attributable to trauma, tumor, arteriovenous malformation, or infarction were excluded from the study. Blood cultures taken peripherally or from the catheter line were ordered on clinical suspicion of infection and at the discretion of the clinical team.
Blood samples for measuring PCT, white blood cell (WBC) count, leukocytes, CRP, and albumin were obtained on admission. The BSI was determined retrospectively from written documentation by the infectious disease team, whose decision was based on objective clinical evidence, microbiological data, and clinical judgment. All patients were followed up for 28 days. The protocols used to prevent BSIs in our hospital included maximum barrier precautions, hand hygiene, chlorhexidine skin disinfection, choice of the best catheter location for the preferred insertion site in the subclavian vein, and the need for a daily catheter examination.
Definitions
Cases of nosocomial BSI were those with: (1) an infection occurring after more than 48 hours in the hospital [19]; (2) one or more blood cultures positive for a known pathogen. For coagulase-negative staphylococci and other common skin flora, at least two positive blood cultures with the same microorganism from blood samples obtained at least two hours apart but not exceeding a 48-hour period were required; (3) sepsis according to the criteria of the 2016 International Sepsis Definitions Conference [20]; and (4) a central line-associated blood stream infection (CLABSI) (a laboratory-confirmed BSI) in those patients who had a central venous catheter that was diagnosed within 48 hours of the onset of BSI unrelated to other site infections [21]. An episode of BSI was defined in cases where all positive blood cultures were extracted within three days [22]. A separate episode of BSI was said to be present when a positive blood culture occurred more than three days after a prior positive culture. However, repeated isolates of the same organism from the same source were considered a single episode, even for cultures taken more than three days apart.
Patients were divided into two groups according to the presence or absence of BSI. The subgroup analysis considered two groups on the basis of the occurrence or absence of sepsis or shock, as defined by the American College of Chest Physicians/the Society of Critical Care Medicine [23]. Patients who lived for more than 28 days after admission were considered survivors.
Laboratory protocol
An electrochemiluminescence immunoassay (ECLIA) B.R.A.H.M.S. PCT ELECSYS® was used for rapid measurement of PCT with an automated Roche Elecsys and Cobase immunoassay analyzer according to the manufacturer's instructions [24]. This new assay is more sensitive than conventional assays, with a sensitivity of 0.02 ng/mL. The WBC and leukocyte counts, serum albumin, and CRP were monitored using an automatic nephelometer (Beckman Coulter, Pasadena, CA). The lower limit of detection was 3.45 mg/L, and the normal range for albumin was 35.0 to 50.0 g/L.
Clinical data collection
We first used the hospital electronic medical record system to search for patients in the ICU having acute ICH between January 2010 and May 2018. Then, the electronic health records of the patients were viewed. Data, including demographics and existing complications such as chronic lung diseases, diabetes, and renal failure, were recorded as were diagnoses, clinical and laboratory findings, pathogens, 28-day survival, complications, and length of ICU stay, as well as the data needed to evaluate the Acute Physiology and Chronic Health Evaluation II (APACHE II) score were collected. Positive blood cultures were classified as contaminants or true bacteremia. This study included only cases of bacteremia that were considered clinically significant BSIs.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation (SD), non-parametric continuous variables are given as the median and interquartile range (IQR), and categorical variables are shown as numbers and percentages describing basic characteristics. The Student t-test or Mann-Whitney U-test was applied for continuous variables and the χ2 test for between-group comparisons of categorical variables. Multivariable regression analysis was performed to determine whether the variables were independent factors for nosocomial BSI. SPSS 18.0 software was used for all statistical analyses, and a two-tailed p value <0.05 was considered indicative of statistical significance; all confidence intervals (CIs) given are 95%. The area under the receiver operating characteristic (ROC) curve and a cut-off value were used to assess the prediction accuracy.
Results
Patient demographics
A total of 170 patients with ICH were included. Eight-five patients with BSI were treated as the BSI group, and 85 ICH patients without BSI were identified as the without-BSI group. Approximately 70% of our patients had a central venous catheter during the entire ICU stay.
