
Abstract
Background:
Antimicrobial drug resistance in community-acquired (CA) infections is a growing problem. Knowing the local epidemiology is essential to design empirical antibiotic therapy. Therefore, we conducted this study to evaluate the resistance patterns of microorganisms isolated from surgical samples of community-acquired intra-abdominal infections (IAIs) and to determine the factors associated with resistance.
Methods:
We analyzed retrospectively the records of patients treated from January 2015 to June 2017 who had IAIs with positives aerobic cultures performed in the first 72 hours after admission. Surgical site infections, abdominal wall procedures, peritoneal dialysis catheters, and patients with admissions in the prior month were excluded. To identify the factors associated with resistance, we considered the resistance to the regimen recommended at our institution, ampicillin/sulbactam (AMS) plus ciprofloxacin (CIP).
Results:
There were 119 patients with 133 isolates, 59% women, and mean age 54 years. The main sources of infection were appendicitis (38%) and cholecystitis (20%), with 64 patients presenting a complicated IAI (cIAI), defined by the presence of peritonitis (55%). Resistance in Enterobacteriaceae was AMS 32% (6.4% intermediate resistance), CIP 31%, cefotaxime 9%, piperacillin/tazobactam (PTZ) 3%, trimethoprim/sulfamethoxazole 32%, gentamicin 9.5%, and amikacin 2%. Considering all patients, resistance to AMS + CIP was 16.8%. Factors associated with resistant to this regimen was, by univariable and multivariable analysis, the presence of diabetes mellitus (odds ratio [OR] 3.6; 95% confidence interval [CI] 1.1–11.6; p = 0.03). Female gender (OR 2.7; CI 0.9–8.4; p = 0.08) and complicated IAI (OR 2.0; CI 0.7–5.4; p = 0.17) were associated with resistance but did not reach statistical significance.
Conclusion:
High resistance to CIP and AMS was observed. Although the combination of AMS + CIP offers coverage for 84% of patients, PTZ should be considered as an option for patients with severe infections or diabetes mellitus. Finding factors associated with antibiotic resistance could help to select empirical therapy for CA IAIs better.
Antimicrobial resistance (AMR) is a global threat projected to be one of the leading causes of death in the near future [1]. Resistance is increasing, not only in nosocomial infections but in community-acquired (CA) infections as well [2,3].
Intra-abdominal infections (IAIs) are one of the most common requiring hospital admission [4,5]. Appropriate empirical antibiotic therapy (EAT) in IAIs is associated with better patient outcomes, shorter length of stay, and lower costs, especially in patients with complicated IAIs (cIAIs) or patients presenting with sepsis or septic shock [6–9]. Knowing local AMR patterns and risk factors for acquisition of resistant microorganisms is key to deciding on the optimal EAT [10]. Considering community gram-negative isolates commonly involved in IAIs, such as Escherichia coli and Klebsiella pneumoniae, the rate of resistance to first-line antibiotics such as ciprofloxacin (CIP) and ampicillin/sulbactam (AMS) in our country is around 31.7–35% and 19%–34.3%, respectively [11,12]. However, little is known about the risk factors for AMR in IAI isolates. Detecting patients at high risk of AMR could help select patients with IAI who would benefit from broader-spectrum antimicrobial drugs, as well as to optimize antibiotic stewardship policies.
We designed this study to describe the resistance patterns of CA IAI isolates from surgical samples to assess the effectiveness of our EAT (AMS plus CIP) and to determine the factors associated with resistance to those antibiotics.
Patients and Methods
Study population
Sanatorio Güemes, Buenos Aires, Argentina, is a 680-bed acute-care general hospital. We analyzed the medical records of earlier patients with intra-abdominal surgery and positive aerobic cultures. Adult patients who underwent intra-abdominal surgery involving the peritoneal cavity at our institution from January 2015 to June 2017 were included if they had at least one positive aerobic isolate from intra-abdominal samples (peritoneum or visceral samples, including both hollow and solid viscera). We chose patients who had their operations performed within the first 72 hours after admission in order to exclude patients with hospital-acquired IAIs. The other exclusion criteria were surgical site infections, infections limited to the abdominal wall or abdominal wall procedures, peritoneal dialysis catheter infections, primary peritonitis such as spontaneous bacterial peritonitis, and patients with admissions in the last month.
