
Abstract
Abstract
Background:
Although uncomplicated acute diverticulitis has a benign disease course, some patients are at increased risk for complications. Identification of these patients may aid the selection of treatment strategies such as outpatient treatment. This study aimed to assess the rate and timing of a complicated disease course in initially computed tomography (CT)-proven uncomplicated diverticulitis, and to identify risk factors for the development of these diverticular complications.
Patients and Methods:
Computed tomography-proven, left-sided uncomplicated diverticulitis patients from two cohorts were included. Main outcome measure was complicated diverticulitis (perforation, abscess, obstruction, or fistula) within three months after presentation. Risk factors for diverticular complications were identified using multivariable logistic regression.
Results:
Of the 1,087 patients with initially CT-proven uncomplicated diverticulitis, 4.9% (53/1,087) developed complicated diverticulitis. Most perforations and abscesses (16/21) occurred during the first 10 days, whereas colonic obstruction and fistula occurred during three months of follow-up. Independent risk factors for the transition from uncomplicated to complicated diverticulitis were American Society of Anesthesiologists (ASA) classification 3/4 (odds ratio [OR] 4.43, 95% confidence interval [CI] 1.57–12.48), duration of symptoms before presentation longer than five days (OR 3.25, 95% CI 1.72–6.13), vomiting (OR 3.94, 95% CI 1.96–7.92), and C-reactive protein (CRP) above 140 mg/L (OR 2.86, 95% CI 1.51–5.43).
Conclusion:
Approximately one in 20 patients with CT-proven uncomplicated diverticulitis develops a complicated disease course within three months; perforation and abscess occur predominantly within 10 days after presentation. Patients with systemic comorbidity, symptoms for more than five days, those who vomit, or have high CRP levels at presentation are at risk for diverticular complications after an uncomplicated initial presentation and may warrant closer observation.
Acute diverticulitis is a condition diagnosed commonly at the emergency department and often results in hospital admission. The presentation of patients with acute diverticulitis can vary from mild and self-limiting to severe with a need for emergency surgery. Based on current knowledge, most patients with uncomplicated diverticulitis, defined as pericolic inflammation only, are suitable for non-antibiotic and outpatient treatment [1–3]. However, some patients may be at higher risk for complications and therefore may warrant a different approach. Timely identification of these patients could prevent under-treatment and may prevent additional adverse events.
Currently, treatment strategies are based mostly on the stage of diverticulitis at presentation, assuming all patients at a certain stage should be treated equally. Therefore, most studies have focused on the severity of the disease at presentation. Determination of risk factors for the presence of diverticular complications at the emergency department have limited value because imaging is available and more accurate. Risk factors for the progression into complicated diverticulitis would be more useful. Studies addressing risk factors for a complicated course of initially uncomplicated acute diverticulitis are scarce, and because this complicated progression seems relatively rare in uncomplicated diverticulitis, the few studies on this topic lack statistical power to identify patients at risk adequately [4–7].
The aim of this study was to identify risk factors for a complicated course of disease in initially computed tomography (CT)-proven uncomplicated diverticulitis. Furthermore, this study aimed to assess which types of diverticular complications occur and in which time interval after presentation patients are at risk for a complicated disease course.
Patients and Methods
Study design and patient population
Patients with acute left-sided uncomplicated diverticulitis (Hinchey Ia [8] confirmed by abdominal CT were included. Data in this observational cohort study comprised two Dutch acute diverticulitis cohorts. The first was a retrospective cohort from three Dutch hospitals (Onze Lieve Vrouwe Gasthuis, Meander Hospital, and Sint Antonius Hospital), including 1,233 patients admitted to the hospital with a primary episode of acute diverticulitis between January 2004 and January 2012 [9]. The second was a cohort of 528 patients from the Dutch randomized DIABOLO trial [2]. This randomized control trial compared observational and antibiotic treatment for uncomplicated acute diverticulitis (Hinchey Ia and Ib) and included only primary episodes of CT-proven acute diverticulitis patients from 22 Dutch hospitals between June 2010 and October 2012. Both cohorts combined resulted in a total of 1,761 patients. After applying inclusion criteria and removing duplicates a total of 1,087 patients remained.
Outcomes and follow-up
Outcome measures were the number of patients with complicated diverticulitis at three months of follow-up and the type of complication. Clinical events within the first three months after the initial acute diverticulitis diagnosis were considered related to this initial episode and therefore informative about the disease course of that (initially) Hinchey Ia episode. Complicated diverticulitis was defined as diverticulitis with abscess formation, free perforation, colonic obstruction requiring surgical intervention, or fistula.
Statistical analysis
For categorical variables, numbers and percentages were calculated and continuous variables are expressed as mean and standard deviation or median and interquartile range (IQR), as appropriate. First, rates of diverticular complications were calculated and plotted against the time from presentation. Second, risk factors for the development of diverticular complications (perforation, abscess, obstruction, or fistula) were assessed using multivariable logistic regression analysis. Patient characteristics and clinical parameters that were univariably associated (p < 0.10) with the outcome measure were entered into the multivariable logistic regression model. Numerical variables were univariably tested as continuous variables for selection for the multivariable models but were dichotomized in the multivariable models to ease interpretation and usage in daily practice. Age (≤50 years or >50 years), body temperature (≤38.5°C or >38.5°C), and duration of symptoms before presentation (≤5 days or >5 days) were dichotomized using clinically relevant thresholds. Thresholds for duration of symptoms, C-reactive protein (CRP), and white blood cell (WBC) count were set at optimal sensitivity and specificity according to receiver operating characteristic (ROC) curves. Both CRP and WBC were measured on the day the patient presented to the emergency department.
Other parameters assessed for their association with the outcome were gender, American Society of Anaesthesiologists (ASA) score (1, 2, and 3 or higher), non-steroid anti-inflammatory drug (NSAID) use at presentation (yes or no), primary or recurrent diverticulitis episode, vomiting (yes or no), and initial antibiotic treatment (yes or no). All risk estimates are expressed in odds ratios (OR) with 95% confidence intervals (CI). These univariable and multivariable analyses were performed with all diverticular complications within three months as outcome and with only infectious complications (perforation or abscess) within three months as outcome. Furthermore, these analyses were repeated with complications within one month as outcome. Last, the three-month analyses were repeated with adjustment for clustering of data. Because the data from two cohorts were used, differences between cohorts in outcome assessment or follow-up could have had an effect on the outcomes. Likewise, differences between hospitals in treatment protocols could have had an effect on the outcomes. To test this bias by clustering of data, the multivariable models were additionally adjusted for study cohort and hospital.
A two-sided p < 0.05 was considered statistically significant. Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for reporting were followed [10]. All analyses were performed using SPSS, version 24.0 (SPSS Inc., IBM, Armonk, NY).
Results
From a total of 1,761 patients in both cohorts, 1,087 CT-proven uncomplicated diverticulitis patients were included. Because 42 patients in the DIABOLO trial had Hinchey Ib (with small diverticular abscess) diverticulitis at presentation, only 486 of 528 patients were included in the present study. From the retrospective cohort study, 601 of 1,233 patients had CT-proven diagnosis of uncomplicated diverticulitis and were included. The mean age was 57.5 (±12.6) years and symptom duration before presentation was median three (2–5) days (Table 1). In this study, 6.8% (74/1087) of the patients did not have follow-up at three months. Because baseline characteristics between these patients, who were lost to follow-up, and patients who were not lost to follow-up were comparable, the risk of attrition bias was considered limited (Supplementary Table S1). Therefore, these patients were labelled in the risk factor analyses as patients that indeed did not develop a complicated disease course within three months after presentation.
Baseline Characteristics of All Hinchey Ia Patients
Values in parentheses are percentages unless indicated otherwise.
Values are mean (standard deviation).
Values are median (interquartile range).
One hundred forty-one missing.
Sixty-one missing.
Thirteen missing.
Fifteen missing.
ASA = American Society of Anesthesiologists.
Complicated disease course of initially uncomplicated diverticulitis
Only 4.9% (53/1087) of the patients developed a complicated disease course within three months: colonic obstruction in 2.1% (23/1087); perforation in 1.2% (13/1087); abscess formation in 0.7% (8/1087); and fistula in 0.8% (9/1087) of all initially uncomplicated diverticulitis patients. Almost half of complications occurred during the first 10 days after presentation (24/53 (45%) of complicated cases) and were somewhat evenly distributed over these days (Figs. 1 and 2). Perforation and abscesses (16/21) predominantly occurred during the first 10 days (Fig. 1) and are shown in more detail in Figure 2. The other five cases of perforation or abscess occurred after 11 to 90 days. Other complications, such as colonic obstruction (23 cases) and fistula (9 cases) occurred during the entire three months of follow-up.

Type of complication (abscess, perforation, obstruction, or fistula) within three months after being diagnosed with acute uncomplicated diverticulitis.
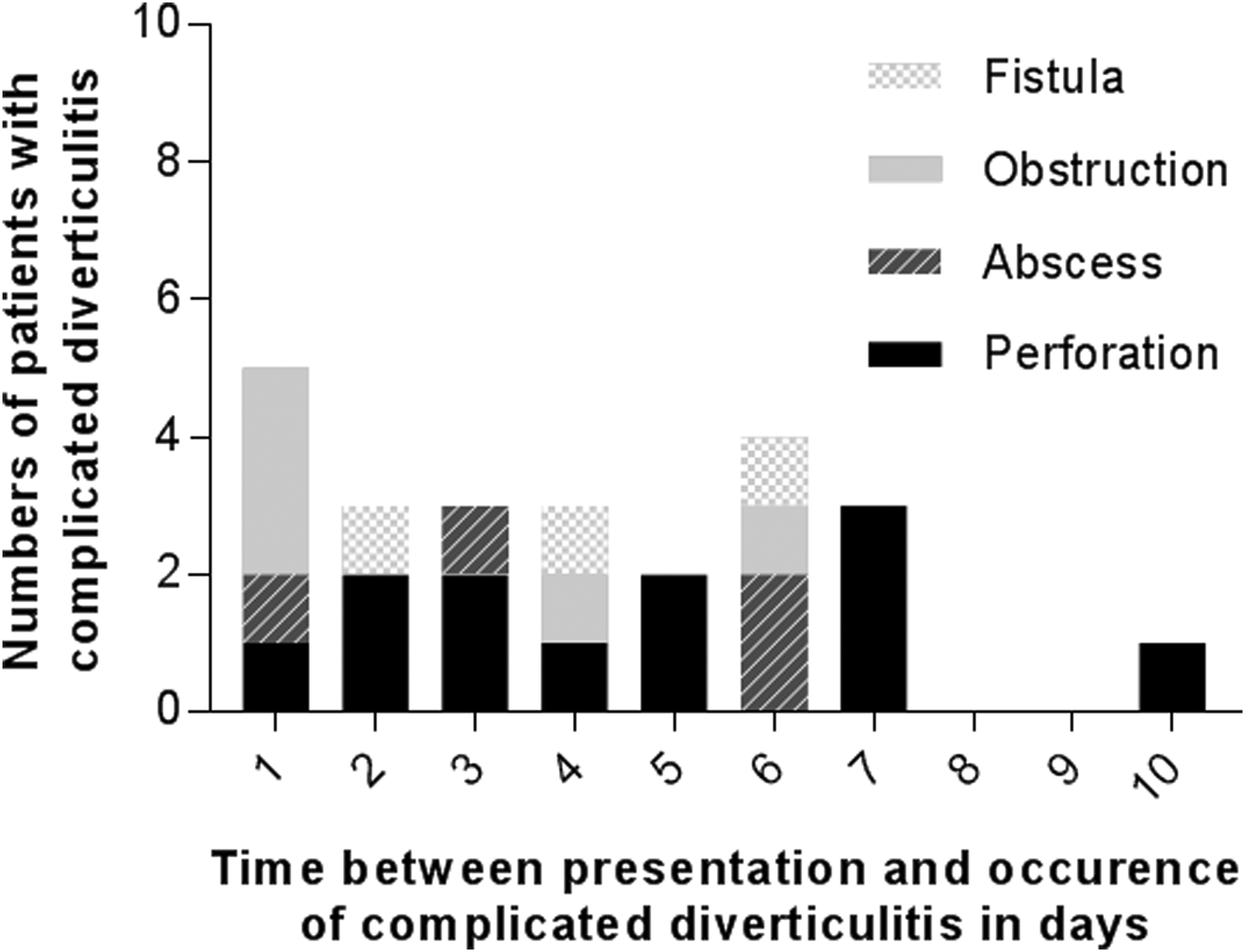
Type of complication (abscess, perforation, obstruction, or fistula) within the first 10 days after being diagnosed with uncomplicated diverticulitis. Day one in this figure represents the day after presentation.
Risk factors for a complicated disease course in initially uncomplicated diverticulitis
The value of optimal sensitivity and specificity according to ROC curves was 140 mg/L for CRP and 15 × 109 cells per liter for WBC (Supplementary Figs. S1 and S2). Independent risk factors for the development of a complicated disease course within three months after presentation were: severe systemic disease ASA 3/4 (OR 4.43, 95% CI 1.57–12.48), duration of symptoms longer than five days before presentation (OR 3.25, 95% CI 1.72–6.13), presence of vomiting (OR 3.94, 95% CI 1.96–7.92), and CRP >140 mg/L (OR 2.86, 95% CI 1.51–5.43) (Table 2).
Univariable and Multivariable Analyses of Risk Factors (Odds Ratio) Associated with a Complicated Disease Course (Abscess, Perforation, Obstruction, or Fistula) within Three Months after Presentation with Acute Uncomplicated Diverticulitis
C-statistic 0.77.
Nine missing.
One hundred forty-one missing.
Twenty missing.
Sixty-one missing.
Fifteen missing.
Thirteen missing.
One missing.
OR = odds ratio; CI = confidence interval; ASA = American Society of Anesthesiologists; NSAID = non-steroidal anti-inflammatory drugs.
Because colonic obstruction and fistula may be considered a different type of complication than the infectious complications perforation and abscess, the logistic regression analysis was repeated only for patients who developed a perforation or abscess as complication. Compared with the risk factors for all types of diverticular complications, ASA score and duration of symptoms were eliminated as risk factors and WBC count appeared to be a new risk factor. For a complicated disease course with perforation or abscess within three months of an initially uncomplicated diverticulitis the following independent risk factors were identified: presence of vomiting (OR 3.53, 95% CI 1.36–9.15), CRP >140 mg/L (OR 3.24, 95% CI 1.36–7.91), and WBC > 15 × 109 cells per liter (OR 3.66, 95% CI 1.50–8.94) (Table 3). Logistic regression for both outcomes at one month of follow-up identified no additional risk factors (Supplementary Tables S2 and S3). Correction for clustering of data yielded comparable results (Supplementary Table S4).
Univariable and Multivariable Analyses of Risk Factors (Odds Ratio) Associated with Abscess or Perforation within Three Months after Presentation with Acute Uncomplicated Diverticulitis
C-statistic 0.78
Nine missing.
One hundred forty-one missing.
Twenty missing.
Sixty-one missing.
Fifteen missing.
Thirteen missing.
One missing.
OR = odds ratio; CI = confidence interval; ASA = American Society of Anesthesiologists; NSAID = non-steroidal anti-inflammatory drugs.
Discussion
Only 4.9% of patients with CT-proven acute uncomplicated diverticulitis developed a complicated disease course within three months after presentation, mostly occurring in the initial 10 days. Patients with uncomplicated diverticulitis at increased risk for diverticular complications had a severe systemic disease according to ASA classification, had more than five days of symptoms before presentation, vomited, had increased CRP levels (>140 mg/L) or increased WBC counts (>15 × 109 cells per liter).
