
Abstract
Abstract
Background:
Despite surgical treatment of peptic ulcer perforation (PUP), the high rates of morbidity and mortality have motivated researchers to search for new laboratory markers to predict morbidity and mortality. The aim of this study was to investigate the relation between pre-operative laboratory values and demographic factors and post-operative mortality in patients undergoing surgery for PUP.
Patients and Methods:
A retrospective study was made of the clinical findings and laboratory data of patients operated on for a diagnosis of PUP in the general surgery clinic between 2014 and 2018. The patients were separated into two groups according to survival (PUP-S) or mortality (PUP-M) and the differences between the groups were evaluated.
Result:
In the analysis of the patient data, age (p = 0.014), female gender (p = 0.005), length of stay in hospital (p = 0.009), platelet to lymphocyte ratio (PLR) (p = 0.09), and neutrophil to lymphocyte ratio (NLR) (p = 0.010) values were determined to be high and lymphocyte count was low (p = 0.046) in the PUP-M group. A positive correlation was determined between mortality and age, length of stay in hospital, PLR, and NLR (p < 0.05). A substantial negative correlation was determined between mortality and gender and lymphocyte count (p < 0.05). As a result of the receiver operating characteristic (ROC) curve analysis, it was determined that a PLR value <322.22 (p = 0.009) and lymphocyte count <0.67 × 103 microliter (p = 0.035) could have diagnostic value in the prediction of the possibility of mortality in patients operated on because of PUP.
Conclusion:
This study results suggested that PLR, NLR, and lymphocyte count values could be used as new biomarkers to identify the mortality risk in patients operated on for peptic ulcer perforation.
Peptic ulcer perforation (PUP) is a high-risk acute abdomen event that constitutes 5% of all abdominal emergency situations. It is a severe complication that can result in localized or generalized peritonitis, sepsis, and even death [1–3]. The mortality rate in patients developing PUP has been reported as 10%–40% [4,5]. It is not believed that there is a single factor that can identify patients at high risk of mortality easily, and it has been reported that advanced age, presence of comorbidities, and a delay in surgery can increase the mortality risk associated with PUP [3]. Therefore, surgery is still advocated as the optimal treatment for PUP [1,6]. Nevertheless, despite the surgical treatment of PUP, continuing high rates of morbidity and mortality have motivated researchers to search for new laboratory markers to predict morbidity and mortality.
Several biomarkers have been used as markers of inflammation, primarily C-reactive protein (CRP), procalcitonin, mean platelet volume (MPV), platelet to lymphocyte ratio (PLR), and neutrophil to lymphocyte ratio (NLR), to predict prognosis in inflammatory diseases [1,7]. Neutrophil to lymphocyte ratio and PLR have been recommended as new markers of systemic inflammation in clinical practice and they are being used increasingly in the prediction of prognosis of patients with malignancy, coronary artery disease, acute appendicitis, acute cholecystitis, acute pancreatitis, and community-origin infections [8–14]. However, to the best of our knowledge, there has been no study that has evaluated the use of NLR and PLR values to determine post-operative patient prognosis and the risk of mortality in patients treated with surgery for PUP. The aim of this study was to investigate the relation between pre-operative laboratory values and demographic factors and post-operative mortality in patients operated on because of PUP.
Patients and Methods
Patient groups
Approval for this retrospective study was granted by the Clinical Research Local Ethics Committee (decision no: 14/05, dated: 12/06/2018). The clinical and laboratory data of patients who were operated on in the general surgery clinic with a diagnosis of PUP between 2014 and 2018 were examined. Patients were excluded if all the information was not available from the records, if they were aged <18 years, or if the perforation was related to traumatic or iatrogenic injury or stomach tumors.
The patients were separated into two groups: (1) PUP-S (patients who survived after surgical treatment, n = 19) and (2) PUP-M (patients who died after surgical treatment, n = 4).
