
Abstract
Abstract
Background:
Post-operative central nervous system infection (PCNSI) caused by multi-drug–resistant/extensively drug-resistant (MDR/XDR) Acinetobacter baumannii is a severe complication. This study aimed to analyze the clinical presentation and treatment of this disorder.
Patients and Methods:
A retrospective study that recruited patients having PCNSI caused by MDR/XDR Acinetobacter baumannii was performed at our institute. The patients' demographic information and clinical data were recorded and analyzed. To analyze treatment, we assigned patients to different groups according to whether they had intraventricular/intrathecal injection of antibiotic agents or cerebrospinal fluid (CSF) drainage therapy.
Results:
Twenty-four patients were included. The risk factors were classified into two categories: environmental factors (intensive care unit stay, tracheal intubation or tracheotomy, positive culture of MDR/XDR Acinetobacter baumannii from other samples) or infectious approaches (CSF drainage, incision CSF leakage). Cerebrospinal fluid sterilization was achieved in 13 patients (54.2%) and the 30-day mortality was 50%. In the seven patients having intraventricular/intrathecal injection of antibiotic agents, the CSF sterilization rate was 71.4% (5/7) and 30-day mortality was 28.6% (2/7), compared with 47.1% (8/17; p = 0.27) and 58.8% (10/17; p = 0.18) in patients having only intravenous antibiotic agents. In 19 patients having CSF drainage therapy for PCNSI, the CSF sterilization rate was 63.2% (12/19) and 30-day mortality was 42.1% (8/19) compared with 20% (1/5; p = 0.08) and 80% (4/5; p = 0.13) in the remaining patients.
Conclusions:
The risk factors for PCNSI caused by Acinetobacter baumannii can be classified in two categories: environmental factors or infectious approaches. Both intraventricular/intrathecal injection of antibiotic agents and CSF drainage are helpful for CSF sterilization.
Post-operative central nervous system infection (PCNSI) is a severe complication secondary to cranial surgery that results in longer hospital stays, higher medical costs, and even serious neurologic dysfunction or death. The incidence of PCNSI ranges widely from 0.7%–8.9%, because of variations in diagnostic criteria [1–3]. The most common micro-organism responsible for PCNSI was gram-positive bacterium, including coagulase-negative staphylococcus and Staphylococcus aureus [3–5]. However, the rate of PCNSI caused by multi-drug–resistant/extensively drug-resistant (MDR/XDR) gram-negative bacillus is increasing rapidly [6,7]. Central nervous system (CNS) infections caused by MDR/XDR gram-negative bacillus are often difficult to treat and usually have poor outcomes with high mortality [6–10].
Acinetobacter baumannii is one of the most common MDR/XDR gram-negative bacillus with severe drug resistance that exists diffusely in the intensive care unit (ICU) and neurosurgical wards [11,12]. Although the incidence of PCNSI caused by Acinetobacter baumannii appears to be low (most of the articles are case reports), the patients' prognoses are poor [7,10]. For better analysis of this disorder, we reviewed 24 patients with PCNSI caused by MDR/XDR Acinetobacter baumannii and analyzed the clinical presentations and treatment of these cases.
Patients and Methods
Patients
This retrospective study was performed at the First Affiliated Hospital, College of Medicine, Zhejiang University. The patients' inclusion criteria were (1) adult patients (age ≥16 years old) reported to have PCNSI caused by MDR/PDR Acinetobacter baumannii from January 2015 to December 2016 and (2) PCNSI that had been treated at least for one week. The patients who had intracranial infection before the operation or who died within one-week post-operation were excluded. The study protocol was approved by the Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University based on the ethical standards of the 1964 Declaration of Helsinki and its later amendments, or on comparable ethical standards.
In the present study, PCNSI was defined as meningitis/ventriculitis and intracranial abscess/empyema according to the U.S. Centers for Disease Control and Prevention (CDC) criteria [4]. Moreover, MDR Acinetobacter baumannii was defined as the micro-organism resistant to at least one agent in three or more antimicrobial categories (such as carbapenems, aminoglycosides, and cephalosporins) [13]; XDR was defined as resistance to all other antimicrobial agents, except one or two antimicrobial agents [13].
