
Abstract
Abstract
Background:
Surgical site infections (SSIs) remains a concern for surgeons because of the negative impact on outcomes and health care costs. Our purpose was to assess whether topical antibiotics before primary incision closure reduced the rate of SSIs.
Methods:
Systematic review of MEDLINE/PubMed, Scopus, CINAHL, and Web of Science databases from inception to January 2017. Only randomized controlled trials (RCTs) were retrieved. The primary outcome was the SSI rate. Meta-analysis was complemented with trial sequential analysis (TSA).
Results:
Thirty-five RCTs (10,870 patients) were included. Only β-lactams and aminoglycosides were used. A substantial reduction of the incidence of SSIs with the application of antibiotic agents before incision closure (risk ratio [RR] 0.49, 95% confidence interval [CI] 0.37–0.64) was found, which remained in the analysis of 12 RCTs after removal of studies of uncertain quality. The use of β-lactams was effective to reduce SSI in elective surgery only (RR 0.33, 95% CI 0.13–0.85). In clean-contaminated fields and as an irrigation solution, β-lactams did not reduce the risk of SSI. Aminoglycosides were not effective (RR 0.74, 95% CI 0.49–1.10). After TSA, the evidence accumulated was far below the optimal information size. The heterogeneity of studies was high and methodological quality of most RCTs included in the meta-analysis was uncertain.
Conclusions:
Results of this meta-analysis show the data present in the literature are not sufficiently robust and, therefore, the use of topical β-lactams or aminoglycosides before incision closure to reduce SSI cannot be recommended or excluded.
Surgical site infections (SSIs) are among the most frequently reported health-care–associated infections leading to worse patient outcomes and increased costs [1]. Classification of SSIs proposed by the U.S. Centers for Disease Control and Prevention (CDC) including incisional, deep incisional, and organ/space infection is probably the most widely used [2]. An SSI is frequently defined as one that occurs within 30 days of the operative procedure and involves the skin or deep tissue of the incision [2]. At least 5% of patients undergoing a surgical procedure develop an SSI [3]. However, the incidence of SSIs varies largely depending on a number of factors, such as the type and frequency of surgical procedures, the context in which operations are performed, the surveillance criteria used, and the quality of data collection. For example, post-cesarean delivery SSIs in rural areas of resource-limiting countries account for up to one-third of all surgeries [4], with reported incidence rates of 42.8% in this setting [5].
Given the burden of SSIs worldwide, the numerous gaps in evidence-based guidance, and the need for standardization, international bodies including the World Health Organization (WHO) [6,7] and the CDC [8,9] have developed guidelines for the prevention of SSIs. Interventions before primary closure of the surgical incision have been suggested, and some of them such as pre-operative administration of intravenous antibiotic agents are accepted fully [7,8]. Topical application of antibiotic agents has been used for decades in surgical practice [10], although consistent recommendations regarding the effectiveness of this measure are lacking. According to WHO guidelines [7], irrigation of the incision with antibiotic agents before closure should not be used. CDC guidelines also advice against application of ointments, solutions, or powders at the site of the incision, but irrigation with antibiotic agents (e.g., intra-abdominal, deep, or subcutaneous tissues) remains an unsolved question [8]. Moreover, the antibiotic agents that should or should not be used are not specified.
The use of topical antibiotic agents before incision closure to prevent SSIs is applicable to multiple surgical procedures, in urgent or elective operations, and in the form of irrigation solutions, powders, injections, carriers (collagen implants), or other modalities [6–8]. Considering these different perspectives, the question of whether topical antibiotic agents before primary closure are beneficial to prevent SSIs has not been answered in any previous meta-analysis. Therefore, a meta-analysis of randomized controlled trials (RCTs) on this topic was conducted to provide strong evidence that could justify the recommendation of application of antibiotic agents on the incision before primary closure to prevent SSIs effectively.