Methods
Age, gender, and length of stay in the hospital were recorded. Furthermore, the measurements of the blood hemoglobin level, leukocyte, neutrophil, lymphocyte and platelet counts values, and MPV, NLR, and PLR values, which were obtained from the patients' medical data related to their first admissions to the hospital, were also recorded.
Surgery
The perforation area was repaired with the open suture repair technique. After peritoneal toilet procedure, both sides of the perforation area were sutured at full-layer thickness with single silk sutures and the omentum placed below the sutures [15].
Biochemical analysis
The routine biochemical parameters were examined in the venous blood samples taken when the patients were admitted to the hospital. In the biochemistry laboratory, hemoglobin (reference interval 10–18 g/dL), thrombocyte (reference interval 150,000–450,000 per microliter), MPV (reference interval 0.00–15.00 fL) leukocyte (reference interval 4,400–11,300 per microliter), neutrophil (reference interval 1,100–9,600 per microliter), and lymphocyte (reference interval 500–6,000 per microliter) counts were determined using an analyzer device (Mindray BC-6800, Shenzen, China).
Statistical analysis
Demographic and laboratory data were reported as mean, median, standard deviation, minimum, maximum, number, and percentage values. The differences between groups of non-parametric data were evaluated using the Mann-Whitney U test (p < 0.05). Parametric data were analyzed using the independent samples t-test (p < 0.05). Spearman ρ correlation and Pearson correlation analyses were applied to determine correlations between the parameters of the patients (p < 0.05). In the evaluation of the sensitivity and specificity of the parameters in diagnosis and to predict prognosis, the ROC curve test was used (p < 0.05).
Results
A total of 23 patients were included in the study. There were 18 male males (78.3%) and five females (21.7%) with a mean age of 54.52 ± 20.38 years. Perforation localization was determined during surgery as in the stomach in 19 (82.6%) patients and in the duodenum in four (17.4%). Primary repair and omentoplasty was applied to all the patients. Length of stay in hospital was mean 11.17 ± 6.18 days. Four patients (17.4%) died and 19 (82.6%) were discharged with medication (Table 1).
Demographic Data and Laboratory Results of All Patients
SD = standard deviation; n = number of patients.
Age, gender, length of stay in hospital, pre-operative lymphocyte count, and pre-operative PLR and NLR values were not statistically different between the groups (Table 2). The mean age was substantially higher in the PUP-M group (76.50 ± 10.27 years) compared with the PUP-S group (49.89 ± 18.97 years; p = 0.014). The rate of female gender was higher in the PUP-M group at 75% compared with 10.5% in the PUP-S group (p = 0.005). The length of stay in hospital was statistically significantly longer in the PUP-M group at 18.50 ± 4.04 days compared with 8.00 ± 5.76 days in the PUP-S group (p = 0.009). The pre-operative lymphocyte count value was measured as 0.59 ± 0.40 in the PUP-M group and as 1.63 ± 0.94 in the PUP-S group, and the difference was statistically significant (p = 0.046). The pre-operative PLR was higher in the PUP-M group at 460.21 ± 418.45 compared with 173.73 ± 272.80 in the PUP-S group (p = 0.09). The pre-operative NLR was higher in the PUP-M group at 21.25 ± 15.96 compared with 9.98 ± 5.73 in the PUP-S group (p = 0.010). No statistically significant difference was determined between the groups in terms of perforation localization, hemoglobin, leukocyte, neutrophil, platelet, and MPV values (Table 2, Figs. 1 and 2).
