
Abstract
Abstract
Background:
There is a lack of evidence-based recommendations for surgical hand washing when there is a minor cut on the hand. We sought to evaluate whether two-layer wound sealing functions as a barrier to prevent the spread of micro-organisms.
Methods:
We randomly categorized 20 surgeons into subjects with either a right- or left-hand injury. Each subject was assumed to have a minor injury on the assigned hand and the other hand was used as a control. Subjects applied a waterproof topical dressing as a first layer, then protected the injured area with a second layer using an antimicrobial drape, and finally performed surgical hand rubbing. Subjects stamped each hand onto an agar plate. The injured hands were checked by an investigator to confirm the wounded area remained properly sealed after hand rubbing. Colonies were counted and the micro-organisms were identified after 48 hours of incubation.
Results:
There was no leak found from two-layer wound sealing after hand washing. Mean number of the colonies was 0.2 on the injured hand and 0.25 on the uninjured hand (p = 0.772). The micro-organisms cultured from both the injured and uninjured hands were coagulase-negative staphylococci.
Conclusions:
Using a model for a minor cut injury on the hand this study demonstrated that two-layer wound sealing is an effective barrier not only to prevent the spread of micro-organisms but also to protect surgeons.
Surgical site infections (SSIs) increase the length of hospital stay, rehospitalization rates, and medical costs; they are also one of the leading causes of increased morbidity and mortality after surgery [1–3]. To reduce SSIs, proper hand washing by the surgical staff before any surgical procedure is important [4–7].
As a result of the use of sharp surgical instruments, accidental injuries to surgeons' hands are inevitable [8,9]. Moreover, cut injuries on the hands are common during normal daily life outside of the hospital [10,11]. A large proportion of these injuries are minor superficial cut injuries, for which treatment with a simple wound dressing for a few days is sufficient.
Because of the importance of proper hand washing before surgery to prevent SSIs, there have been many studies to elucidate how the surgical hand washing should be performed [4–7]. However, to the best of our knowledge, no study has demonstrated pre-operative hand washing of injured hands.
The purpose of this study was to evaluate whether two-layer wound sealing is effective to protect surgeons and to investigate the effect of the two-layer wound sealing in preventing micro-organism colony formation. We hypothesized that two-layer wound sealing would function as a barrier to protect the surgeons' hands and to prevent the spread of micro-organisms.
Materials and Methods
A randomized prospective study was performed at the authors' institution. The Institutional Review Board of our hospital reviewed the protocol and approved the study (B-1609-361-302). A total of 20 surgical staff volunteers from the orthopedic department of our institution were enrolled to provide 20 injured and 20 uninjured hands. A previous study that used the hand stamp method to identify colony-forming unit (CFU) changes after hand washing with alcoholic solution found that the mean CFU changed from 75 ± 39 to 9 ± 11 after hand washing [12]. On the basis of this value, we designed the present study to identify 50% difference in the colony count between the injured and uninjured hands, with a standard deviation of 37 (for an effect size of 1.0). Power analysis indicated that a sample size of 12 patients would provide a statistical power of 80% at a two-sided 5% type I error to detect this effect size between the injured and uninjured hands using the paired Student t -test.
To be eligible for inclusion in the study, the volunteers could not be currently using any antibiotics; could not have any kind of dermatologic conditions or injuries or deformities of the hands; and could not have a history of sensitivity to either ethyl alcohol or chlorhexidine gluconate. Of the 20 participants, 17 were residents and three were clinical fellows. All participants provided informed consent. None of the participants dropped out of the study and none of the laboratory results were contaminated. Baseline characteristics of the subjects are provided in Table 1. Clinical characteristics such as age, gender, and dominant hand were obtained from a self-reporting questionnaire. For the dominant side hand, the questions asked were: “Which hand do you use for writing?” and “Which hand do you use for throwing a ball?” If different answers were received we then asked “Which is your dominant hand?” for confirmation.
Baseline Characteristics of the Participants
The values are given as the number of subjects, with the percentage in parentheses.
The values are given as the mean, with the range in parentheses.