Methods
This meta-analysis was carried out according to the predefined methodological approach outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [11]. The protocol was registered in the PROSPERO database in February 2017 (registration number CRD42017056644, available at: www.crd.york.ac.uk/PROSPERO).
Systematic literature search
We conducted a systematic literature search of MEDLINE/PubMed, SCOPUS, CINAHL, and Web of Science databases using MeSH terms and text words from inception until January 31, 2017. Search terms included “antibiotics” OR “antimicrobials” OR “antibacterial” OR “anti-infective” OR “topical” AND “surgical wound infection” OR “wound infection.” The search was limited to randomized controlled trials (RCTs) using a maximally sensitive strategy. In the case of MEDLINE/PubMed, the following terms were used: (“anti-bacterial agents”[Pharmacological Action] OR “anti-bacterial agents”[MeSH Terms] OR (“anti-bacterial”[All Fields] AND “agents”[All Fields]) OR “anti-bacterial agents”[All Fields] OR “antibiotics”[All Fields]) OR (“anti-infective agents”[Pharmacological Action] OR “anti-infective agents”[MeSH Terms] OR (“anti-infective”[All Fields] AND “agents”[All Fields]) OR “anti-infective agents”[All Fields] OR “antimicrobial”[All Fields]) OR topical[All Fields] AND (“surgical wound infection”[MeSH Terms] OR (“surgical”[All Fields] AND “wound”[All Fields] AND “infection”[All Fields]) OR “surgical wound infection”[All Fields]) OR (“wound infection”[MeSH Terms] OR (“wound”[All Fields] AND “infection”[All Fields]) OR “wound infection”[All Fields]) AND Randomized Controlled Trial[ptyp]. The target was human studies written in English, French, German, and Spanish languages. The references list of all retrieved studies was cross-checked for additional reports. The abstracts of all articles retrieved were reviewed independently by three authors (M.L.-C., A.C., and M.K.) to identify eligible studies.
Study selection, data extraction, and quality assessment
We established the inclusion criteria for study selection according to the PICO (population, intervention, control, and outcomes) approach. The population consisted of patients undergoing colorectal, soft tissue (sinus/hidradenitis), hernia, cardiovascular, biliary tract, breast, miscellaneous abdominal, and trauma surgeries. Patients undergoing eye surgery and those treated with antibiotic-impregnated beds (orthopedic surgery), cements, or antibiotic dressings were excluded. The intervention was the use of topical antibiotic agents at the incision site before primary closure for SSI prevention by means of an irrigation solution, powder, carrier (i.e., collagen implant), incision injection, or other delivery forms. Patients with surgical incisions in which prophylactic topical antibiotic agents were not applied were included in the comparator group (placebo). Comparisons of different topical antibiotic agents or antibiotic agents with antiseptics were excluded.
The primary outcome was the SSI rate after topical antibiotic therapy. Secondary outcomes were SSI rates according to the following parameters: (1) type of antibiotic agent; (2) type of surgery (urgent or elective operations); (3) grade of contamination of the surgical field defined as clean, clean-contaminated, contaminated, and dirty [2]; (4) antibiotic administration mode; and (5) use of topical antibiotic agents with and without associated systemic antibiotic treatment.
Three authors (M.L.-C., A.C., and M.K.) independently extracted data from the included trials. Any divergences during the data extraction phase were resolved through discussion with a fourth investigator (J.M.G.A.).
Methodological quality (risk of bias) was assessed in four specific areas: method of randomization, clear allocation concealment, use of masked outcome assessments, and time of assessment of infection. Depending on whether information on these aspects was present, partially present, or absent, the quality of studies was considered high, low, or uncertain, respectively.
Statistical analysis
For the meta-analysis of the primary outcome parameter, all eligible RCTs were grouped according to the use of the same antibiotic agent. Also, separated meta-analyses were performed for secondary outcomes in the different pre-defined categories and grouping RCTs by the same agent used for SSI prevention. These meta-analyses were performed when more than two RCTs were eligible for a given outcome. A sensitivity analysis was performed to assess the impact of the use of topical antibiotic agents on the global effect according to the best quality of studies (high and low excluding uncertain), and on SSI occurring within 30 days after surgery.