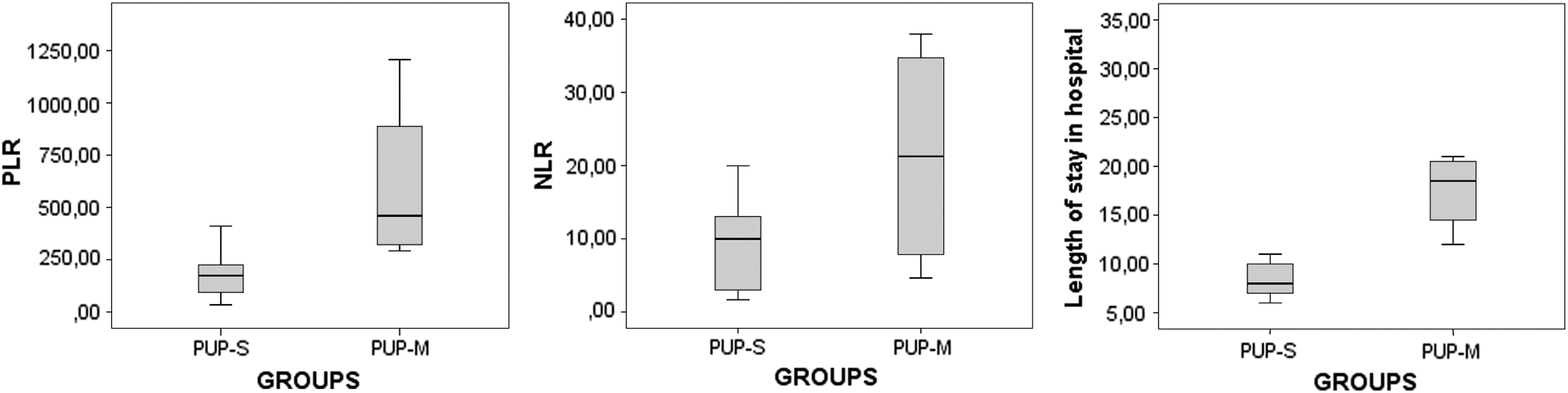
Graphs showing the platelet to lymphocyte ratio (PLR), neutrophil to lymphocyte ratio (NLR), and length of stay in hospital of the groups.
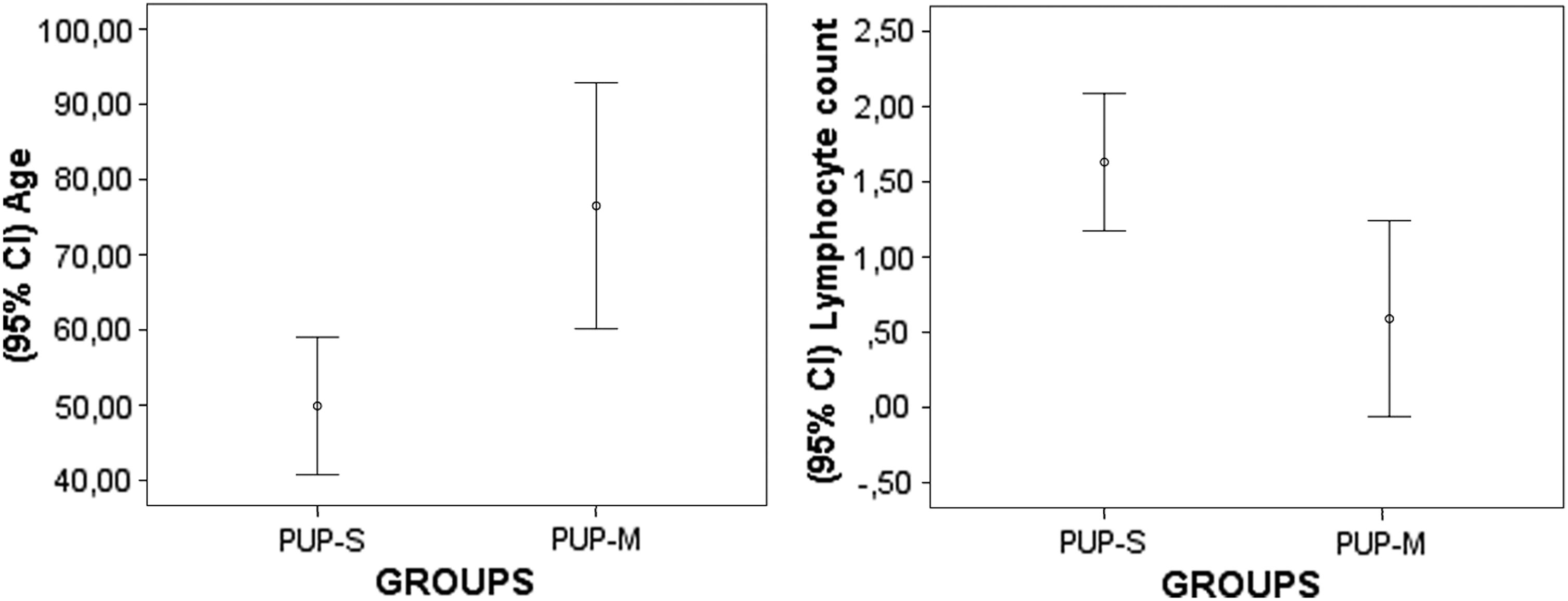
Graphs showing the age and lymphocyte count values of the groups.