The volunteers' hands were screened by two investigators one day before the experiment to determine eligibility. When 20 volunteers were confirmed to have been enrolled, they were randomly assigned to one of two groups: the right-hand injured group or the left-hand injured group. Each subject was assumed to have a minor injury on the volar surface of the index distal phalanx of one hand. The other uninjured hand was used as a control. As a result of random assignment, 11 subjects were assigned to have an injury on their dominant hand.
Before the experiment, subjects were asked to remove all jewelry from both hands and forearms. Subjects clipped the fingernails up to a less than 1 mm free edge and cleaned under the fingernails of both hands with a nail cleaner. After the fingernails were cleaned, an investigator applied a 1.5 cm diameter circular-shaped waterproof topical dressing (DuoDERM Extra Thin Dressing, ConvaTec, Greensboro, NC) on the volar surface of the distal phalanx of the index finger of the injured hand [13; Fig. 1a).The injured finger was then washed using 100 mL of a solution product (Greenhexidiol solution, Green Pharmaceutical, Seoul, Korea) containing 2.5 mL of chlorhexidine gluconate and 75 mL of 96% ethyl alcohol. The subjects waited for 90 seconds until the injured finger had dried completely. To obtain two-layer wound sealing, we used antimicrobial incise drape (Ioban™ 2, 3M Heath Care, St. Paul, MN) to wrap around the injured phalanx (Fig. 1b). The entire distal phalanx as well as the distal interphalangeal joint of the injured finger was completely covered. After sealing the wound, each subject performed hand rubbing using a product containing 1% chlorhexidine gluconate and 61% ethyl alcohol by weight (3M Avagard Surgical and Healthcare Personnel Hand Antiseptic with Moisturizers; 3M Heath Care, St. Paul, MN) [14]. Three aliquots of 2 mL were used each time to wash the hands and forearms. Subjects rubbed their hands according to the corresponding manufacturer's label instructions for longer than three minutes until the hands had completely dried under the supervision of an investigator [15].
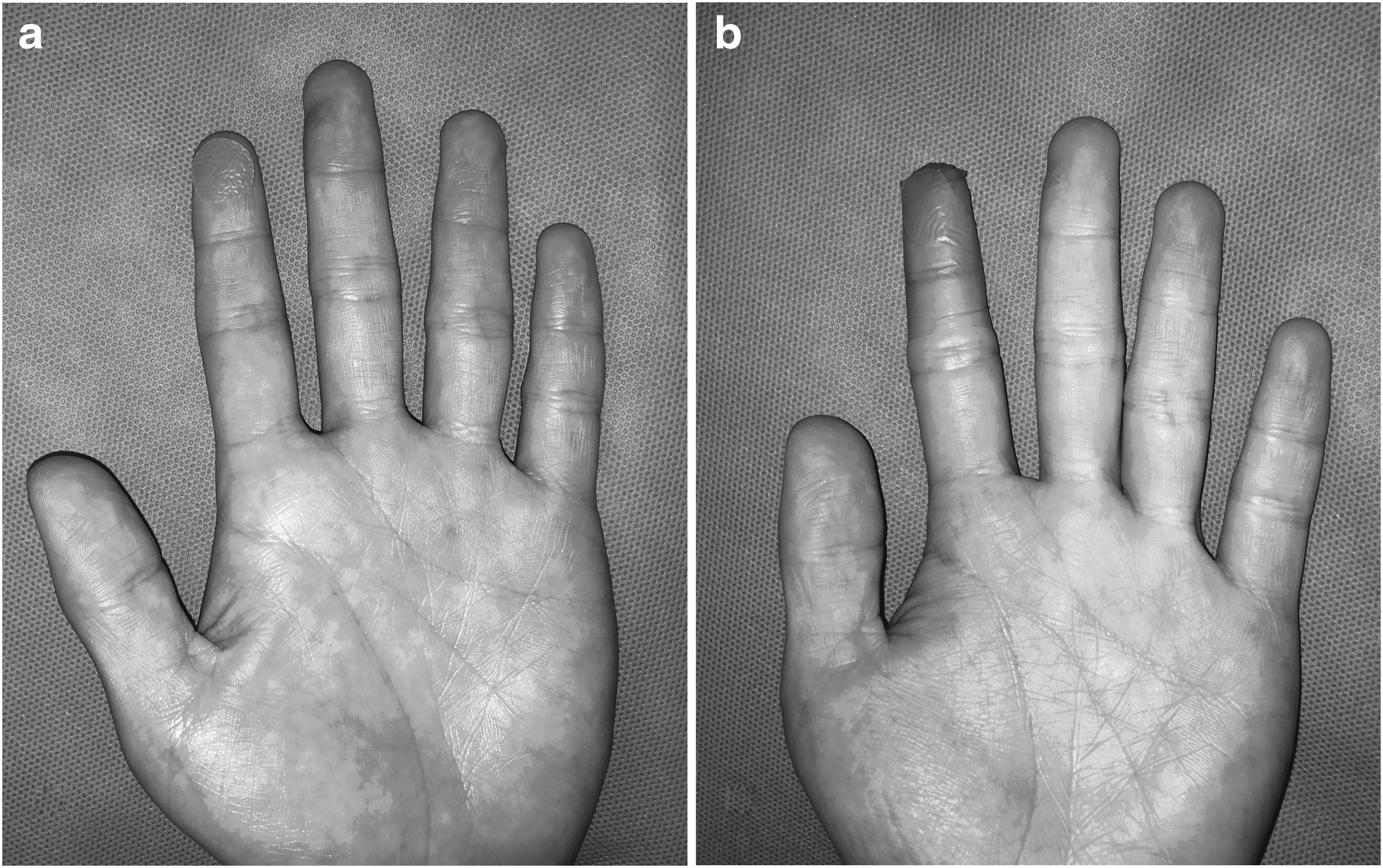
(
