
Abstract
Background:
The Augmented Renal Clearance in Trauma Intensive Care (ARCTIC) scoring system is a validated system to predict augmented renal clearance in trauma patients. This study examined the ability of the ARCTIC score to identify patients at risk for subtherapeutic vancomycin trough concentrations relative to estimated creatinine clearance (eCrCl) alone.
Methods:
Trauma patients admitted to the intensive care unit from September 2012 to December 2017 who received vancomycin and had a vancomycin trough concentration recorded were included. Patients were excluded if their serum creatinine concentration was >1.3 mg/dL, if they had received vancomycin doses <30 mg/kg per day, an improperly timed trough concentration measurement, or renal replacement therapy. The primary endpoint was an initial subtherapeutic vancomycin trough concentration (<10 mg/L). Classification and regression tree (CART) analysis was used to identify thresholds for the ARCTIC score and other continuous data where subtherapeutic troughs were more common. A step-wise logistic regression analysis was performed to control for confounders for subtherapeutic troughs whereby inclusion of ARCTIC was modeled sequentially after eCrCl.
Results:
A total of 119 patients with a mean age of 42 ± 17 years and eCrCl 142 ± 39 mL/min met the inclusion criteria. The mean daily vancomycin dose was 44 ± 9 mg/kg, and the incidence of subtherapeutic trough concentration was 46%. The CART analysis identified two variables creating three groups where subtherapeutic trough concentrations differed: eCrCl >105 mL/min and ARCTIC score ≥7, eCrCl >105 mL/min and ARCTIC score <7, and eCrCl ≤105 mL/min. The base logistic regression model identified eCrCl >105 mL/min and pelvic fracture as risk factors for subtherapeutic trough values. The final model included the addition of ARCTIC score ≥7, which improved the model significantly (p = 0.009). Predictors of subtherapeutic trough concentrations were (odds ratio [95% confidence interval]): eCrCl >105 mL/min (6.5 [1.66–25.07]), ARCTIC score ≥7 (3.26 [1.31–8.09]), and pelvic fracture (4.36 [1.27–14.93]).
Conclusion:
The ARCTIC score is useful when applied in conjunction with eCrCl. Patients with a eCrCl >105 mL/min and an ARCTIC score ≥7 may require a more aggressive dosing strategy.
The development of renal hyperfiltration, a phenomenon commonly referred to as augmented renal clearance (ARC), has been observed in 30%–65% of critically ill patients [1]. Recent literature has demonstrated a clear association between ARC and subtherapeutic tissue concentrations of antimicrobial drugs, which contributes to the inability to reach established pharmacodynamic goals [2]. Vancomycin, which is used routinely for coverage of methicillin-resistant Staphylococcus aureus, undergoes significant renal clearance and consequently is affected by ARC. Thus, there is tremendous potential for under-dosing in populations with ARC who are treated with vancomycin.
Several studies have demonstrated the difficulties of reaching the pharmacodynamic goals established for vancomycin in the presence of ARC. In one study of critically ill patients admitted to two intensive care units (ICUs), patients exhibiting ARC were at nearly twice the risk of subtherapeutic vancomycin concentrations as patients without ARC [3]. In another study of 363 patients admitted to a clinical–surgical ICU, patients exhibiting ARC had significantly lower concentrations of vancomycin within the first 72 hours of treatment despite receiving nearly 50% higher doses than patients without ARC [4].
The timely identification of patients with ARC is the critical first step in allowing clinicians to mitigate the risk of subtherapeutic vancomycin concentrations pre-emptively. However, identifying patients with ARC prior to therapy is difficult because creatinine clearance (CrCl) estimations leads to underestimation of clearance in this population [5]. Additionally, measurement of urinary CrCl can take up to 24 hours to complete; therefore, it does not provide the information needed to minimize under-dosing during the critical early hours of therapy. As a result, predictive scoring models have been developed to aid in identifying patients at risk of ARC at the onset of therapy.
The Augmented Renal Clearance in Trauma Intensive Care (ARCTIC) scoring system is a predictive model specific to trauma patients that can be used to screen those at risk for ARC [6]. Although ARCTIC identifies patients at risk of ARC, it has yet to demonstrate a capacity to predict subtherapeutic antimicrobial concentrations directly. The objective of this study was to evaluate the ability of an ARCTIC score to identify patients at risk for subtherapeutic vancomycin trough concentrations relative to CrCl estimates alone.