Results of the Statistical Comparisons of the Variables of the Groups
Mann-Whitney U test.
Mann-Whitney U test, independent samples t- test, p < 0.05.
In the correlation analysis, a positive correlation was determined between mortality and age (pr = 0.506, p = 0.014), between mortality and length of stay in hospital (sr = 0.560, p = 0.005), between mortality and PLR (sr = 0.553, p = 0.006), between mortality and NLR (pr = 0.523, p = 0.010), between PLR and length of hospital stay (sr = 0.540, p = 0.008) and between age and length of stay in hospital (pr = 0.437, p = 0.037) (Figs. 3 and 4).
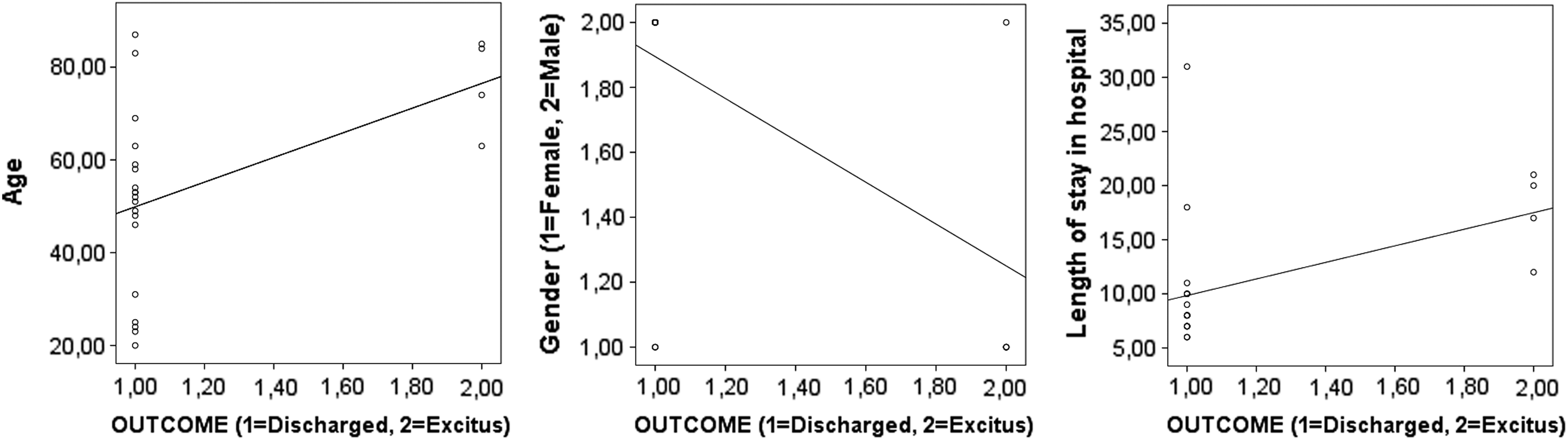
Correlation graphs of the variables of age, gender, and length of stay in hospital.