Data collection and analysis
Demographic information and clinical data of the patients were recorded for every case. The demographic data included gender and age and the clinical data included primary disease, the operation and peri-operative time incidents that may be related to PCNSI, cerebrospinal fluid (CSF) examination results, the susceptibility of MDR/XDR Acinetobacter baumannii to different antibiotics, the treatment aimed at intracranial infection (surgical management and the use of antibiotic agents), as well as the treatment efficacy and the patient outcomes.
Intraventricular/intrathecal injection of antibiotics is an important method for treating intracranial infection caused by MDR/XDR Acinetobacter baumannii [7,14]. In the present study we compared the CSF sterilization rate and 30-day mortality between patients receiving intravenous antibiotic agents combined with intraventricular/intrathecal injection of antibiotic agents and those only receiving intravenous antibiotics. Furthermore, we compared the same indicators between patients having CSF drainage therapy for PCNSI and those only having antibiotic agent therapy.
All data were analyzed with SPSS software (version 18.0; SPSS Inc., Chicago, IL); 95% confidence intervals (CI) were calculated and p values <0.05 were considered statistically significant. Differences were compared using Pearson χ2 or Fisher exact test for ranked variables.
Results
Study population and clinical presentation
A total of 24 patients were included in the present study. Twelve patients underwent cranial operation for cerebrovascular disease (including hypertensive intracerebral hemorrhage, intracranial aneurysm, and cerebral artery-venous malformation), nine patients underwent craniotomy/craniectomy for head trauma, and three patients underwent craniotomy for intracranial tumor.
Clinical factors can increase the risk of PCNSI caused by MDR/XDR Acinetobacter baumannii, including CSF drainage therapy, incision CSF leakage, the history of tracheal intubation or tracheotomy, ICU stay, carbapenems use, and positive culture of MDR/XDR Acinetobacter baumannii from other humoral samples [10]. We analyzed these risk factors and the results are shown in Table 1. Before the onset of PCNSI, most of these patients had a history (more than three days) of tracheal intubation or tracheotomy (87.5%), ICU stay (more than three days, 87.5%), and CSF drainage (62.5%) including extraventricular drainage (EVD) or lumbar cistern drainage (LCD).
Risk factors for Post-Operative Central Nervous System Infection Caused by Multi-Drug–Resistant/Extensively Drug-Resistant Acinetobacter baumannii
CSF = cerebrospinal fluid; ICU = intensive care unit, MDX/XDR = multi-drug resistant/extensively drug-resistant.
PCNSI, CSF examination results, and susceptibility testing
Twenty of 24 patients had simple ventriculitis/meningitis, two had ventriculitis/meningitis combined with incision infection, one developed ventriculitis/meningitis and incision infection combined with intracerebral abscess, and the other developed ventriculitis/meningitis combined with subdural abscess. The time from first operation to the onset of PCNSI was three to seven days for six patients, eight to 21 days for 16 patients, and more than 28 days for two patients.
The average number of leukocytes in CSF was 41,373 ± 108,405 per microliter (median: 8,500 per microliter); the average protein level was 6.1 ± 4.8 g/L (median: 5.4 g/L); and the average glucose level was 0.7 ± 1.5 mmol/L (median: 0.1 mmol/L).
Information regarding the susceptibility of MDR/XDR Acinetobacter baumannii to different antibiotic agents in the present study is shown in Table 2; this micro-organism was resistant to most common antibiotic agents including carbapenems and cephalosporin. Only colistin and tigecycline had a high sensitivity rate above 70%.
Results of the Susceptibility of Twenty-Four Strains of Multi-Drug–Resistant/Extensively Drug-Resistant Acinetobacter baumannii to Different Antibiotic Agents
Treatment and outcomes
Surgical management
After the diagnosis of PCNSI caused by Acinetobacter baumannii, CSF drainage therapy including EVD and LCD were performed in 19 patients; the average time of CSF drainage therapy was 11.1 ± 4.9 days (range, 5–21 days). Five patients had debridement for combined incision infection or removal of artificial materials (such as artificial meninge).