There were several potential factors predisposing patients to nosocomial BSI, including shock during hospitalization, use of antibiotics within 90 days before admission, requirement for a blood transfusion during hospitalization to maintain organ function, and having a DVC or peripherally inserted central catheter in place. The mean incidence density per ICU was 1.63 BSI episodes per 1,000 patient-days. The average age of the patients was 57 years, ranging from 18 to 80 years. There were 92 men. The statistical data and clinical characteristics of the patients are shown in Table 1. Thirty-eight patients (22.4%) had more than two co-morbid diseases at admission, and 65 patients (38.2%) were in shock at some time during hospitalization. In addition, 28 patients died, for a crude mortality rate of 16.5%. The WBC and leukocyte counts and PCT concentration of the patients with BSI were significantly higher than those of patients without BSI, but the albumin concentration was significantly lower. The CRP concentration did not differ between patients with and those without BSI. Among the biomarkers, the albumin:PCT ratio on admission was dramatically lower in patients with BSI than in those without (11.739 [3.192–38.452] versus 200.000 [40.634–417.500]; p < 0.001) (Table 1).
Baseline Features of Patients with Spontaneous Intra-Cerebral Hemorrhage
alb = albumin; APACHE II Score = Acute Physiology and Chronic Health Evaluation II score; CRP = C-reactive protein; GCS = Glasgow Coma Scale; INQ = interquartile range; Neu = neutropenia; PCT = procalcitonin; SD = standard deviation; WBC = white blood cell count.
Albumin:PCT ratio as an independent predictor of BSI in patients with ICH
In a univariable logistic regression analysis, admission Glasgow Coma Scale (GCS) score, PCT, albumin, WBC count, shock, leukocyte count, and albumin:PCT ratio were significantly related to BSI. Furthermore, multivariable logistic analysis revealed that the albumin:PCT ratio (odds ratio [OR] 1.006; 95% confidence interval [CI] 1.002–1.011; p = 0.001], WBC count (OR 1.129; 95% CI 1.044–1.220; p = 0.002), and shock (OR 4.504; 95% CI 1.774–11.435; p = 0.002) were independent predictors of nosocomial BSI, allowing differentiation of patients with such infection from those without (Table 2).
Univariable and Multivariable Logistic Analyses for Discriminating Nosocomial Blood Stream Infection in Spontaneous Intra-Cerebral Hemorrhage
Alb = albumin; APACHE II score = Acute Physiology and Chronic Health Evaluation II score; CI = confidence interval; CRP = C-reactive protein; GCS = Glasgow Coma Scale; LOS = length of stay; Neu = neutropenia; PCT = procalcitonin; WBC = white blood cell count.
Diagnostic performance of the albumin:PCT ratio
The area under the ROC curve (AUC) was used to evaluate the predictability of BSI presence in patients with ICH (Fig. 1). The AUC for the albumin:PCT ratio was 0.830 (95% CI 0.768–0.892; p < 0.001) and was significantly higher than that for the WBC count (0.285 [95% CI 0.208–0.362; p < 0.001]) or leukocyte count (0.363 [95% CI 0.278–0.447; p < 0.001]) (Fig. 1). Moreover, the cutoff value of the albumin:PCT ratio was <1.087 with a sensitivity of 90.6% and a specificity of 98.8%.