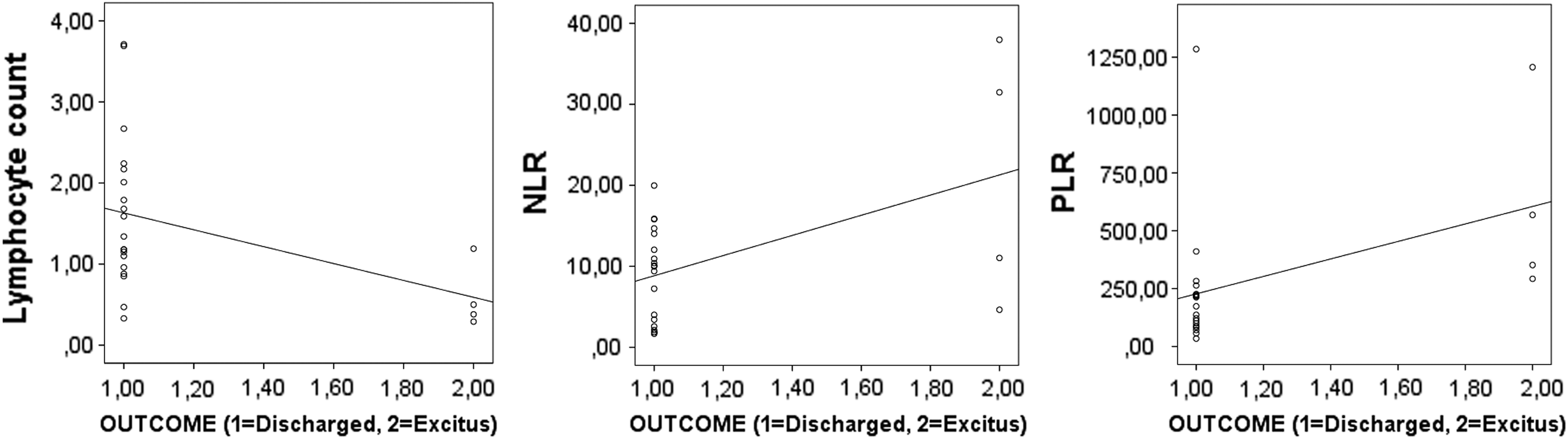
Correlation graphs of the variables of lymphocyte count, neutrophil to lymphocyte ratio, and platelet to lymphocyte ratio values.
A negative correlation was determined between mortality and gender (female = 1, male = 2) (sr = −0.592, p = 0.003). It was believed with these findings that mortality rate increased in female gender. Furthermore, a negative correlation was found between mortality and lymphocyte count (pr = −0.421, p = 0.046), between age and lymphocyte count (pr = −0.443, p = 0.034), between length of hospital stay and gender (female = 1, male = 2) (sr = −0.547, p = 0.007), and between length of stay in hospital and lymphocyte count (pr = −0.439, p = 0.036) (Figs. 3 and 4).
The ROC curve analysis applied to determine the sensitivity and specificity of PLR, NLR, and lymphocyte count values demonstrated that a PLR value >322.22 had diagnostic value with approximately 75% sensitivity and 98.50% specificity in the differentiation and prediction of the mortality probability in patients operated on because of PUP (area = 0.921, p = 0.009, cutoff = 322.22). In addition, a lymphocyte count value of <0.67 × 103 per microliter was believed to have diagnostic value with approximately 89.50% sensitivity and 75% specificity in the prediction of the possibility of mortality in patients operated on because of PUP (area = 0.842, p = 0.035, cutoff = 0.67) (Table 3, Fig. 5).