Patients and Methods
Institutional Review Board approval was obtained prior to study initiation. This retrospective cohort study included all patients who were admitted to the ICU of a Level 1 Trauma Center for a trauma-related diagnosis between September 2012 and December 2017 and who were initiated on vancomycin and had at least one vancomycin trough concentration recorded. Patients were excluded if the baseline serum creatinine (SCr) was >1.3 mg/dL or they were receiving renal replacement therapy at the time of initiation of therapy, had an inappropriately timed vancomycin trough measurement (i.e., more than two hours before or after the scheduled time), or received a dosing regimen of <30 mg/kg/day.
Data abstracted from the electronic medical records included patient demographics, injury type, Injury Severity Score (ISS), SCr, vancomycin dosing regimen, and vancomycin trough concentrations. Creatinine clearance was estimated using the Cockcroft–Gault equation (eCrCl).
A standardized vancomycin dosing protocol was used to administer and monitor vancomycin use. Intermittent vancomycin maintenance doses are between 15–20 mg/kg administered at a frequency determined by the eCrCl. Loading doses are considered for critically ill patients. Serum samples for vancomycin trough concentration measurements are drawn approximately 30 minutes prior to the fourth drug dose.
The primary outcome was an initial subtherapeutic vancomycin concentration, defined as a first trough value <10 mg/L. Patients were stratified into two cohorts on the basis of this trough value, and variables were compared for the groups. Normally distributed continuous data were compared using the Student t-test, and the Mann-Whitney U test was used for data that were skewed. Analysis of variance was used when there were more than two groups. Dichotomous data were compared using either