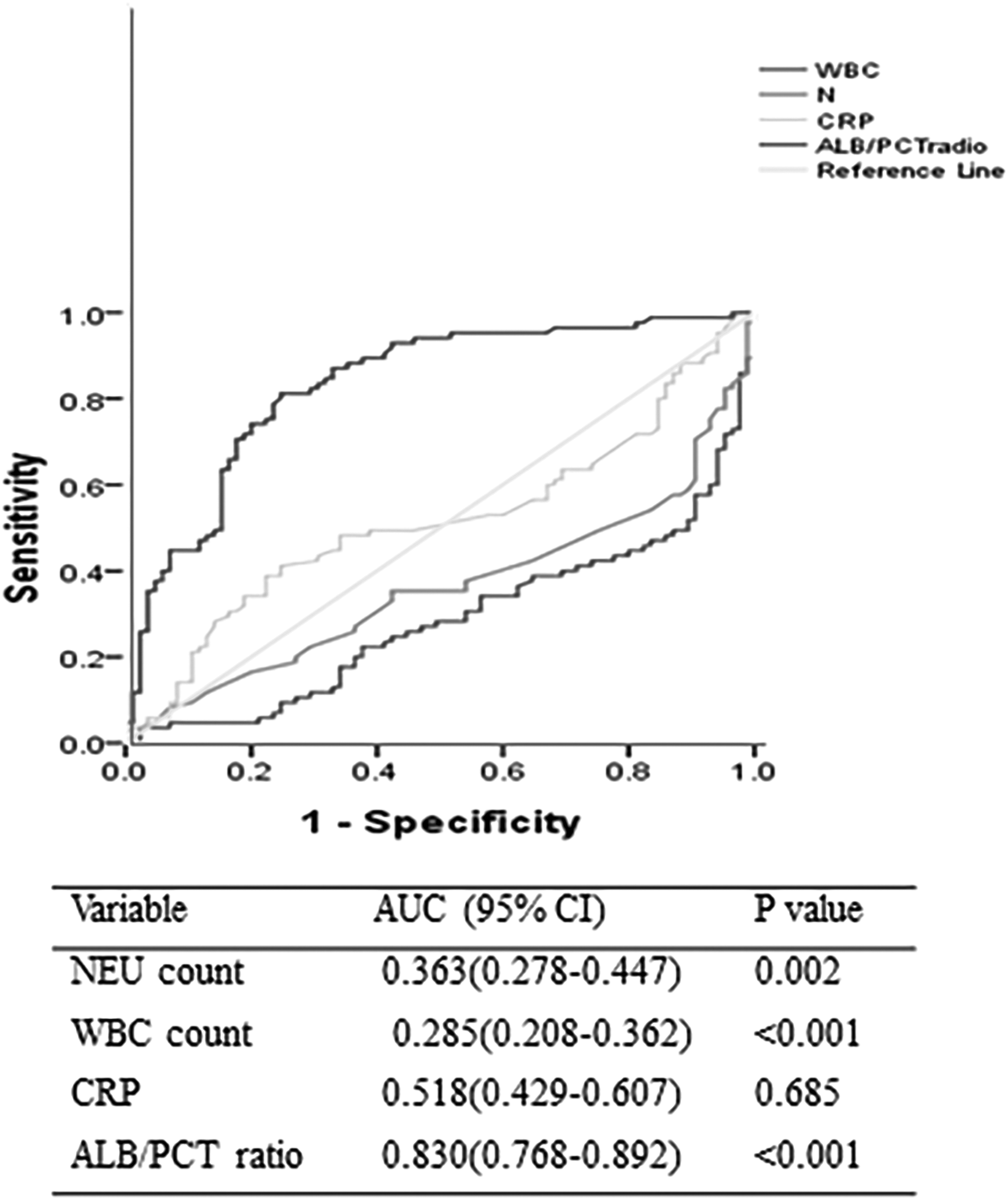
Receiver operating characteristic (ROC) curve of markers for discriminating blood stream infection (BSI). Alb = albumin; CI = confidence interval; CRP = C-reactive protein; PCT = procalcitonin.
Microbiological features
An ICU-acquired BSI was recorded in 85 patients. Of all the microbial episodes, 41% were caused by gram-negative organisms and 40% by gram-positive organisms. Fifteen percent of all episodes of BSI were polymicrobial, and fungi were isolated in 2% of episodes. The rank order of the major pathogens is shown in Fig. 2. Coagulase-negative staphylococci (CoNS) accounted for one-third of all infections (33%). Klebsiella spp. and Acinetobacter baumannii were the most common gram-negative organisms. The proportion of Staphylococcus aureus isolates and CoNS with methicillin resistance was 100%. Vancomycin resistance was not observed in enterococci. Both A. baumannii and Klebsiella spp. were multi-drug resistant. Sixteen of the patients with nosocomial BSIs died during hospitalization, a crude mortality rate of 30%.