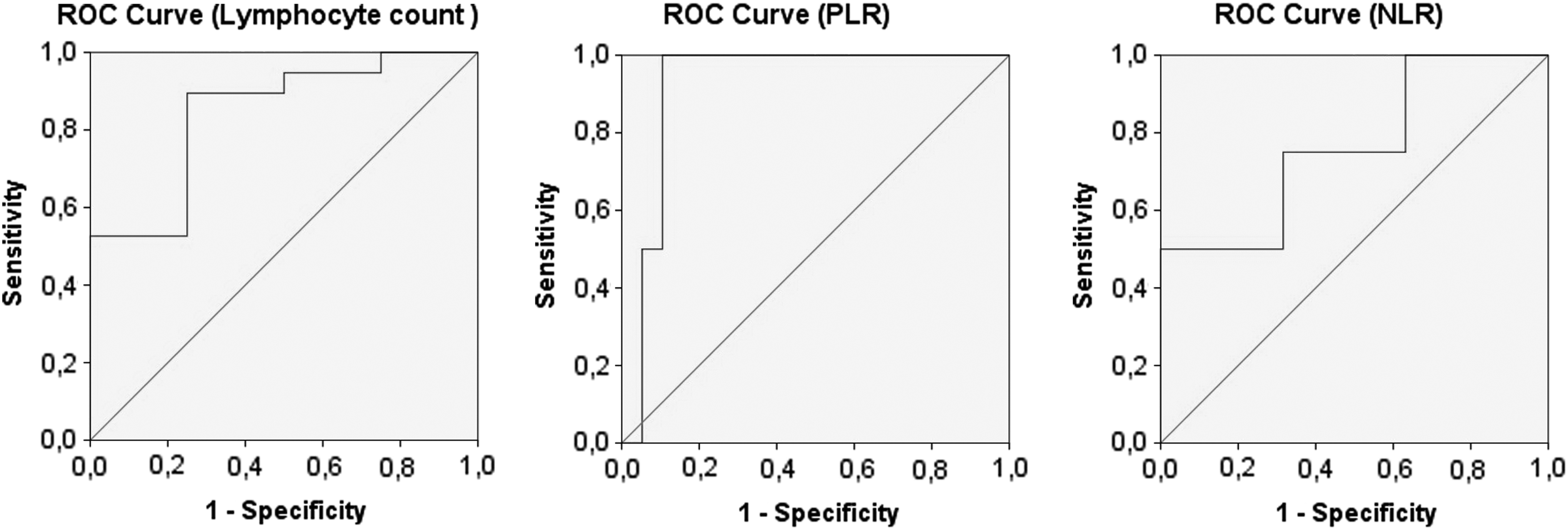
Receiver operating charachteristic (ROC) curve graphs showing the sensitivity and specificity of the lymphocyte count, neutrophil to lymphocyte ratio, and platelet to lymphocyte ratio values in the determination of the mortality risk of the patients.
Sensitivity and Specificity Percentage Values of Lymphocyte Count, Platelet to Lymphocyte Ratio, and Neutrophil to Lymphocyte Ratio of the Groups in the Determination of the Risk of Mortality
Receiver operating characteristic curve test, p < 0.05.
PLR = platelet to lymphocyte ratio; NLR = neutrophil to lymphocyte ratio.
Discussion
Peptic ulcer perforation is a high-risk acute abdomen condition that can cause the development of generalized or localized peritonitis, sepsis, and death [3]. Morbidity rates have been reported as 50% and mortality as 4%–30% [3,16,17]. Testini et al. [18] reported that the post-operative mortality risk was higher in patients with PUP aged >65 years compared with younger patients. Koçer et al. [19] showed a mortality rate of 1.4% in patients aged <65 years and 37.3% in those aged over 65 years. Sivaram et al. [16] reported a relation between female gender and mortality. Kim et al. [20] also reported that female gender was a factor related to morbidity. The length of stay in hospital of PUP patients was reported by Arveen et al. [21] to be mean 10.9 ± 6.8 days, whereas Sivaram et al. [16] reported a mean stay of 11.6 ± 7.3 days with a maximum of 46 days, and observed a correlation with morbidity when hospital stay exceeded two weeks. In the current study, the length of stay in hospital was mean 11.17 ± 6.18 days with a maximum stay 31 days. The mortality rate in the current study was 17.4%.