Acute uncomplicated diverticulitis has a benign disease course given the fact that 95% of patients did not develop any diverticulitis-related complication within three months. Several other studies with solely CT-proven uncomplicated diverticulitis patients demonstrate comparable rates. Two retrospective cohort studies have assessed the occurrence of only diverticular complications (perforation, abscess, colonic obstruction or fistula) in initially uncomplicated diverticulitis, showing a 2.0% (16/809) and 2.7% (15/565) complication rate within one month [4,11]. Another retrospective cohort study in uncomplicated diverticulitis only reports rates of inpatient interventions for diverticular complications, that occurred in 3.5% (11/314) of patients [5]. Only two studies have performed a risk factor analysis for the occurrence of diverticular complications [4,5]. With a low number of cases compared with controls, these previous studies were underpowered compared to the present study. Meeting systemic inflammatory response syndrome (SIRS) criteria, increasing age, and immunosuppressive treatment have been identified as risk factors for a complicated disease course [4,5]. Because immunosuppressive treatment has been associated previously with increased risk of complicated diverticulitis at presentation, close observation of these immunosuppressed patients may be appropriate [12]. As a limitation of the present study, immunosuppressive treatment had not been registered and could therefore not be assessed as potential risk factor.
Because of the low number of cases with a complicated disease course, two studies assessed risk factors for combined end point indicating a severe clinical course [5,11]. These combined end points yielded more positive patients that resulted in higher statistically powered analyses. With 46 cases (565 patients) of non-antibiotic treatment failure, a retrospective cohort study identified CRP level above 170 mg/L as a risk factor [11]. However, because this combined end point included non-diverticulitis–related outcomes such as urinary tract infection and pneumonia, generalizability of this findings to patients at risk for diverticular complications is limited. Another study has defined their outcome measure “severe clinical course” as need for surgery, need for percutaneous abscess drainage, length of hospital stay of seven days or longer, or re-admission within 30 days [5]. Also, this study identifies increased CRP level (≥200 mg/L) as an independent risk factor for a severe clinical course. Additionally, use of steroids or immunomodulatory agents, increased body temperature, increased respiratory rate, and a pain score of eight or higher (on a visual analog scale from 0 to 10) are independent risk factors [5].
A previous study using data from the DIABOLO trial has assessed risk factors on CT imaging for the development of complications in initially uncomplicated diverticulitis. This study demonstrates that the presence of fluid collections and a longer inflamed colon segment could have predictive value for a complicated course of initially uncomplicated diverticulitis [7]. Eventually, the combination of published CT parameters and data presented here demonstrated clinical risk factors may provide adequate selection of patients at risk for complications.
A strength of this study is the large number of patients. Fifty-three patients with a relatively rare complicated course of uncomplicated diverticulitis could be evaluated, yielding the statistical power needed for the identification of risk factors. The merge of two data sets was needed to reach this sample size. However, because these populations were similar regarding patient characteristics and treatment protocols, the effect of using two separate data sets was considered limited. Furthermore, all patients had a CT-proven diagnosis of initially uncomplicated acute diverticulitis. However, 632 patients from the retrospective cohort study were excluded because of the absence of a CT-proven diagnosis. It is likely that the patients who did not undergo a CT may have been in a slightly better clinical condition compared with patients who did undergo CT. Therefore, the proportion of patients who developed a complicated disease course may have been slightly overestimated in the present study. Also, five patients developed complicated diverticulitis one day after presentation (one patient a perforation, one patient an abscess, and three patients colonic obstruction requiring surgical intervention). This one-day window in which the complication has developed seems short. It is plausible that some of these complications may have been missed on the initial CT. Another limitation of this study is that data of some potential risk factors described in literature were not available. Specifically, immunosuppressive treatment would have been an interesting factor given the previously reported association with complicated diverticulitis. Although the number of patients was relatively high compared with previous studies, some risk factors may have been missed because of the rarity of complications in the group of uncomplicated diverticulitis patients. Last, most risk factors that were analyzed had relatively low numbers of missing values, except the 141 missing for duration of symptoms.
This study confirmed that clinicians need to be aware of the modest possibility of a complicated disease course (1/20 patients) in initially CT-proven uncomplicated diverticulitis. Patients who fit a profile at risk for the development of a complicated disease course may warrant closer observation during the first week of the disease. Furthermore, previous studies suggest immunocompromised patients may warrant closer observation as well.
Footnotes
Acknowledgments
The DIABOLO trial was funded by The Netherlands Organization for Health Research and Development (ZonMw; 171002303) and Digestive Diseases Foundation (Maag Lever Darm Stichting, MLDS WO08-54).
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.