Antibiotic therapy
All 24 patients received intravenous antibiotic agent therapy. Additionally, seven patients received intraventricular/intrathecal injection of antibiotic agents based on intravenous therapy. These patients were assigned to the intraventricular/intrathecal group; those who did not receive such therapy but only received intravenous antibiotic agents were assigned to the intravenous group. Information regarding antibiotic agent therapy is shown in Table 3.
Antibiotic Agent Therapy
T = therapy method.
Cerebrospinal fluid sterilization was achieved in 13 patients (54.2%). The CSF sterilization rate was 71.4% (5/7) in the intraventricular/intrathecal group and was 47.1% in the intravenous group (8/17; χ2 test, p = 0.27). The 30-day mortality post-onset of PCNSI caused by MDR/XDR Acinetobacter baumannii was 50% (12 patients died) in the present study. In the intraventricular/intrathecal group, the 30-day mortality was 28.6% (2/7); in the intravenous group, the 30-day mortality was 58.8% (10/17; χ2, p = 0.18).
We compared the CSF sterilization and 30-day mortality between patients who had CSF drainage therapy combined with antibiotic agent therapy (CSF drainage group, 19 patients) and those only having antibiotic agent therapy (antibiotics group, five patients). In the CSF drainage group, the CSF sterilization rate was 63.2% (12/19) and the 30-day mortality post-onset of PCNSI was 42.1% (8/19). In the antibiotic agent group, the CSF sterilization rate was 20% (1/5; χ2, p = 0.08), and the 30-day mortality post-onset of PCNSI was 80% (4/5; χ2, p = 0.13).
Discussion
Acinetobacter baumannii is an opportunistic micro-organism that exists widely in healthcare institutes. At present it is one of the most common pathogenic bacteria for nosocomial infection, especially for ICU and surgical wards [15–17]. Acinetobacter baumannii is also a pathogenic bacterium with severe bacterial resistance to antibiotic agents in China [18].
Although PCNSI caused by MDR/XDR Acinetobacter baumannii seemed to be rare before, the incidence has increased quickly. Pan et al. [7] reported a rate of 33.64% of intracranial infections caused by MDR/XDR Acinetobacter baumannii of all patients developing PCNSI. In our institute, the rate of PCNSI caused by MDR/XDR Acinetobacter baumannii is increasing as well, although the gram-positive coccus is still the main pathogenic bacteria.
Some clinical factors can increase the risk of PCNSI caused by Acinetobacter baumannii. These factors can be classified in two categories: environmental factors and infectious approaches (Fig. 1). The ICU usually has the highest infectious rate of MDR/XDR micro-organism and is the main source of nosocomial infections caused by MDR/XDR Acinetobacter baumannii [15,19]. In the present study, most patients had a history of ICU stay (87.5%). In addition, 62.5% of the patients had positive culture of MDR/XDR Acinetobacter baumannii from other humoral samples (blood, sputum, or both). These two factors that indicated the presence of MDR/XDR Acinetobacter baumannii in the environment made the PCNSI caused by this micro-organism possible.