Rank order of major pathogens in patients with blood stream infection.
Subgroup analysis
Additional analyses were performed to determine whether the albumin:PCT ratio was associated with BSI severity. A separate analysis was performed involving only patients with BSI (n = 85). In this subgroup, the PCT concentrations were significantly higher, whereas the albumin concentrations were significantly lower in the shock group than in the group without shock. The mean concentrations of albumin were 30.5 ± 6.3 g/L in the shock group and 33.9 ± 6.4 g/L in the without-shock group. The albumin:PCT ratio in patients with shock was lower than that in patients without shock (7.154 [2.975–26.267] versus 28.000 [3.818–57.812]; p = 0.027) (Table 3).
Baseline Features of Patients with Blood Stream Infection in Subgroup Analysis
Alb = albumin; APACHE = Acute Physiology and Chronic Health Evaluation; CRP = C-reactive protein; GCS = Glasgow Coma Scale; INQ = interquartile range; Neu = neutropenia; PCT = procalcitonin; SD = standard deviation; WBC = white blood cell count.
Discussion
This study is the first to explore the utility of the ratio of albumin to PCT for discriminating patients with BSI among patients with ICH in a comprehensive ICU dataset. The main finding was that the initial albumin:PCT ratio compared with the traditional and widespread biomarkers of systemic infection, such as CRP concentration and WBC and leukocyte counts, can be considered an early diagnostic predictor for discriminating patients with BSI from those without a significantly higher AUC value. In addition, a lower albumin:PCT ratio in patients with ICH at admission is indicative of a higher risk of septic complications.
C-Reactive protein is an acute inflammatory protein, but the reaction that results in an elevated CRP concentration in response to inflammation often takes a long time. The dynamic change in CRP is slower in ICH than in other conditions; the elevation is sustained for three days, and the initial CRP concentration is not correlated with active infection [25,26]. Another study showed a rapid increase in the plasma concentration of CRP in patients with ICH, and higher CRP concentrations were associated with a higher mortality rate and worse functional prognosis at 30 days [27]. These findings may be explained by the low sensitivity of CRP and its responsiveness to early non-infectious inflammation. After multivariable logistic regression analysis adjusted for age and gender, the CRP value was not an independent early diagnostic predictor of BSI in patients with ICH.
Some studies have shown that elevated WBC counts at admission are not an independent prognostic variable for acute ICH [28,29]. In patients with acute ICH, a higher neutrophil count predicted worse three-month outcomes [30], and the neutrophil–lymphocyte count ratio was previously considered a predictor of bacteremia [9]. In the present study, WBC and neutrophil counts were independent predictors of nosocomial BSI, but the AUCs for the two counts were 0.285 and 0.363, respectively, meaning a low sensitivity and specificity for BSI diagnosis.
Systemic traditional and widespread biomarkers, such as CRP and WBC, generally are considered useful for the diagnosis of sepsis and are used together with blood cultures. Because culture results take anywhere from 24 to 72 hours to obtain, this method is not appropriate for early diagnosis. Delays in diagnosis are detrimental to a patient's health; and therefore, it is necessary to find faster and more effective diagnostic methods.
The PCT can predict accurately the presence of bacteremia and the bacterial load in BSI, and it is recommended to use PCT quantitatively in the evaluation of bacterial infection and sepsis in critically ill patients, as it may help to predict bacteremia [9–11]. He and colleagues demonstrated that an elevated PCT concentration at admission was associated with adverse clinical outcomes in patients with ICH [31]. Procalcitonin proved to be the most reliable predictor of BSI, with Neu being the second most reliable predictor; and the PCT concentration in patients with gram-negative BSI was higher than that in patients with gram-positive or fungal BSI [11]. We also found that the CRP, WBC, Neu, and PCT concentrations of patients with BSI were significantly higher at admission than those of patients without BSI. The higher PCT concentration could have been attributable to any of several causes. For example, most patients with BSI have gram-negative bacterial infections, which result in a higher PCT peak than do gram-positive infections. Also, monitoring the serum PCT concentration is an effective antimicrobial management strategy to differentiate bacterial infections from non-infectious inflammatory conditions. In ICU patients with infection and sepsis, PCT-guided antibiotic therapy improves survival and shortens antibiotic treatment duration [32]. Evidence suggests that PCT monitoring is cost-effective as long as the test is ordered judiciously [12].