the Pearson χ2 or the Fisher exact test. An ARCTIC score (Table 1) was calculated for each patient for the day on which vancomycin therapy was initiated. Classification and regression tree analysis was used to identify thresholds for the ARCTIC score and other continuous data where subtherapeutic vancomycin troughs were more common. To identify factors associated with subtherapeutic vancomycin trough concentrations, univariable analysis was conducted; and variables with a p value <0.1 were considered for inclusion in the multivariable model. Multivariable regression analysis was performed in a step-wise fashion whereby inclusion of ARCTIC was modeled sequentially. An omnibus test of model coefficients was performed to assess for improvement over the baseline model. A p value <0.05 defined statistical significance. All statistical analyses were performed using SPSS software, version 23 (IBM, Armonk, NY).
Augmented Renal Clearance in Trauma Intensive Care (ARCTIC) Scoring System
Results
A total of 182 patients admitted with a trauma-related diagnosis were treated with vancomycin during the study period. Of these, 119 patients met the criteria for inclusion (Fig. 1). Their mean age was 42 ± 17 years, and the mean eCrCl was 142 ± 39 mL/min (Table 2). The most common injury type was traumatic brain injury (61%), and the mean calculated ARCTIC score was 6.3 ± 1.4.
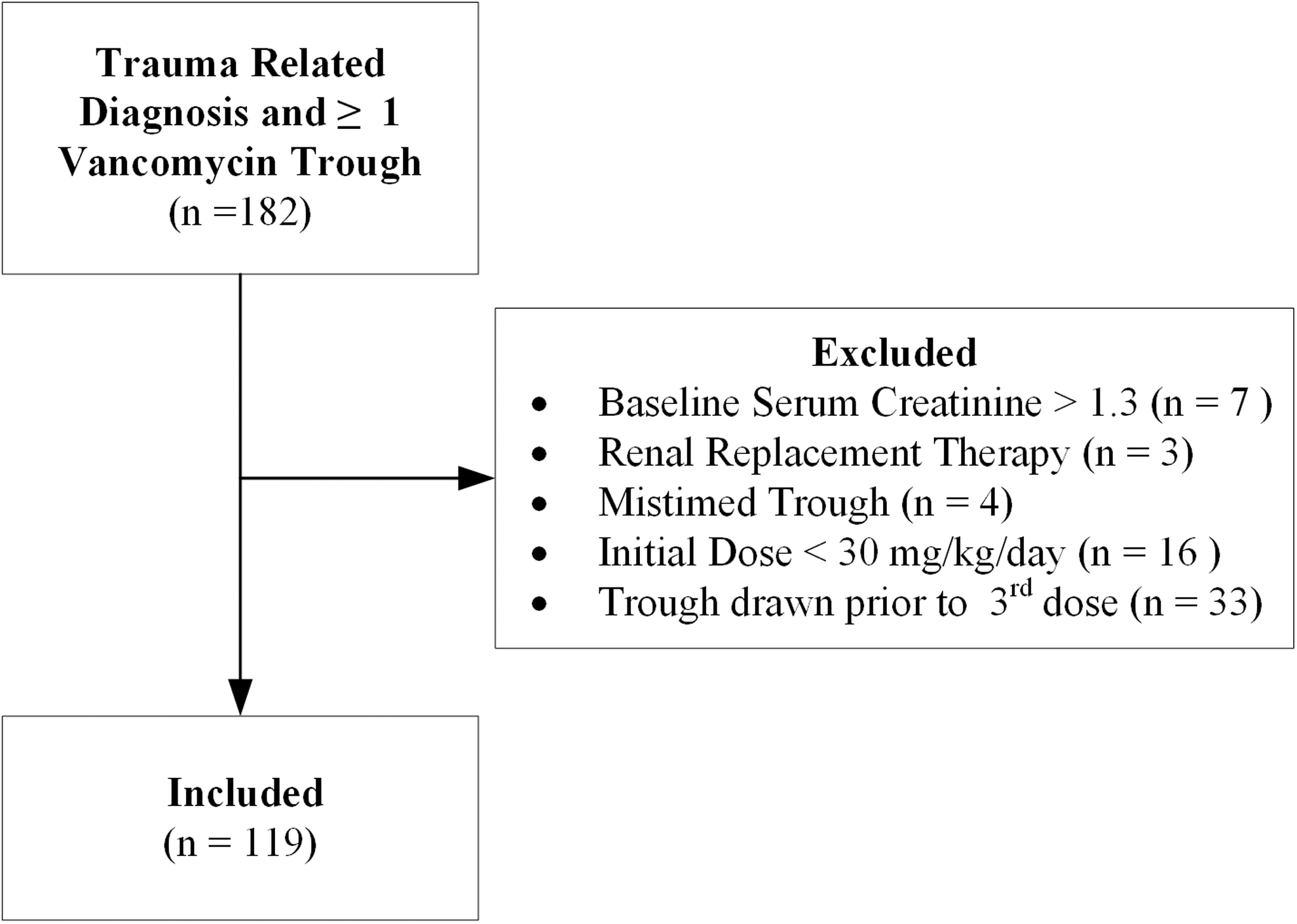
Patient selection flow chart.
Baseline Characteristics of 119 Patients
All data are presented as either mean±standard deviation or number (%).
ARCTIC = Augmented Renal Clearance in Trauma Intensive Care; CrCl = creatinine clearance; SCr = serum creatinine concentration.
Patients received an initial vancomycin daily dose of 44 ± 9 mg/kg. The mean vancomycin trough value was 10.7 ± 4.5 mg/L. Subtherapeutic troughs were noted in 55 patients (46.2%) (Fig. 2).