In the comparisons between the groups, age, female gender, length of stay in hospital, pre-operative PLR and NLR values were found to be higher and the pre-operative lymphocyte count was lower in the PUP-M group. In the correlation analysis, this mortality rate was determined to be correlated to advanced age, female gender, pre-operative low lymphocyte count, and high PLR and NLR values. Thus, the majority of the patients in the mortality group were female and of advanced age, the length of stay in hospital of this group was longer, and the lymphocyte count of these patients was at a substantially low level.
The low lymphocyte count was seen to be correlated with age and length of stay in hospital and there was also a relation between age and length of stay in hospital. From these findings, it can be considered that a low lymphocyte level and advanced age could prolong the length of stay in hospital and these three parameters could affect and increase patient mortality both directly and indirectly.
Corresponding to the advanced age in the PUP-M group, the fact that the lymphocyte count was determined to be low suggests that advanced age could reduce the lymphocyte count indirectly. It is believed that in this older aged patient group, there could be a delay in the cellular immune response related to the low lymphocyte count, and mortality rates could be further increased in this elderly patient group as a result of weakness related to this delay in inflammatory response that could then produce a perforation table. In addition, sensitivity and specificity studies have found that the lymphocyte count could have diagnostic value with approximately 89.50% sensitivity and 75% specificity in the differentiation and prediction of the probability of mortality in patients. Therefore, it has been proposed that the lymphocyte count measured pre-operatively could be used as a biomarker in the prediction of mortality rates.
Despite the similarity of the leukocyte, neutrophil, and thrombocyte counts in the two groups, the NLR and PLR values were different, and these values were determined to be substantially higher in the PUP-M group. The difference in the NLR and PLR values between the groups can be attributed to the difference in lymphocyte levels, and because of the low lymphocyte count measured in the PUP-M group, the NLR and PLR values were determined to be higher. In the correlation analysis, just as a correlation was determined between the low lymphocyte count and mortality rates, there was also a direct correlation between mortality and the NLR and PLR values. It is believed that when the PLR and NLR values increase, the mortality rates could increase. In addition, it was seen that the PLR value could have diagnostic value with approximately 75% sensitivity and 98.50% specificity in the differentiation and prediction of the probability of mortality in PUP. Thus, it has been advocated that PLR values together with NLR values could each be used as a biomarker for patient prognosis and mortality rates.
Study limitations
There were some limitations to this study, primarily that the study design was retrospective and therefore the number of patients included was low. However, the study had similar features to those found in the literature and with the emergence of interesting results can be considered a pioneering study. Therefore, there is a need for further, more extensive studies with larger patient groups to confirm these results. A second limitation is that molecular level studies (cytokines, chemokines) were not made of the patients' blood samples as it would have been distant from the aim of the study. Third, because patient comorbidities were not included in the scope of this study, relations between mortality rates and comorbidities were not examined. Finally, because the aim of the study was to identify predictive and prognostic parameters obtained from routine biochemical laboratory tests in patients operated on for a diagnosis of PUP, the radiologic images of the patients were not evaluated.
Conclusion
From the results of the study, it was observed that mortality rates in patients operated on for a diagnosis of PUP could be higher in females, older patients, and those with a prolonged stay in hospital. It was also determined that mortality rates could be high in patients with high NLR and PLR values and low lymphocyte count.
In conclusion, in addition to NLR, PLR, and lymphocyte count values, age, gender, and length of hospital stay can be considered as new biomarkers in the determination of mortality risk in patients undergoing surgery for PUP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.