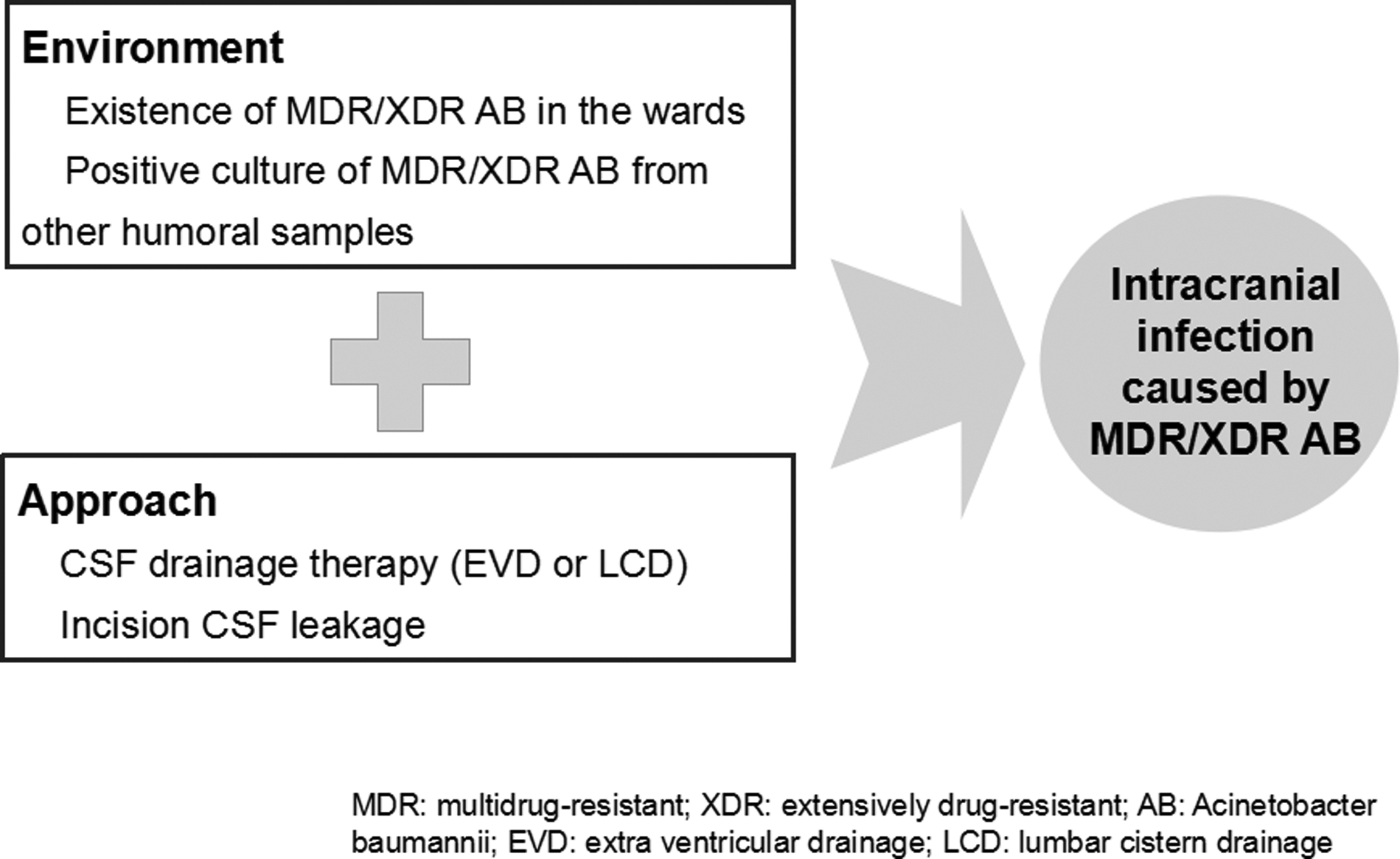
Risk factors of post-operative central nervous system infection (PCNSI) caused by multi-drug–resistant/extensively drug-resistant (MDR/XDR) Acinetobacter baumanni.
In addition to existence in the environment, there are sources that allow the micro-organism to spread into the cranium. Cerebrospinal fluid drainage (mainly including EVD and LCD) is a risk factor for PCNSI [20], especially for that caused by Acinetobacter baumannii. The drainage tube is a potential source for the bacterium getting into the cranium. In the present study 62.5% of patients had CSF drainage therapy before the onset of PCNSI. In addition, six patients (25%) developed incision CSF leakage. Both of these factors allowed the micro-organism to get into the cranium and increased the risk of PCNSI. When such patients are in an environment in which MDR/XDR Acinetobacter baumannii exists around them, the risk of PCNSI caused by this micro-organism increases substantially.
Post-operative central nervous system infection caused by MDR/XDR Acinetobacter baumannii usually leads to severe meningitis/ventriculitis with dramatically decreased glucose levels in CSF (the median level of CSF glucose was only 0.1 mmol/L in the present study). An important feature of meningitis/ventriculitis caused by MDR/XDR Acinetobacter baumannii is the CSF protein concentration. The protein level usually increased substantially. In the present study, the average CSF protein level was 6.1 ± 4.8 g/L (median: 5.4 g/L). Such high CSF protein level would lead to adhesion of subarachnoid space and ventricular system, which increases the risk of hydrocephalus.