A random effects meta-analysis was used and because data were sparse (number of events and study size) a Mantel-Haenszel statistical method was selected. Peto method was used to verify the results in uncommon outcomes [12]. All outcomes were expressed as risk ratios (RRs) with 95% confidence intervals (CIs). Heterogeneity in the included studies was evaluated using I2 statistics with I2 values of 25%, 25%–50%, and more than 50% corresponding to small, moderate, and high heterogeneity, respectively. P values were also calculated. We examined publication bias by constructing a funnel plot of precision. This meta-analysis was performed using the Review Manager 5.3 software (Nordic Cochrane Centre, Copenhagen, Denmark, 2013).
Sequential multiplicity (repeated updates) and sparse data increased the risk of type I error and to control this we performed a trial sequential analysis (TSA) [13] for the primary outcome. For the present TSA, we estimated the required information size (RIS) using an assumption of 0.05 for type I error and 0.20 for type II error, and the control event rate (CER) was calculated according to published data related to clean-contaminated infection rate (10%) [14] because most of the included RCTs involved clean-contaminated surgical fields. The effect size (relative risk reduction [RRR]) estimated from the included studies was used to estimate the RIS. We used the I2 present in the included trials as the estimate for heterogeneity. The TSA can be interpreted by viewing the boundaries and whether the cumulative meta-analysis has crossed them. The TSA was performed using the TSA software v0.9 (www.uct.dk/tsa/index.htm).
Results
Database searches and additional records identified through other sources revealed 3,699 records. After exclusion of 3,646 irrelevant records, 53 RCTs were eligible. Of these 53 RCTs, 13 were finally excluded because of the use of a comparator other than placebo and 5 because they were single studies using a particular agent for which at least two RCTs were not available. The final study sample included 35 RCTs with a total of 10,870 patients [15–49]. The selection of studies is shown in Figure 1.