We used a direct agar contact plate method (hand stamp method) to collect samples of micro-organisms [12,16–18]. Specifically, micro-organisms were cultured using a hand-shaped blood agar plate (Easy Checker TPC, Hanil Komed, Sungnam, Korea) to localize the colonies [19]. Within five minutes after application of the hand rub, subjects stamped each hand on an agar plate for 10 seconds in a uniform manner according to the instructions in the manual (Fig. 2). Two agar plates were used per subject to perform the hand stamp method of the injured hand and the uninjured hand separately on each agar plate. After performing the hand stamp method, an investigator removed the dressing from the injured hand of the participants to check whether the wounded area remained properly sealed after the entire hand washing procedure. The agar plates were sent to the microbiology laboratory immediately after collection in a blinded manner. Mean time from hand stamp sampling to incubation was 32 minutes. All culture plates were incubated aerobically at 35°C and were observed for microbial growth for 48 hours. If any growth was observed, standard laboratory identification procedures were used to identify organisms to the species level and colony-count determinations were made.

Hand stamp method using Easy Checker TPC (Hanil Komed, Sungnam, Korea) is shown.
Colony counts on the injured hand and the uninjured hand were compared using paired Student t-test. Independent t-test was used to determine whether hand dominance affects the colony forming unit (CFU) of the injured hand. We used SPSS statistical software (version 15.0, SPSS Inc., Chicago, IL) for all statistical analyses and considered p < 0.05 as statistically significant.
Results
There was no leak found from wound sealing in the participants when the dressing was removed and examined by an investigator after the hand stamp method. After 48 hours of incubation, the mean number of colonies formed on injured hands and uninjured hands were 0.20 ± 0.55 and 0.25 ± 0.70, respectively. We found four colonies on 20 injured hands, however, all of these colonies were found at locations other than the wounded area. When compared using paired Student t-test, there was no difference in number of colonies formed between injured hands and uninjured hands (p = 0.772). Standard laboratory identification procedures revealed that the micro-organisms cultured from injured hands and uninjured hands were coagulase-negative staphylococci including Staphylococcus hominis, Staphylococcus capitis, Staphylococcus heamolyticus, and Staphylococcus xylosus. There was no substantial effect of hand dominance on the CFU of the injured hands (p = 0.221).