In the past, the serum albumin concentration was considered an indicator of nutritional status; however, recent literature suggests that the protein is associated with disease severity and the mortality rate. Albumin is a powerful marker of clinical disease outcomes because its concentration tends to decline during acute-phase infections [16–18]. Albumin thus has been used to direct the treatment of a variety of diseases. The exact mechanism of its elevation is unclear, although it could include several actions. Albumin can cause elevated serum oncotic pressure, thereby attracting interstitial fluid and improving organ perfusion. In addition, albumin has significant anti-oxidant properties, which can improve micro-circulatory blood flow and reduce leukocyte adherence, thus producing anti-inflammatory effects [33]. Hypo-albuminemia is a common symptom of acute ischemic stroke and is associated with the severity and adverse clinical outcomes [17,34]. Moreover, hypo-albuminemia may be associated with inflammatory changes during sepsis or may reflect poorer baseline nutrition. Albumin is known for its wide range of endogenous ligands and drug transporters, as well as its role as an effective anti-oxidant and anti-inflammatory agent [35]. Therefore, in the case of hypo-albuminemia, these protective biological functions may be impaired, leading to increased morbidity and mortality rates in patients with severe sepsis. This theory is consistent with our findings, as the albumin concentration in patients with BSI was significantly lower at admission than in patients without BSI. In addition, the albumin concentration decreased significantly as the infection worsened. This observation is consistent with a report by Falguera et al. [36] indicating that low serum albumin is a predictive factor for patients with infections such as community-acquired pneumonia.
The PCT is strongly associated with albumin, and PCT positivity together with albumin negativity is a prognostic factor in elderly persons at risk for bacterial infection [37]. The findings of Luo et al. suggested that the PCT/albumin ratio was a fast and relatively cheap biomarker that can be used as an early predictor to distinguish patients with urosepsis from those with febrile UTI [38]. Thus, PCT and albumin were combined to improve the potential predictive capabilities of each single factor. Combining these two markers with inflammatory and nutritional factors can improve their predictive value. We hypothesized that the albumin:PCT ratio was a better predictor than other indicators of inflammation or nutrition. In the present study, the initial albumin:PCT ratio was significantly lower in patients with than in patients without BSI. In addition, as expected, BSI patients with shock had significantly lower blood pressure than those without shock. Therefore, we speculated that the albumin:PCT ratio reflected the severity of infection. The PCT concentration is thought to be associated with infection but sometimes remains low during infection and becomes elevated in non-infectious conditions. The albumin concentration tends to decrease in patients with infection. Therefore, we combined the two biomarkers to improve the sensitivity and specificity for diagnosis of BSI before the onset of hypotension. Our results suggest that the albumin:PCT ratio is a useful predictor of BSI in patients with ICH making it unnecessary to wait for blood culture results.
The current study has several limitations. First, it was retrospective, which may have introduced bias. Second, the sample was small. Furthermore, this investigation was a single-site study, and the results may differ from those of other centers. Finally, the probability of prediction may be overestimated compared with prospective studies. Further analysis is warranted.
Conclusion
The study showed that the albumin:PCT ratio could be an early diagnostic predictor for nosocomial BSI in patients with ICH. In addition, BSI patients with lower albumin:PCT ratios are more likely to experience shock. The albumin:PCT ratio is expected to be a rapid and low-cost tool for clinical practice.
Footnotes
Acknowledgments
This work was supported by grants No. 18140901100, 17140900203, and 20184Y0064.
We thank the Critical Care Medicine staff for their support of this study.
Author Disclosure Statement
None of the authors has a competing financial interest with regard to this research.