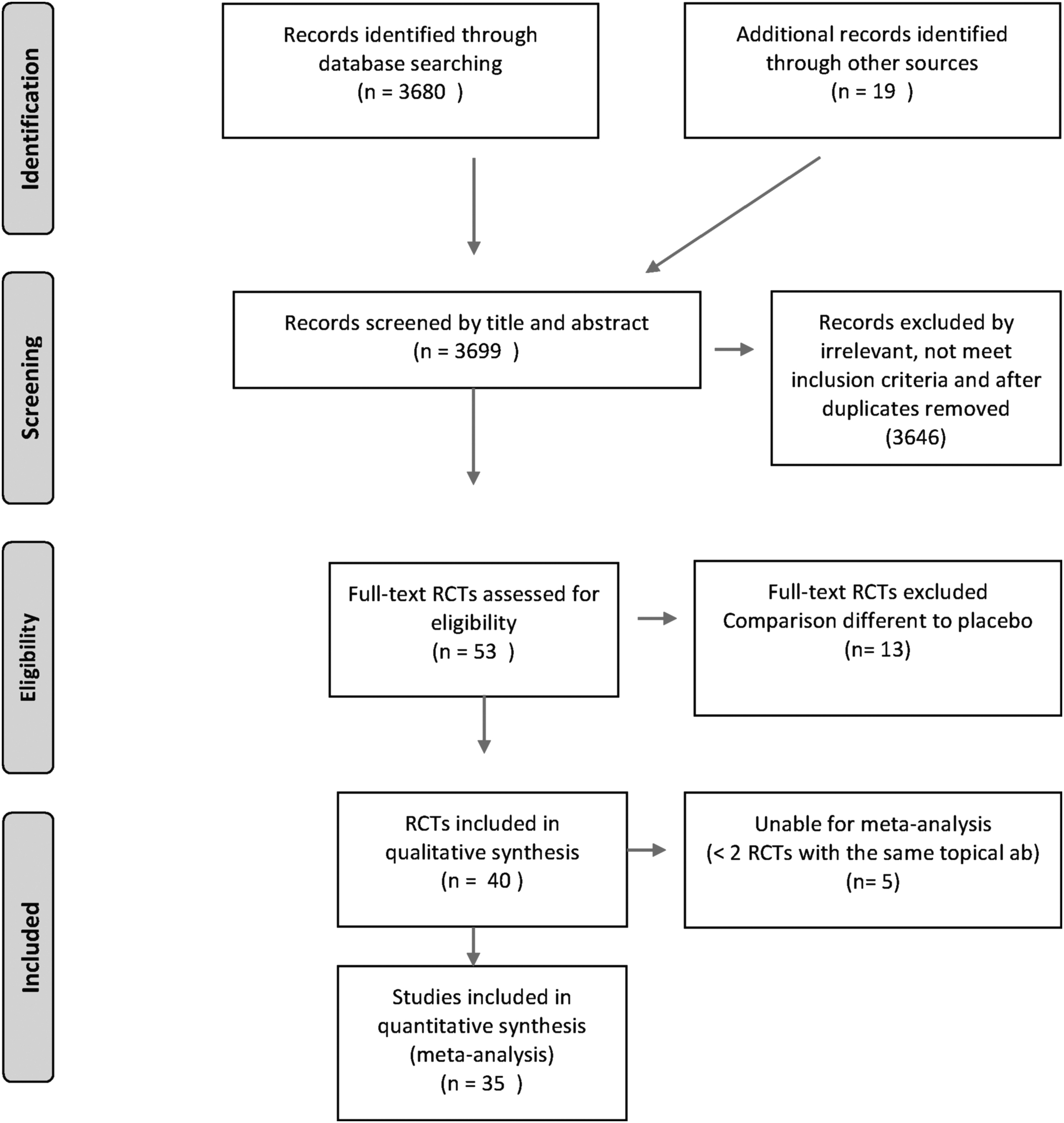
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram.
Randomized controlled trials included in the meta-analysis reported the use of only two antibiotic agents and covered two different time periods: β-lactams in 3,569 patients from the 1960s to 1990s [15–31] and aminoglycosides in 7,301 patients from approximately the 1990s to the present time [32–49]. Urgent surgical procedures were present in 6 RCTs (using β-lactams [16,17,20,23,29,31], and elective operations in the remaining 29 studies using β-lactams in 11 [15,18–22,24,25–28,30] and aminoglycosides in 18 [32–49]. Colorectal surgery was the most frequent type of surgery in which either β-lactams [15–17,19,20,23,27,29,31] or aminoglycosides [32,33,35,37,40,45,48,49] were used, followed by cardiovascular operations in which aminoglycosides were used [38,39,44,47]. For the remaining patients, sufficient information regarding the use of β-lactams was reported only in miscellaneous abdominal operations [18,21,22,28] and regarding the use of aminoglycosides in soft tissue (sinus/hidradenitis) surgeries [34,41,46]. In relation to the grade of contamination, information was available for both β-lactams in clean [24,25,30] clean-contaminated [15,18–22,26–28], and contaminated [16,17,20,23,29,31] surgical fields and aminoglycosides in clean [36,38,39,42,44,47] clean-contaminated [32,33,35,37,40,45,48,49] and contaminated [34,41,46] fields. Antibiotic agents were applied as powders [15–20,22–24,27] and irrigation solutions [21,25,26,28–30] for β-lactams, and with a carrier (i.e., collagen implant) [33–41,43–47,49] and irrigation solutions [32,42,48] for aminoglycosides. Systemic antibiotic agents were mainly associated with topical aminoglycosides [32,33,35–40,44,45,47–49] rather than with β-lactams both in elective [18,22,25,27,28] and urgent (29,31) surgical procedures. The characteristics of RCTs included in the meta-analysis are provided in Table 1. Risk of bias assessments are presented in Table 2.
General Characteristics of Randomized Controlled Trials Included in the Meta-Analysis
Risk of Bias of Randomized Controlled Trials Included in the Meta-Analysis
SSI = surgical site infection; RCT = randomized controlled trial; NS = not stated; seq = sequence.
Primary outcome
The meta-analysis for the primary outcome (SSI rate) included all 35 RCTs (10,870 patients) and demonstrated a substantial reduction of the incidence of SSI with the application of antibiotic agents before primary surgical incision closure (RR 0.49, 95% CI 0.37–0.64). The heterogeneity between studies was high (I2 = 70%). Of the 35 RCTs included in the meta-analysis, 21 [15,17,18,20,23,24,26,27,29–37,39,41–43] were deemed to be of uncertain quality and in 2 low-quality trials [16,22] SSI was assessed within 30 days of the surgical procedure. After removal of studies with uncertain quality and time assessment of infection less tha 30 days, the beneficial effect of the use of topical antibiotic agents was maintained (RR 0.58, 95% CI 0.39–0.86; 12 RCTs, 6,211 patients; I2 = 81%; Fig. 2).
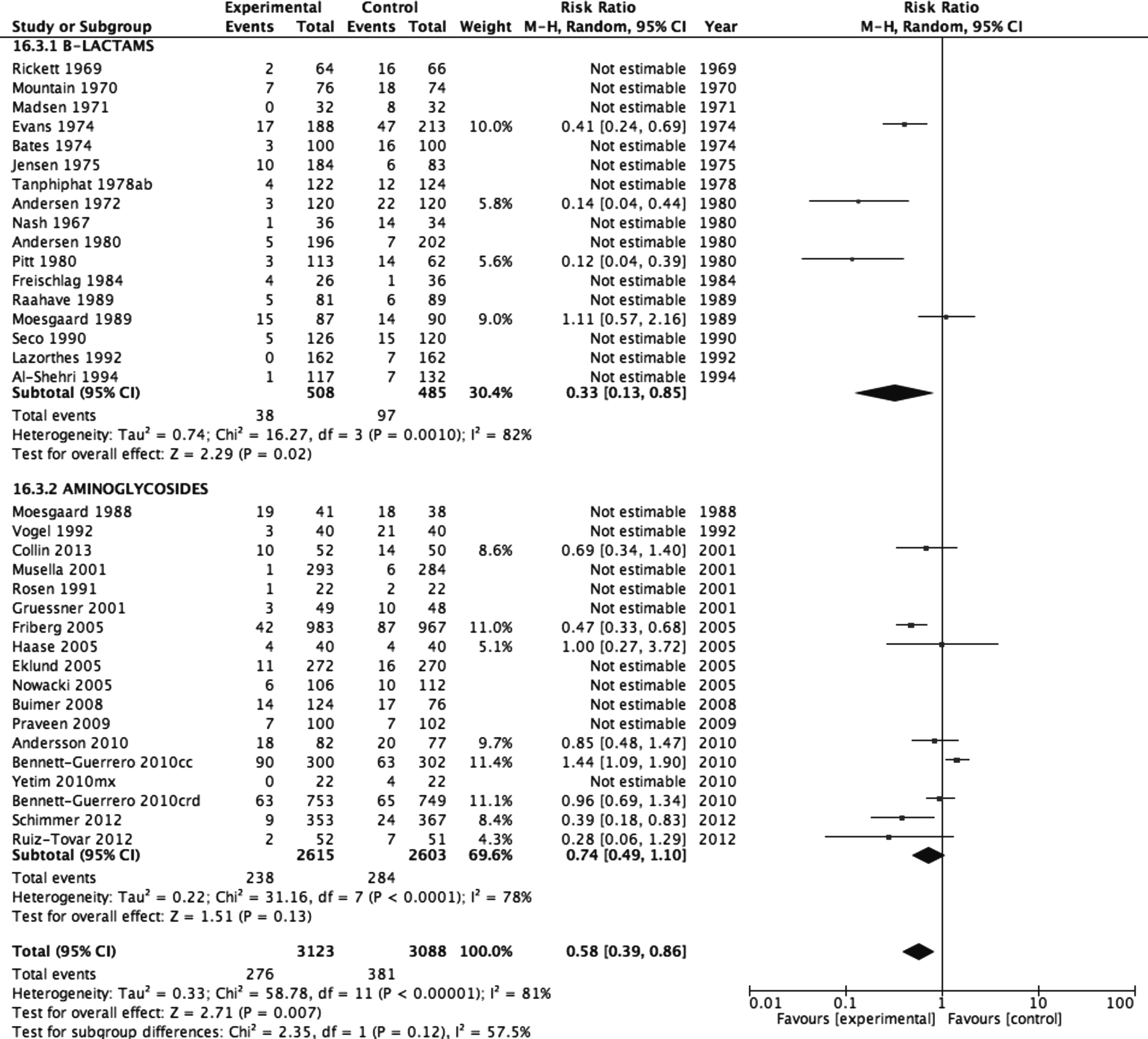
Effect of topical antibiotics for preventing surgical site infection (SSI) after removal of studies with uncertain quality.
Secondary outcomes
A total of 12 RCTs [19,21,25,28,38,40,44–49] with 6,211 patients were included in the meta-analyses for secondary outcomes after removal of studies with uncertain quality and time of assessment of infection less than 30 days. The use of β-lactams was effective to reduce SSI in patients undergoing elective surgical procedures (4 RCTs, 993 patients) [19,21,25,28] (RR 0.33, 95% CI 0.13–0.85; I2 = 82%). In clean-contaminated surgical fields, the use of topical β-lactams was not associated with a reduction of SSI (3 RTCs, 818 patients) [19,21,28] (RR 0.44, 95% CI 0.16–1.19; I2 = 82%). Also, the use of β-lactams as an irrigation solution was not effective to reduce SSI (3 RCTs, 753 patients) [21,25,28] (RR 0.42, 95% CI 0.15–1.18; I2 = 83%). The information available was insufficient to perform meta-analyses of the remaining secondary outcomes, including urgent surgery, associated systemic antibiotic agents, clean and contaminated fields, and other forms of application of β-lactams. The use of topical aminoglycosides (8 RCTs, 5218 patients) [38,40,44–49] was not associated with a reduction of SSI (RR 0.74, 95% CI 0.49–1.10; I2 = 78%). The funnel plot of the RCTs included in the analysis [19,21,25,28,38,40,44–49] did not show publication bias.
For the primary outcome (SSI rate) and for the use of β-lactams, the TSA estimation using a RRR of 67% and a CER proportion of 17% with a constant continuity adjustment of 0.5 events per group, the accrued information size (993) was 41.1% of the estimated RIS (RRR 67% = 2416; Fig. 3). For the use of aminoglycosides, the TSA estimation using a RRR of 26% and a CER proportion of 10%, with a constant continuity adjustment of 0.5 events per group, the accrued information size (5,218) was 31.1% of the estimated RIS (RRR 26% = 16,772; Fig. 3).
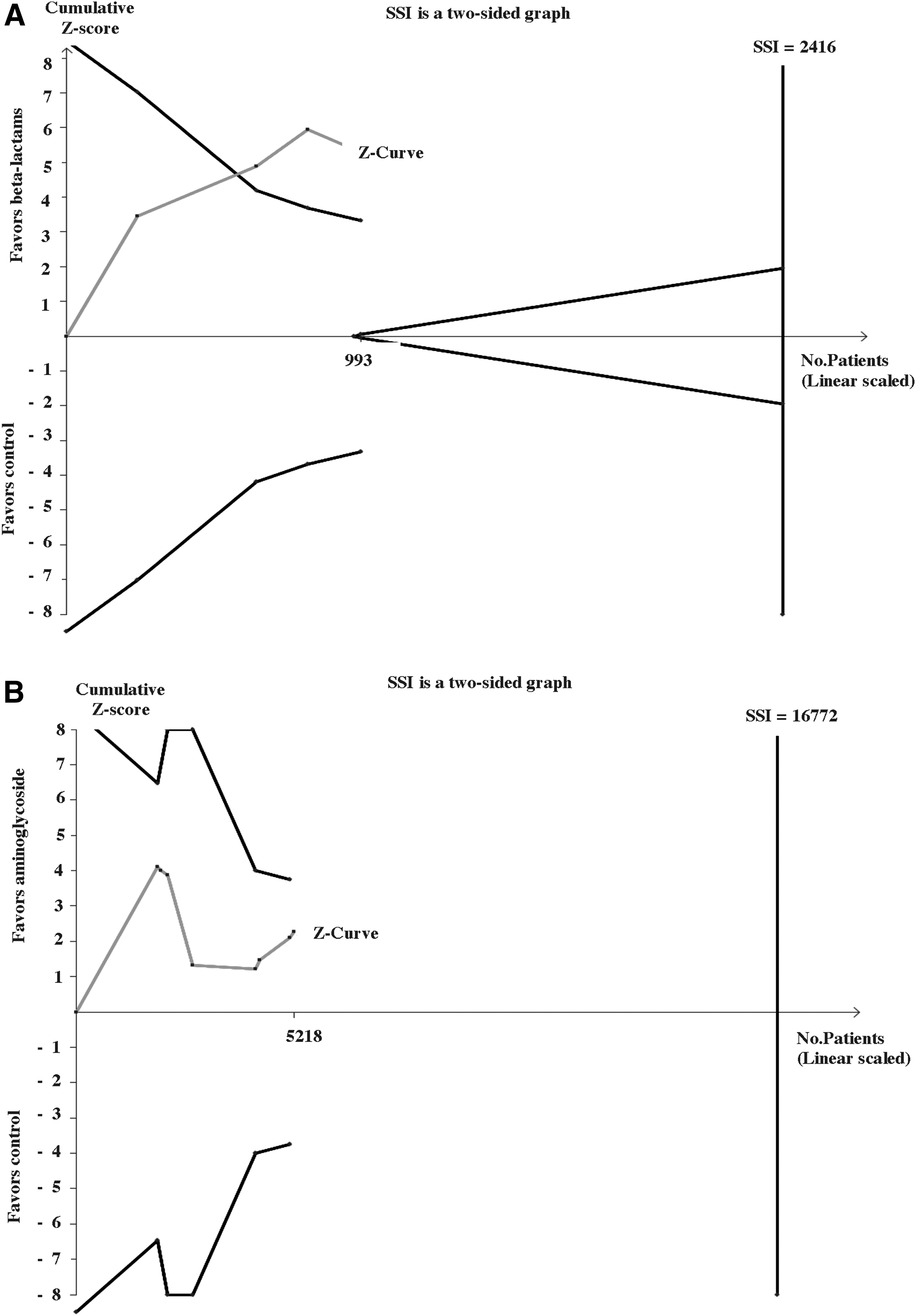
(
Discussion
This meta-analysis of RCTs shows that topical use of antibiotic agents before primary incision closure appears to reduce the risk of SSI compared with placebo (no use of antibiotic agents). The effectiveness of this measure remained after excluding RCTs of uncertain quality and those assessing SSI less than 30 days after the surgical procedure. In relation to the type of antibiotic agent, β-lactams (generally ampicillin) were effective, whereas aminoglycosides (generally gentamicin) were not. However, it was not possible to draw conclusions regarding the effectiveness of prophylactic use of topical antibiotic agents to prevent SSI in elective or urgent operations, type of surgical field, mode of application of the antibiotic agent, and presence or absence of associated systemic antibiotic treatment. Nevertheless, the present findings raise the question of whether this meta-analysis is sufficiently robust to support a definitive recommendation that topical antibiotic agents before primary incision closure effectively reduce the risk of SSI.
The RCTs selected for the study were published in the past five decades and included only two antimicrobial classes: β-lactams and aminoglycosides. Interestingly, articles assessing the effect of β-lactams were published up to the 1990s, in contrast to studies assessing the effect of aminoglycosides, which began to be reported in the literature in the 1990s up to the present time. With these remarks, the applicability of β-lactams to prevent SSI in current surgical practice may be seriously impaired for different reasons. First, as mentioned in other meta-analysis [50], studies of topical β-lactams did not progress in time because of increasing resistance of both gram-positive and gram-negative pathogens to ampicillin [51–53]. Second, the introduction of systemic antibiotic prophylaxis in the 1990s [54], and third, the overall deficient quality of RCTs as shown by inadequate or unreported methods of randomization, allocation concealment, and blinding are also limitations. Also, the most commonly accepted definition of SSI was proposed in 1999 [2], which determines a high heterogeneity in the definition of SSI used in previous studies as well as in the duration of follow-up, which was already pointed out in a systematic review performed immediately after 1999 [55]. Finally, other factors that are currently known to be associated with SSI such as obesity, smoking, or diabetes mellitus [2] were not adequately evaluated.
Regarding aminoglycosides, the increased use of these agents in the past decades may be because broad spectrum of activity and the post-antibiotic effect [56]. However, in our opinion it is not possible to recommend the generalized use of topical aminoglycosides in the current surgical practice. Not only the methodological quality of most RCTs included in the meta-analysis is uncertain, but also the risk of SSI was not substantially reduced when only high-quality studies [38,40,44–49] with 5,218 patients were analyzed. In addition, SSI rates reported in controls were higher than what is considered to be acceptable [14] both for studies of β-lactams [19,21,25,28] and aminoglycosides [38,40,44–49]; this fact may limit the applicability of results. Moreover, after estimate of TSA, the evidence accumulated in the literature is far below the potentially necessary information size, which indicates that more data are needed for the two classes of antibiotic agents to draw conclusions or to make solid recommendations regardless of statistical significance.
Limitations of the study include analysis restricted to prophylactic use of two antibiotic agents. Other strategies such as combination of antibiotic agents with different ointments (e.g., neomycin/polymyxin B/bacitracin zinc) were not examined, nor was a comparison between antibiotic agents and antiseptics made. Also, the information available was insufficient to assess whether systemic antibiotic prophylaxis or the use of associated systemic antibiotic agents could influence outcomes.
Conclusions
Currently, in light of our meta-analysis and in the age in which antibiotic resistance poses challenges in daily care [57], the use of topical antibiotic agents (β-lactams or aminoglycosides) before incision closure to reduce SSI cannot be recommended. However, without wishing to be controversial or create confusion, the use of topical antibiotic agents before incision closure cannot be excluded definitely from the prophylactic armamentarium because more data in quantity and quality are needed for the two classes of antibiotic agents (and perhaps others) to draw firm conclusions from robust evidence. It is likely that any future consideration regarding the use of topical antibiotic agents before incision closure for preventing SSI would require an evaluation of the micro-organisms involved most frequently in each particular surgical context, hospital environment, and antibiotic agent susceptibility patterns. Also, in the current context in which the evidence accumulated in the literature is far below the potentially necessary information size and in the age in which antibiotic resistance poses challenges [57], it may be useful to examine further the effect of high local antibiotic concentrations achieved with the use of topical antibiotic agents in multi-resistant environments with increased risk for SSI. In summary, we do not recommend the use of topical antibiotic agents before incision closure to reduce SSI but do recommend a large clinical trial on their efficacy.
Footnotes
Acknowledgments
The authors thank Dr. Marta Pulido for editorial assistance.
Author Disclosure Statement
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author(s) received no financial support for the research, authorship, and/or publication of this article.