Discussion
Regarding the prevalence of minor skin damage on surgeon's hands, it is not feasible to prevent every surgeon with a minor cut injury on the hand from participating in surgery. However, it has been demonstrated that damaged skin can alter the bacterial flora on the hand, which might contribute to the spread of unusual micro-organisms [20]. Moreover, surgical gloves are easily perforated during surgery and are not a secure barrier between the patient's body fluid and the surgeon's hand [21,22]. Therefore, to protect not only the patient but also the surgeon from pathogen transmission, proper sealing of the wound is crucial. Our results suggest that the proposed two-layer wound sealing can be an effective method for surgeons with a minor cut injury on the hand.
Using two-layer wound protection, all wounds were sealed securely after hand washing. To accomplish secure wound protection, the following considerations were made during the two-layer wound sealing procedure. As the first step of the procedure, we used a topical dressing that enhances wound healing because it is waterproof [12]. Second, we used a solution containing 2.5 mL of chlorhexidine gluconate and 75 mL of 96% ethyl alcohol to wash the injured finger before affixing an antimicrobial incise drape. There were two reasons for using this, i.e., the microbicidal effect and the effect of ethyl alcohol on dissolution and removal of fatty acids from the skin that helps surgical drapes to attach firmly to the skin. Third, the incise drape used for two-layer wound sealing is not only waterproof but it also contains iodophor complex in the adhesive that is antimicrobial [23]. Last, after sealing the wound, the subjects performed hand rubbing instead of scrubbing. Although certain SSI pathogens are prone to develop in alcohol-based hand rubs [24], there are studies suggesting that hand rubbing using an alcohol-based product is more effective than hand scrubbing using a brush [4,25–29]. Moreover, hand scrubbing using a brush might cause damage to the wound sealing products as it causes damage to the skin [30,31]. We used a U.S. Food and Drug Administration-approved alcohol-based waterless product as a rubbing agent because it was shown to be more effective than other alcohol-based water aided products [32].
Our study found no substantial difference between the injured hand with two-layer wound sealing and the uninjured hand in the number of colonies as well as the species of micro-organisms formed after surgical hand washing. Although there has never been a study regarding surgical hand washing of an injured hand, a previous study has evaluated the effect of nail polish on the number of bacterial CFU left on hands after pre-operative surgical scrubbing [33]. No difference was found in the number of bacteria on hands after surgical scrubbing between the subjects with nail polish and the subjects without nail polish. Those results suggest that if a foreign material is firmly attached to the hand, it may not increase the risk of contamination after surgical hand washing.
There are some limitations to our study. First, since we assumed that the wound was located on the volar surface of the index distal phalanx, our results might not represent minor cut injuries at other locations on the hand. For the study purpose, we selected a part of the hand where the injuries occur most frequently during surgery [8]. Second, the hand stamp method is limited to only one surface of the hand. To evaluate the entire surface of the hand, the glove juice method or the bag broth technique is appropriate [3]. However, in our study, we used the hand stamp method to localize the colonies to determine whether these colonies are obtained from the injured area of the hand. Third, our study did not show the delayed effect, i.e., the change in integrity of the wound sealing that might occur within hours after hand washing. However, the hand rubbing product that we used in this study is known to have a prolonged antimicrobial effect [13]. Last, we could not measure the comfort of the surgeon and mobility of the index finger with the sealant in a glove. Despite the limitations, it is noteworthy that this is the first study to propose an effective way of hand washing before surgery for surgeons with a minor cut injury on the hand.
Conclusions
We conclude that two-layer wound sealing is an effective barrier to protect patients as well as surgeons. For further verification of the validity of two-layer wound sealing method, prospective studies with larger number of injured hands using the glove juice method are needed.
Footnotes
Acknowledgments
The Seoul National University Bundang Hospital Institutional Review Board (SNUBH IRB) reviewed the protocol and approved the study (B-1609-361-302). All participants provided informed written consents.
The datasets used and/or analyzed during the current study are available from the corresponding author on request. The authors received no financial support for the research, authorship, and/or publication of this article. All authors read and approved the final manuscript.
Trial Registration: SNUBH Registry 1609-361-302 Registered September 1, 2016.
We would like to thank all the residents and clinical fellows who took part in the study voluntarily.
Author Disclosure Statement
The authors declare that they have no competing interests.