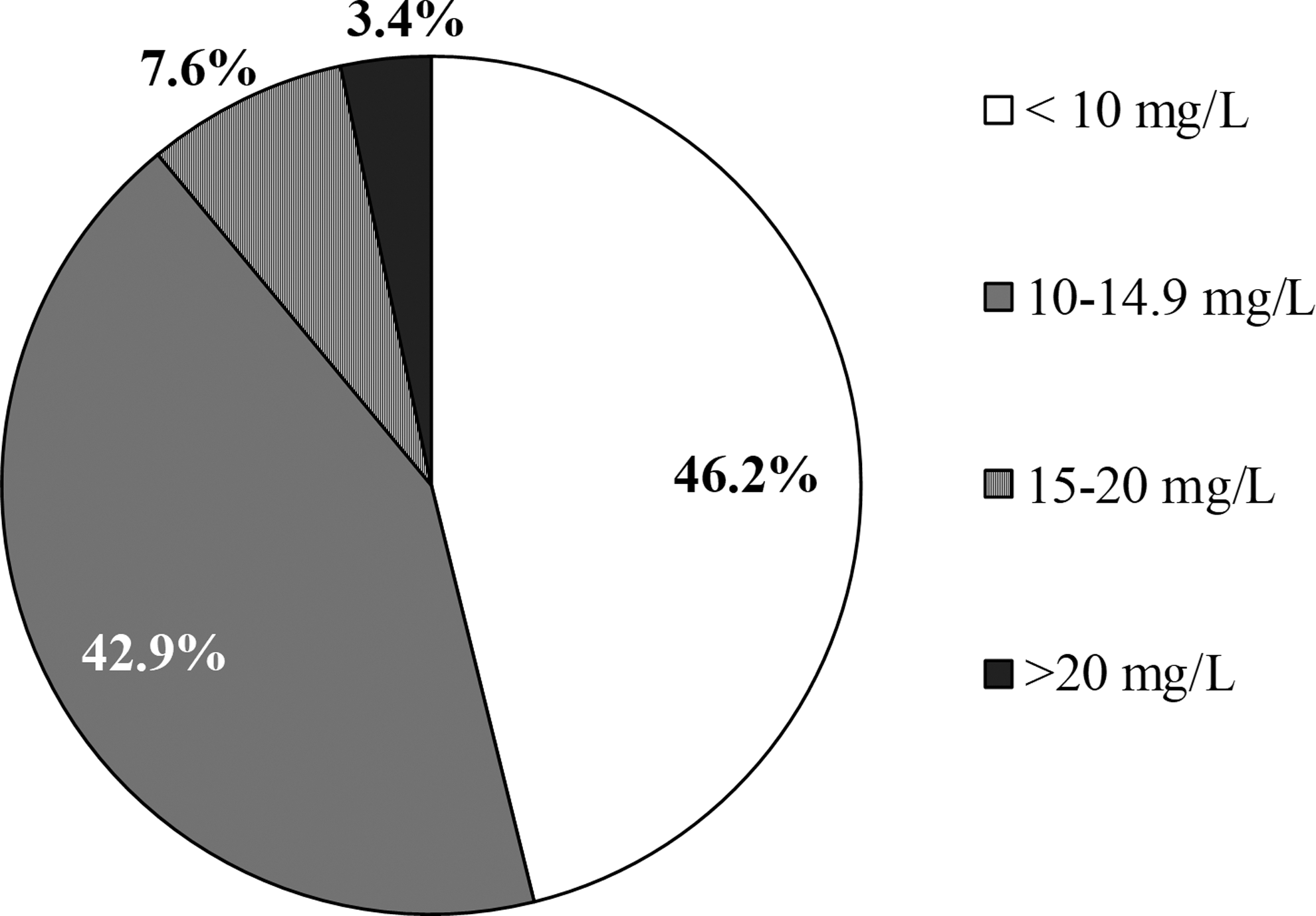
Distribution of initial vancomycin trough concentrations.
Classification and regression tree analysis identified two variables (eCrCl and ARCTIC) forming three groups where the incidence of subtherapeutic troughs differed: eCrCl >105 mL/min and ARTIC ≥7, eCrCl >105 mL/min and ARCTIC <7, and eCrCl ≤105 mL/min (Fig. 3). Vancomycin dosages were similar in these three groups (44 ± 8 versus 44 ± 10 versus 41 ± 7 mg/kg/day, respectively; p = 0.228). Univariable analysis identified several factors that were associated with subtherapeutic trough values, including ARCTIC score and eCrCl (Table 3). The multivariable model included the following variables: eCrCl >105 mL/min, pelvic fracture, average vancomycin dose/day, and ARCTIC score ≥7. The final model revealed ARCTIC score ≥7, eCrCl >105 mL/min, and pelvic fracture to be risk factors for subtherapeutic vancomycin trough concentrations. The addition of ARCTIC improved the model significantly (p = 0.009) (Table 4).
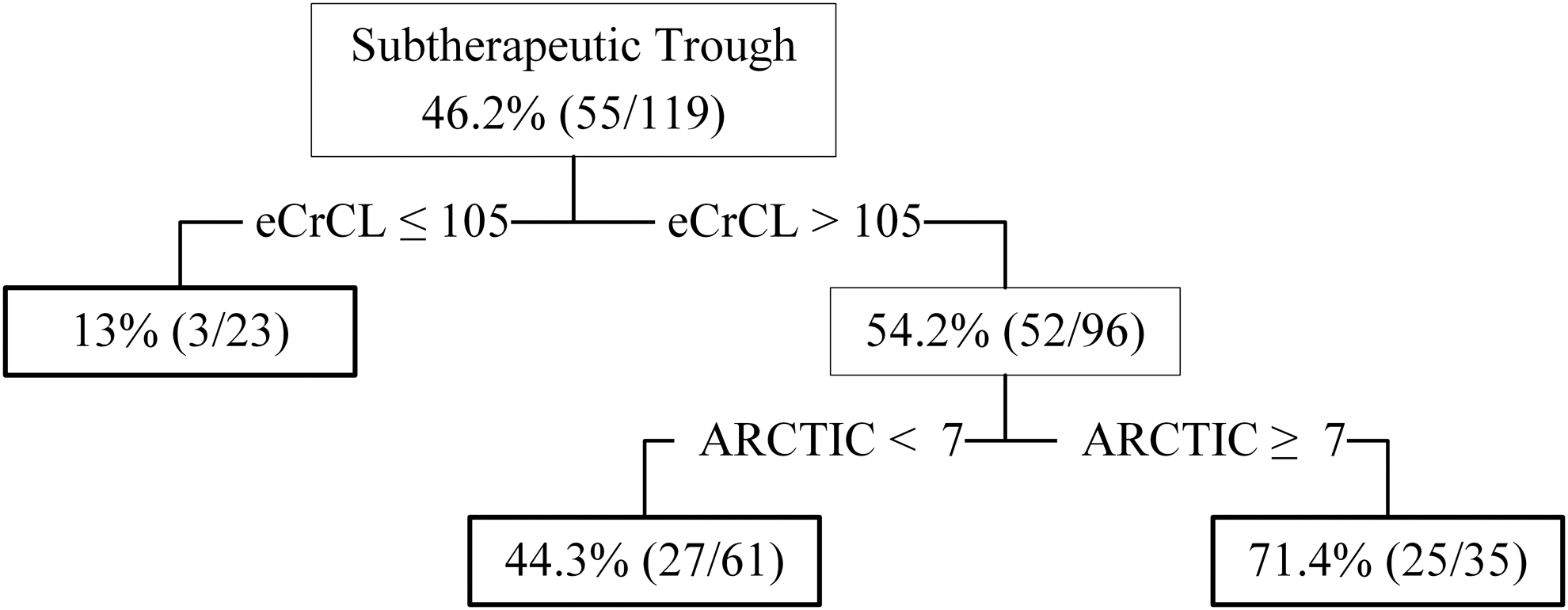
Decision tree analysis of factors associated with subtherapeutic vancomycin trough concentrations.
Univariable Analysis of Variables Associated with Subtherapeutic Vancomycin trough Concentrations
All data are presented as either mean ± SD or number (%).
ARCTIC = Augmented Renal Clearance in Trauma Intensive Care; eCrCl = estimated creatinine clearance; SCr = serum creatinine concentration.
Multivariable Analysis of Variables Associated with Subtherapeutic Vancomycin trough Concentrations
Omnibus test of model coefficients comparing Model 1 with Model 2: p = 0.009.
ARCTIC = Augmented Renal Clearance in Trauma Intensive Care; eCrCl = estimated creatinine clearance.
Discussion
The presence of ARC is common in critically ill populations and represents a significant hurdle in reaching pharmacodynamic goals, particularly with renally eliminated antimicrobial drugs such as vancomycin. One study of patients treated with vancomycin stratified the achievement of trough concentrations by CrCl subgroup [7]. In the subgroup with CrCl >130 mL/min, 62.9% of patients did not reach a vancomycin trough concentration of 10 mg/L. Another study examined vancomycin concentrations in critically ill septic patients having vancomycin administered by continuous infusion. On the first day of therapy, 89% of the patients with ARC had subtherapeutic vancomycin concentrations compared with 53% of the group without ARC [8]. These data highlight the difficulty in achieving adequate vancomycin concentrations in critically ill populations, particularly in patients with ARC.
Several studies have described the relation between rapid achievement of vancomycin pharmacodynamic targets and the effect on clinical outcomes. The currently accepted pharmacodynamic target for vancomycin is an area under the curve to minimum inhibitor concentration (AUC/MIC) ≥400 due to achievement of bacterial eradication and improved clinical response [9,10]. In a study of patients with bacteremia being treated with vancomycin, achievement of target AUC/MIC on day one of therapy was associated with a 2–2.5-fold reduction in the 30-day mortality rate [11]. A recent meta-analysis of nine cohort studies demonstrated that an AUC/MIC ≥400 was associated with a lower mortality rate (relative risk [RR] 0.47; 95% confidence interval [CI] 0.31–0.70); p < 0.001] and treatment failure (RR 0.39; 95% CI 0.28–0.55; p = 0.001) compared with AUC <400 [12].
Previously, it was demonstrated that the use of CrCl estimations carries a high risk of bias compared with measured urinary CrCl, particularly when CrCl is elevated [5]. We demonstrated that the addition of ARCTIC when eCrCl is >105 mL/min can improve the ability of clinicians to discern trauma patients at risk of subtherapeutic vancomycin concentrations. Risk factors associated with subtherapeutic vancomycin trough concentrations in our study were CrCl >105 mL/min, ARCTIC ≥7, and pelvic fracture. Of note, pelvic fractures have not been reported previously to influence vancomycin dosing. Earlier studies evaluated vancomycin pharmacokinetic parameters in trauma patients and reported a high degree of inter-patient variability and unexplained variance [13]. This finding illustrates the complexity of vancomycin dosing in this population and the numerous factors that can affect dose outside of the variables that routinely are considered (i.e., age, weight, CrCl). For these reasons, the optimal approach to vancomycin dosing remains elusive in trauma populations, as many studies have demonstrated inadequate attainment of therapeutic concentrations [14,15].
Although ARC most commonly has been defined as CrCl >130 mL/min in the literature, our finding that the CART-derived eCrCl of >105 mL/min were at significantly greater risk of subtherapeutic vancomycin trough values has implications for the design of vancomycin dosing protocols. Many hospitals have implemented protocols that do not differentiate between patients with adequate renal function and those with supraphysiologic renal function (e.g., the same dose is given to any person with eCrCl >90 mL/min). However, several studies have demonstrated a clear association between elevated CrCL and decreased vancomycin concentrations. Minutke et al. showed that each 40 mL/min increase in eCrCl correlates with a decrease in initial vancomycin trough concentration by 1.49 mg/L [3]. Another study found a log-linear relation between steady-state vancomycin trough concentrations and various CrCl subgroups whereby troughs were lower with increasing CrCl values [7]. In order to optimize the dosing of vancomycin, protocols must differentiate patients who are unlikely to reach pharmacodynamic goals at conventional doses. Furthermore, it is important that protocols reflect differences between patients with normal and elevated eCrCl and patients exhibiting ARC and, further, differentiate between patients with various degrees of ARC. Finally, as higher than typical doses of vancomycin have been necessary for patients with ARC, absolute dose ceilings should be discouraged in these populations.
Several limitations are evident when interpreting the results of our study. First, this was a single-center, retrospective study and therefore is subject to the biases inherent to this design. Second, we were unable to measure vancomycin AUC/MIC [9]. Vancomycin trough concentrations can be interpreted only as a surrogate target, and there are studies showing a lack of correlation between vancomycin trough concentrations and AUC/MIC [16]. However, vancomycin trough concentration represents the most common variable used for therapeutic drug monitoring. Further research is needed examining the probability of attaining AUC/MIC targets in patients exhibiting ARC. Finally, the purpose of our study was to evaluate the pharmacokinetics of vancomycin in patients at risk for ARC and not clinical outcomes. Further outcome research is necessary.
In conclusion, the incidence of subtherapeutic vancomycin trough concentrations is high, and the addition of the ARCTIC score to conventional eCrCl may assist in identifying at-risk patients. Clinicians should screen all critically ill trauma patients for risk factors for ARC, particularly in those being considered for treatment with vancomycin. Future studies are needed to evaluate dosing strategies that will optimize vancomycin pharmacodynamics and clinical outcomes in this population.
Footnotes
Acknowledgment
Abstract presented as platform at the 48th Critical Care Congress of the Society of Critical Care Medicine, San Diego, California, February 19, 2019.
Author Disclosure Statement
All authors report that no competing financial interests exist.