The outcomes of intracranial infections caused by MDR/XDR Acinetobacter baumannii are poor according to previous studies; the mortality ranged from 20% to 48% [10,21–23]. One of the reasons is the severe bacterial resistance to common antibiotic agents. In the present study, only colistin and tigecycline had a relatively high sensitivity rate above 70%. Unfortunately, usually the drug CSF levels of both colistin and tigecycline are too low to eradicate the micro-organism. Thus, for PCNSI caused by MDR/XDR micro-organism, intraventricular/intrathecal injection of antibiotic agents is an important method for saving patients' lives. In the present study, seven patients had intraventricular/intrathecal antibiotic agents and both the CSF sterilization rate (71.4%–47.1%) and 30-day mortality (58.8%–28.6%) are higher than those in patients only having intravenous antibiotic agents. Although there were no statistical differences, probably because of the small sample, the intraventricular/intrathecal injection of antibiotic agents should be utilized for treating such patients. The same results have been reported by previous studies [7,9,10,14] and the intraventricular/intrathecal injection of antibiotics was suggested to be the last resort for treating intracranial infection caused by MDR/XDR Acinetobacter baumannii [14]. However, we suggest that it may be performed early after diagnosis of PCNSI caused by MDR/XDR Acinetobacter baumannii.
In the present study, two patients had intraventricular/intrathecal injection of antibiotic agents but still did not recover from PCNSI. For these patients, the intracranial infection developed rapidly even though intravenous antibiotic agents had been used. The intraventricular/intrathecal injection of antibiotic agents was performed one-week post-diagnosis. Prior to that, the number of leukocytes in CSF was above 50,000 per microliter, CSF protein level was above 15 g/L, and CSF glucose level was below 0.1 mmol/L. Finally, the PCNSIs could not be cured. When the intracranial infection develops rapidly and the CSF becomes ropy, the adhesion of subarachnoid space and ventricular system would prevent the antibiotic agents from spreading in the CSF circulation even though intraventricular/intrathecal injection had been performed. As a result, the intracranial infection cannot be controlled. Additionally, we believe that the CSF drainage therapy is another important method for treating intracranial infection caused by MDR/XDR Acinetobacter baumannii. Cerebrospinal fluid drainage therapy is able to help clear the infectious CSF and accelerate the process of CSF sterilization, especially for severe intracranial infection. As for PCNSI caused by MDR/XDR Acinetobacter baumannii, because of the high CSF protein level and high risk of hydrocephalus, CSF drainage therapy seems to be more effective. Furthermore, EVD or LCD make the intraventricular/intrathecal antibiotic agents easier and more convenient.
In the present study, the CSF sterilization was relatively low compared with previous studies. One of the reasons is the low rate of intraventricular/intrathecal injection of antibiotics. Colistin and tigecycline are two antibiotics that have good sensitivity to MDR/XDR Acinetobacter baumannii. There are several case reports regarding the use of tigecycline for intraventricular/intrathecal antibiotic agent therapy [9,24], but the safety and efficacy need further study. Polymycin is the only antibiotic that has good sensitivity for MDR/XDR Acinetobacter baumannii and can be used for intraventricular/intrathecal injection, however in China it was not easily accessible and was expensive prior to 2018 and is why our patients had low rates of intraventricular/intrathecal injection of antibiotic agents. In addition, in this study, for some patients the treatment period was shortened because of death, other reasons, or cessation of treatment by relatives.
Conclusion
In present study, we retrospectively analyzed 24 patients who developed PCNSI caused by MDR/XDR Acinetobacter baumannii. The types of clinical factors that would increase the risk of this disorder include CSF drainage therapy (62.5%), incision CSF leakage (25%), tracheal intubation or tracheotomy (87.5%), ICU stay (87.5%), history of carbapenems use (54.2%), and positive culture of MDR/XDR Acinetobacter baumannii from other humoral samples (62.5%). Regarding treatment, both intraventricular/intrathecal injection of antibiotic agents and CSF drainage therapy are helpful for CSF sterilization.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest.