
Abstract
Abstract
Background:
Guidelines recommend an antimicrobial therapy duration of four to seven days for intra-abdominal infections (IAIs). Despite evidence that shorter treatments are appropriate for this disease state, longer durations frequently are utilized in clinical practice. This study compared the clinical outcomes of short course (SC) and prolonged course (PC) antimicrobial therapy for IAI.
Methods:
This was a noninterventional, retrospective, single-center study. Adults admitted with documented IAI who received antimicrobial treatment for ≥48 hours were included.
Results:
A total of 175 patients were enrolled, 73 patients receiving SC (≤7 days) and 102 patients receiving PC (>7 days) therapy. No significant differences were observed in the primary outcome of clinical cure (74% versus 67.6%; p = 0.367). Secondary outcomes including hospital length of stay (LOS) (5.5 versus 5.8 days; p = 0.372), intensive care unit (ICU) LOS (3 versus 5 days; p = 0.117), 28-day all-cause mortality rate (4.1% versus 2%; p = 0.651), and 30-day re-admission rate (19.2% versus 20.6%; p = 0.818) also were not significantly different.
Conclusions:
There was no significant difference in the rate of clinical cure between SC and PC antimicrobial therapy. These results further support guideline recommendations for a shorter duration of antimicrobial therapy in IAI.
Intra-abdominal infections (IAIs) are associated with a significant morbidity and mortality rate, estimated to be as high as 30%–50% [1,2]. Appropriate management of IAIs requires adequate source control in addition to antimicrobial therapy [3]. Inadequate IAI treatment can lead to complications, including sepsis, extra-abdominal infections, re-infection or death [1,2].
Although antimicrobial therapy clearly reduces the infectious burden and prevents post-surgical infections, its appropriate duration remains a matter for debate [4,5]. The 2010 Infectious Diseases Society of America (IDSA) guideline recommends a treatment duration of four to seven days [3]. Evidence published after the IDSA guideline release also support a duration of less than seven days, specifically for complicated intra-abdominal infections (cIAIs) [5,6]. This recommendation is further supported by the 2017 Surgical Infection Society guideline [7]. Antimicrobial drug use is recommended to be limited to four days in patients with adequate source control and five to seven days in the absence of source control. However, in clinical practice, antimicrobial therapy frequently is administered for longer periods, up to 14 days, because of concern about the lack of clinical resolution [8,9].
Another point to consider is that complications are associated with prolonged antimicrobial therapy for IAIs. Changes in the abdominal flora to select more resistant pathogens has been observed [10]. Additionally, longer treatment is associated with a higher risk of extra-abdominal infections, Clostridium difficile overgrowth, and death [4,9]. From an antimicrobial stewardship perspective, shorter therapy is not associated with higher clinical failure rates in cIAIs and community-acquired IAIs [5,11,12]. Evaluating antimicrobial therapy durations is warranted to minimize drug exposure. The goal of this study was to determine the clinical outcomes of short course (SC) versus prolonged course (PC) antimicrobial therapy for the treatment of IAIs.
Patients and Methods
Study design and subjects
This study was approved by the local Institutional Review Board with a waiver for written informed consent. It enrolled a retrospective, single-center cohort of patients admitted between January 1, 2012, and June 30, 2017, with an IAI. Patients were identified by International Classification of Diseases, Ninth Revision and Tenth Revision (ICD-9 and ICD-10) codes for the following sites of infection: Peritoneal or intestinal abscess or perforation; acute appendicitis or other unspecified disease of the appendix; calculus of the gallbladder or bile duct with acute or chronic cholecystitis; cholangitis or other disorders of the gallbladder, bile duct, or biliary tract including perforation of the gallbladder or bile duct; diverticulitis of the small intestine or colon; acute, chronic, or unspecified gastric, duodenal, peptic, or gastrojejunal ulcer; acute or other chronic peritonitis; and other digestive system complications.
Patients were included if they had at least one sign of IAI, defined as either a white blood cell count (WBC) ≥12,000 or ≤4,000/mm3; a temperature of ≥38°C or ≤36°C; or documented nausea, vomiting, or abdominal pain and were managed with antimicrobial drug(s) for at least 48 hours. Patients with IAI classified as pancreatitis, primary peritonitis, or peritoneal dialysis-related peritonitis; IAI that progressed to bacteremia; and those who were immunocompromised or treated for a concomitant infection at a site other than the abdomen were excluded. Patients were then divided into two groups: Those who received SC antimicrobial therapy (defined as ≤7 days of antimicrobial therapy) or those who received PC therapy (defined as >7 days).
The primary outcome was clinical cure, defined as survival, absence of unplanned repeated intervention, and resolution of signs of IAI at day 10 after antimicrobial initiation or at hospital discharge, whichever occurred first [13]. Secondary outcomes included hospital and intensive care unit (ICU) length of stay (LOS), 28-day all-cause mortality rate, and 30-day re-admission rate.
Data collection
Data were obtained from patients' electronic and paper medical records and entered in a standardized case report form. Data collected included patient demographics, co-morbidities, admitting service, vital signs and laboratory data at admission and discharge or day 10, surgical procedure or other intervention performed, antimicrobial therapy, microbiological data, and clinical outcome.
Statistical analyses
We estimated that a total sample size of 328 patients was needed to detect a 15% difference in the proportion of clinical cure between the groups, assuming a baseline clinical cure rate of 60% among controls, with 80% power and a two-sided 5% level of significance [9].
All statistical analyses were performed using SPSS version 23 (IBM, Armonk, NY). Categorical variables were compared via the Pearson χ2 or Fisher exact test, and continuous variables were compared with the Student t-test or Mann-Whitney U test, as appropriate. All tests of significance were two-tailed, and p < 0.05 was considered statistically significant. A multivariable logistic regression analysis was conducted to determine factors associated with clinical cure. Variables were chosen on the basis of statistical significance (p < 0.05) on univariable analysis or biological plausibility for affecting the outcome. Results are presented as n (%) or median (interquartile range [IQR]) when in tabular format.
Results
During the study period, 839 patients were screened for inclusion (Fig. 1). The primary reason for exclusion was the presence of concomitant infection or bacteremia. A total of 175 patients met inclusion criteria; 73 received SC antimicrobial therapy, and 102 received PC therapy. Baseline characteristics were similar in the two groups with a few exceptions (Table 1). Of note, a higher proportion of patients in the SC group presented with biliary disease (50.7% versus 42.4%; p = 0.015) and a higher proportion with diverticular disease in the PC group (27.3% versus 42.4%; p = 0.045). Additionally, there were more patients in the PC group who received percutaneous drainage (11.0% versus 29.4%; p = 0.004) and more patients in the SC group who underwent a laparoscopic procedure (31.5% versus 11.8%; p = 0.001).
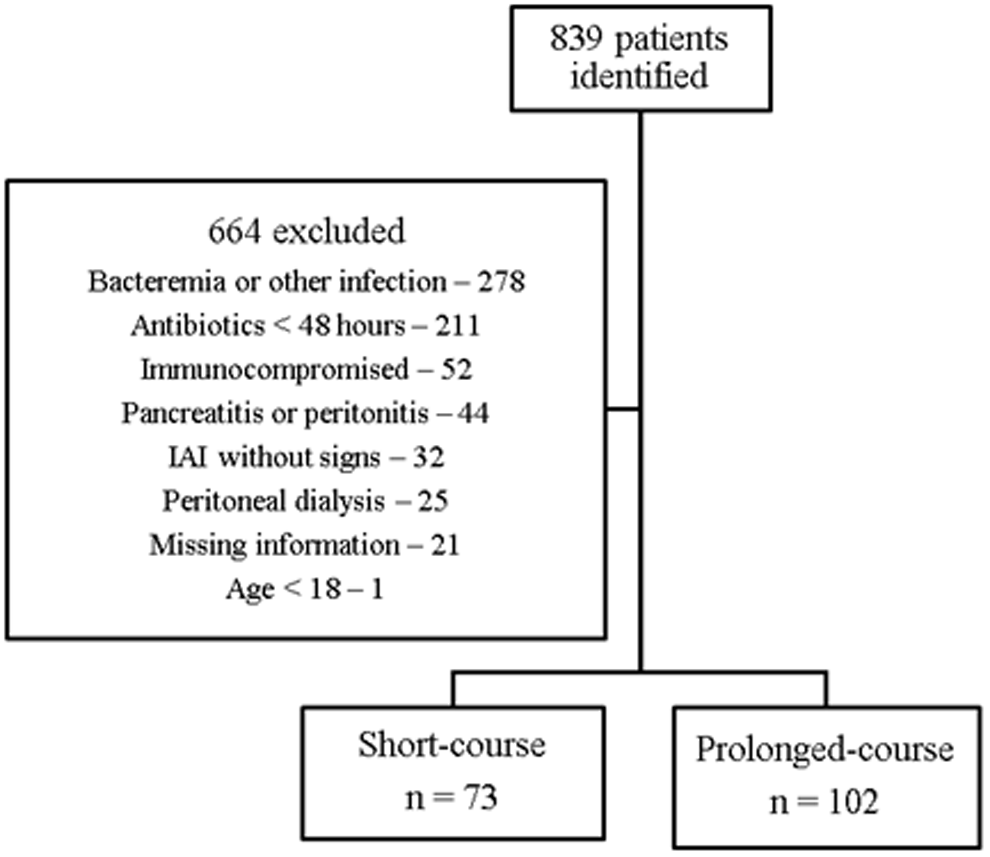
Study enrollment flowchart.
Baseline Characteristics
More than one procedure was possible for a given patient.
CCI = Charlson Comorbidity Index; IAI = Intra-abdominal infection; ICU = intensive care unit; SBO = small bowel obstruction.
Most patients (102/175; 58.3%) received combination antimicrobial therapy, most often with a fluoroquinolone plus metronidazole (51/102; 50.0%) or a cephalosporin plus metronidazole (14; 13.7%). When monotherapy was used (73/175; 41.7%), piperacillin/tazobactam was the most common choice (42/73; 57.5%) followed by a fluoroquinolone alone (10; 13.7%) or metronidazole alone (9; 12.3%).
Of the 54 patients with culture results available, the most common gram-negative organism isolated was Escherichia coli (24%), followed by Enterobacter spp. (14.8%) and Klebsiella spp. (13.0%). The most common gram-positive organism was Enterococcus spp. (18.5%), followed by Staphylococcus spp. (13%) and Streptococcus spp. (7.4%).
The primary outcome, clinical cure, was achieved more frequently in the SC group than in the PC group (74.0% versus 67.6%), but this difference did not reach statistical significance (p = 0.367) (Table 2). Clinical failure occurred most commonly due to persistent signs of IAI, particularly continued WBC abnormalities or documented nausea/vomiting/abdominal pain and unplanned repeated intervention. Secondary outcomes, including hospital and ICU LOS, 28-day all-cause mortality rate, and 30-day all-cause re-admission, again were not significantly different in the two groups. Of course, there was a significant difference in the median duration of antimicrobial therapy received in the two groups (4 days versus 13 days; p < 0.001), reflective of treatment group assignment.
Clinical Outcomes
Patients may have had more than one reason.
IAI = intra-abdominal infection; ICU = intensive care unit; LOS = length of stay; WBC = white blood cell count.
A multivariable logistic regression was conducted to account for the retrospective nature of the study. This analysis evaluated factors associated with clinical cure. The variables examined were the duration of therapy, receipt of percutaneous drainage or a laparoscopic procedure, infection from a biliary or diverticular source, admission to the ICU, and monotherapy versus combination therapy. The only variable independently associated with clinical cure was infection from a diverticular source (odds ratio 0.34; 95% confidence interval 0.13–0.85; p = 0.022).
Discussion
To the best of our knowledge, this is the first study to evaluate treatment of a heterogeneous IAI patient population. Previous studies have evaluated solely cIAI or community-acquired IAI. Our study found no difference in the clinical cure rate according to the antimicrobial therapy duration. Other clinical outcomes also were not impacted by antimicrobial therapy duration.
The clinical cure rate for IAI is reported at various frequencies between 20% and 90%, depending on the patient population studied [5,6,11,14]. The rate of clinical cure in the present study was similar to the rates observed in previous studies [5,11]. Sawyer et al. evaluated a treatment duration of 10 days versus four days in patients with cIAI following adequate source control and found a clinical cure rate >70% in both groups [5]. A trial conducted by Basoli et al. found clinical cure rates higher than in our patient population of approximately 90% in patients receiving either three or greater than five days of ertapenem therapy for community-acquired IAI [11]. Studies evaluating a solely ICU patient population with cIAI have, as expected, found lower rates of clinical cure than in the present study [6,14]. Our baseline expected rate of clinical cure of 60% was chosen because of the heterogeneous patient population. In contrast to previous studies, not all patients underwent source control given the nature of their IAI (i.e., diverticulitis). The present study provides additional information on anticipated rates of clinical cure for IAI, an area with limited data on expected outcomes.
The most common causes of clinical failure in this cohort were continued abnormalities in WBC count, unplanned repeated intervention, or persistent nausea, vomiting, or abdominal pain. Because of the retrospective nature of this study, we cannot determine the reason for antimicrobial continuation; however, prolonged therapy given a persistently abnormal WBC count is a common reason identified in previous literature [8,9]. The usual reason for protocol deviation from shortened antimicrobial therapy in the study by Sawyer et al. also was an abnormal WBC count [5].
The most common antimicrobial drugs utilized in this study were piperacillin/tazobactam for patients receiving monotherapy and a fluoroquinolone and metronidazole for patients receiving combination therapy. These regimens are consistent with recommendations from the IDSA [3]. Limited data exist on the specific agents used for shorter antimicrobial durations for IAIs. Most previous studies did not report on drug-specific outcomes [5,6]. The use of fluoroquinolones is frequent in clinical practice for treatment of IAI. Shortened duration of this therapy is imperative because of the risk of Clostridium difficile overgrowth associated with prolonged antimicrobial administration in IAI and the inherent risk with this class of medications [15]. According to the bacteria isolated in this patient population, the most frequent therapies utilized were appropriate. Isolation of enterococci and E. coli were most frequent in this cohort, which is consistent with the findings in previous studies [3,14].
This study has several strengths. We evaluated a diverse IAI patient population and included both complicated and uncomplicated infections. The median durations of therapy were significantly different and clinically meaningful. The methods utilized to account for confounders or potential bias also contribute to the strength of this analysis.
Limitations of this study include the sample size and the population not meeting power standards. This may be a result of the strict inclusion and exclusion criteria chosen in order to evaluate a patient population representative of the study question. Because of the retrospective nature of this analysis, there is a potential for unaccounted for variables to impact the outcomes. A multivariable logistic regression was used to help control for identified or presumed differences between treatment groups. Additionally, there is not a standard definition of clinical cure or failure for IAI. The definition used in this study was similar to that in previous analyses, but future studies should specify the most accurate definition to use in this patient population. Lastly, other complications associated with prolonged treatment such as the appearance of Clostridium difficile or multidrug-resistant infections were not assessed.
This study did not detect a difference in the clinical cure rate between patients treated with less than or equal to seven days versus greater than seven days of antimicrobial drug(s) for IAI. Treatment of IAI should be limited to less than seven days, which is in accordance with the current IDSA guideline. In this study, prolonged antimicrobial therapy did not improve outcomes in IAI.
Footnotes
Acknowledgment
The results of this study were presented at IDWeek 2018, San Francisco, CA, October 3–7, 2018.
Author Disclosure Statement
No competing financial interests exist. This study was carried out as part of our routine work.