Case selection and examination
Case identification was triggered using electronic medical records after detecting at least one positive aerobic culture from a peritoneal or visceral sample. Polymicrobial cultures in which no predominant isolate(s) could be identified were excluded. We collected demographic data, type of surgical procedure, source of IAI, presence of peritonitis, admissions in the last six months, co-morbidities (malignant disease, diabetes mellitus, chronic renal failure, obesity, and immunosuppression), the antimicrobial therapy prescribed, and the antibiotic susceptibility of the isolate(s). Peritonitis was defined by surgical findings of peritoneal infection. Patients with peritonitis were considered to have a cIAI, whereas those with infection limited to the viscera, without peritoneal involvement, were considered to have an uncomplicated IAI (uIAI).
To assess the activity of the EAT recommended at our institution (AMS plus CIP), we considered all isolates from each patient, irrespective of the antimicrobial drug actually prescribed. The AMS plus CIP was considered adequate if all the patient's isolates were susceptible to at least one of the antibiotics, whereas if the patient had at least one isolate not susceptible to the recommended combination, the regimen was considered inadequate. The particular regimen was defined by the infectious diseases team on the basis of an earlier analysis of microbiologic data from IAI at our institution, taking into account resistance selection, adverse reactions, and the cost of other options. Antimicrobial susceptibility was determined by disk diffusion and automated methods (BD Phoenix™) according to the Clinical and Laboratory Standards Institute recommendations.
Given the retrospective nature of the study, no informed consent was required. The study was approved by the Institutional Research Department. All data were kept confidential, and the study was carried out according to the Helsinki Declaration.
Statistical analysis
Stata® 13 (Statistics/Data Analysis, Stata Corp LP, College Station, TX USA) was used for statistical analysis. Continuous variables are expressed as mean and standard deviation, and qualitative variables are shown as frequencies and percentages. The χ2 test was used to compare qualitative variables and the Student t-test to compare continuous variables. A two-sided p value <0.05 was considered statistically significant. A multivariable analysis was performed using logistic regression to assess factors associated with isolates resistant to the EAT (AMS plus CIP). Adjusted odds ratios (ORs) and their 95% confidence interval (CI) are provided.
Results
Patient characteristics
During the period studied, we identified 119 patients with 133 bacteriologic isolates from intra-abdominal samples. Patient characteristics, source of IAI, and co-morbidities are shown in Table 1. Female gender was slightly more frequent. Appendicitis and cholecystitis accounted for more than half of the IAIs. There were eight isolates from solid organ infections (five hepatic and three pancreatic), and 55% of the patients were considered to have a cIAI on the basis of the presence of peritonitis, localized or generalized. Malignant disease was a frequent co-morbidity followed by diabetes mellitus.
Demographic Characteristics of Patients
Prior admission 30–180 days before present admission.
IAIs = intra-abdominal infection; IQR = interquartile range; SD = standard deviation.
Microbiology results
Ten patients (7.5%) had more than one isolate from IAI samples (range two to four). Table 2 shows all identified isolates. The number of gram-negative bacilli (GNB) and gram-positive cocci were 104 (78.2%) and 27 (20.3%), respectively, whereas 2 (1.5%) Candida spp. were obtained. Escherichia coli accounted for more than half of the isolates, followed by Streptococcus spp., all belonging to the viridans group (VGS). Among GNB, Enterobacteriaceae accounted for 89.4%.
Microorganisms Isolated
There were six Enterobacteriaceae, four Aeromonas spp., and one Haemophilus influenzae.
Empirical antibiotics prescribed
The most frequent combination of antimicrobial drugs prescribed was AMS plus CIP in 55 patients (46%), followed by AMS in 31 (26%), piperacillin/tazobactam in 8 (7%), CIP plus metronidazole in 7 (6%), and other antibiotics in 18 patients (15%).
In vitro antibiotic susceptibilities and regime activity
Antibiotic resistance patterns for Enterobacteriaceae are shown in Fig. 1. Strains not susceptible to AMS accounted for 38.7% of the isolates, and resistance to CIP was apparent in 32.6%. A few of the strains (9.7%) were resistant to cefotaxime, this being more frequent in K. pneumoniae (22.2%). The agents most active against Enterobacteriaceae were PTZ and amikacin (resistance in 3.2% and 2.1% of strains, respectively). Against Pseudomonas spp., five of the six isolates were susceptible to CIP. Among GBP, all Streptococcus spp. were susceptible to penicillin, and two of the five strains of Enterococcus spp. (both E. faecium) were resistant to ampicillin.
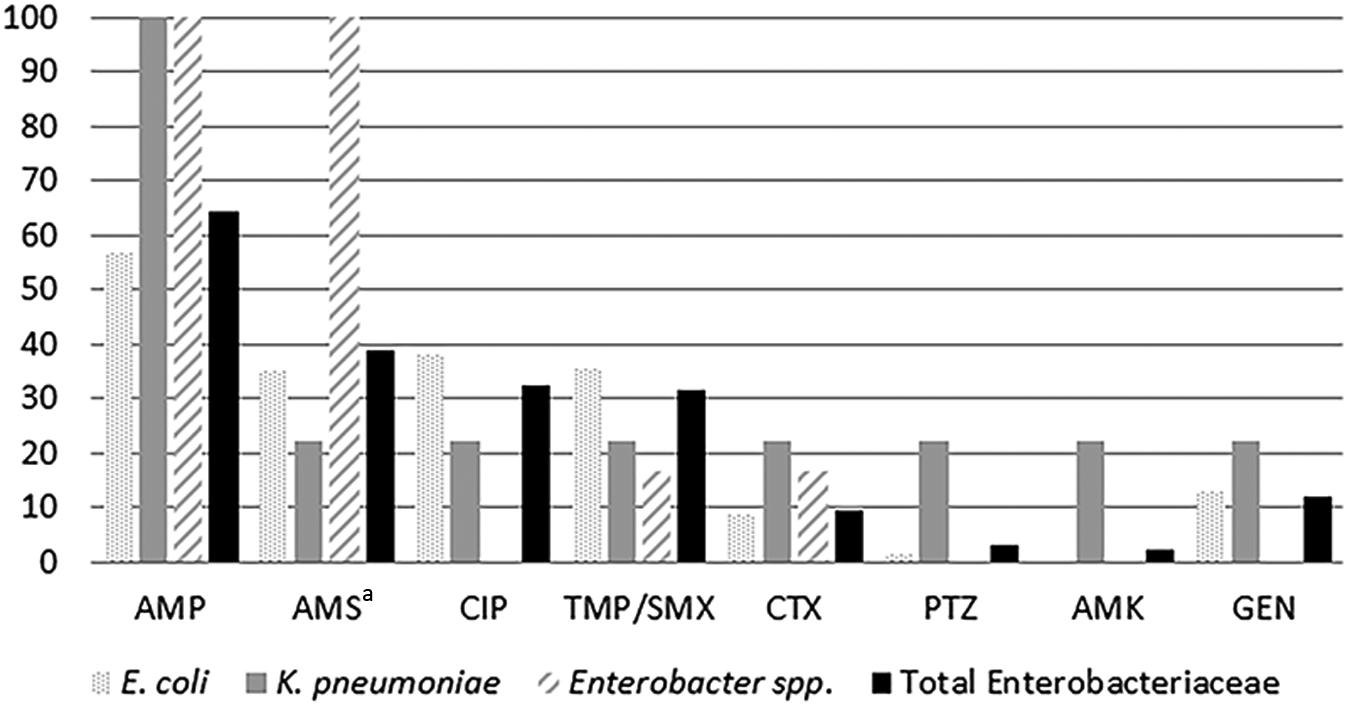
Antibiotic resistance in Enterobacteriaceae from intra-abdominal infections (in percentage). AMP = ampicillin; AMS = ampicillin/sulbactam; CIP = ciprofloxacin; TMP/SMX = trimethoprim/sulfamethoxazole; CTX = cefotaxime; PTZ = piperacillin/tazobactam; AMK = amikacin; GEN = gentamicin.
Figure 2 shows the antimicrobial resistance in Enterobacteriaceae isolated from cIAI and uIAI. Resistance was higher for patients with cIAI; however, it was statistically significant only for ampicillin (73 versus 53%; relative risk [RR] 1.4; CI 0.9–1.9; p = 0.04). Considering the global resistance (both natural and acquired) against the most prescribed EAT (AMS plus CIP), 20 patients had at least one isolate not susceptible to both antibiotics (16.8%; CI 10.6–24.7%). The theoretical activity of different regimens is shown in Fig. 3. Resistance to AMS plus CIP was higher in cIAI than in uIAI, 20.9 versus 11.5%, although the difference did not reach statistical significance (OR 2.0; CI 0.7–5.4; p = 0.17).

Antibiotic resistance in Enterobacteriaceae from intra-abdominal infections (in percentage). Complicated IAI was defined by surgical findings of peritonitis. AMP = ampicillin; AMS = ampicillin/sulbactam; CIP = ciprofloxacin; TMP/SMX = trimethoprim/sulfamethoxazole; CTX = cefotaxime; PTZ = piperacillin/tazobactam; AMK = amikacin; GEN = gentamicin.
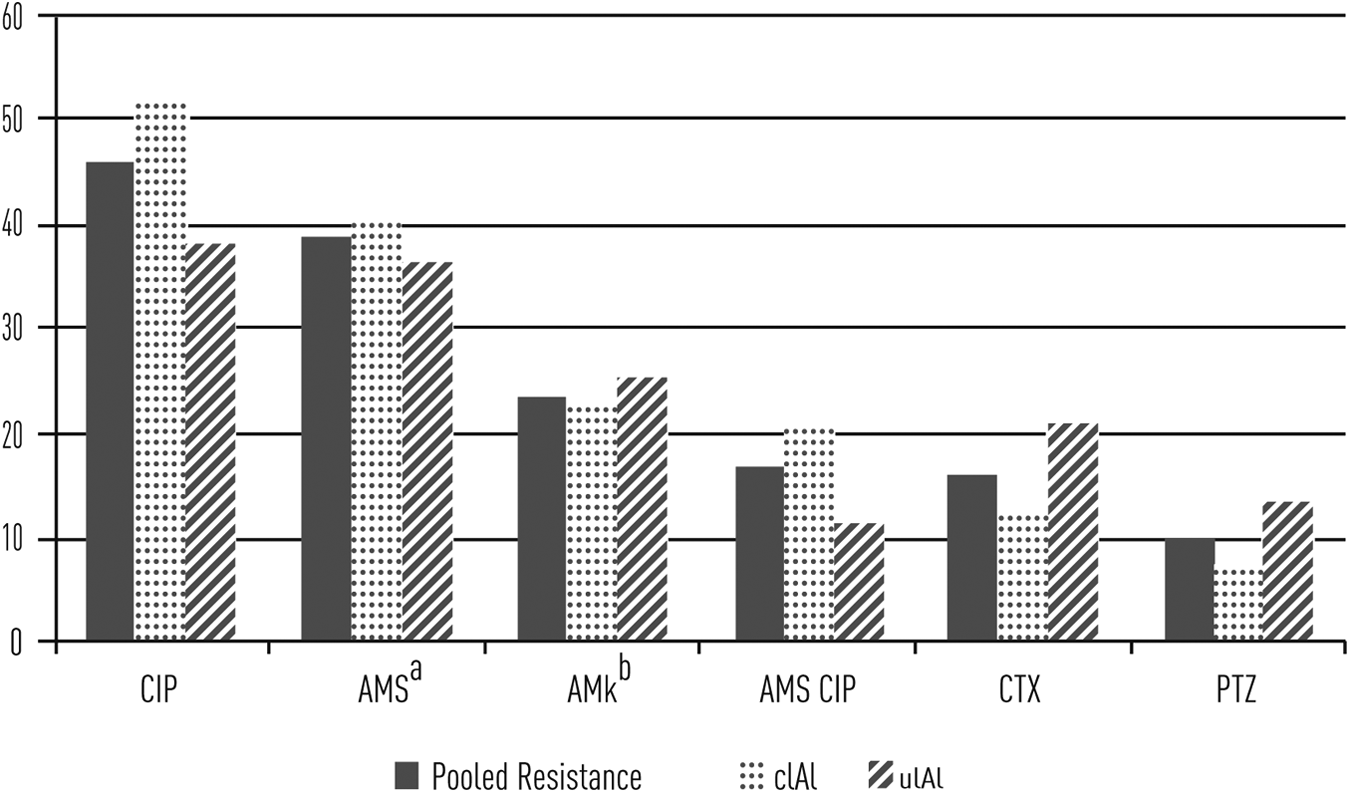
Theoretical resistance to different antibiotic regimens in aerobic isolate(s) from each patient (in percentage). To consider the regimen active, it must show in vitro activity against all microorganisms isolated. cIAI = complicated IAI; uIAI = uncomplicated IAI; CIP = ciprofloxacin; AMS = ampicillin/sulbactam; AMK = amikacin; CTX = cefotaxime; PTZ = piperacillin/tazobactam.
Factors associated with resistance
Patient characteristics associated with isolates resistant to AMS plus CIP are shown in Table 3. In the univariable analysis, diabetes mellitus was associated with resistance to AMS plus CIP, as was female gender, although this did not reach statistical significance (p = 0.10). In the multivariable analysis, the presence of diabetes mellitus remained associated with resistance to AMS plus CIP, whereas female gender was associated but with no statistical significance (p = 0.08).
Characteristics Associated with Resistance to Standard Antibiotic Therapy
cIAI = complicated intra-abdominal infection; CI = confidence interval; uIAI = uncomplicated intra-abdominal infection.
Discussion
In this study of CA IAIs, we found high rates of resistance to first-line antibiotics often prescribed in this scenario. Resistance of Enterobacteriaceae to AMS, CIP, and TMP/SMX was seen in more than 30% of isolates. These results are in line with previous reports in our country, as well as in other regions of the world [3,11–14]. Resistance to third-generation cephalosporins (3GCs) was considerable, 9.7%, which may show the increasing prevalence of extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae in CA infections, as shown in the SMART study, even though they considered CA IAIs based only on the time after admission, without taking into account other factors such as previous admissions [15,16].
In the present work, we took a pragmatic approach and sought to assess the efficacy of the EAT recommended at our institution instead of analyzing the resistance of the different isolates alone, given that the activity of an antimicrobial treatment depends on both the species involved (natural resistance) and any acquired resistance. The recommended EAT, AMS plus CIP, was prescribed for almost half of the patients, and 16.8% of the patients had at least one isolate resistant to both antibiotics. The proportion of resistance to AMS or CIP was unacceptably high to use only one active antibiotic against aerobic bacteria. Moreover, VGS were the second isolates in frequency behind E. coli, and CIP is not an adequate choice for these organisms [17]. Therefore, we use combination therapy against aerobic bacteria from IAIs. Even though AMS plus CIP does not provide coverage for a small but significant proportion of aerobic bacteria in our population, patients with mild presentation and uncomplicated IAI might evolve favorably with surgical source control alone [4,7,8]. However, patients presenting with sepsis or complicated IAI could have worse outcomes with inappropriate initial antibiotic therapy [18,19]. We observed that resistance to AMS plus CIP was higher in cIAI without statistical significance with this sample size, so this should be studied in larger samples.
Recently, concern has been raised about the use of quinolones because of their potentially serious adverse effects, as well as the possibility of selection of ESBL-producing Enterobacteriaceae and Clostridium difficile [20–25]. Aminoglycosides combined with an anti-anaerobic agent could be an option for patients with uncomplicated IAIs. In our study, the resistance to amikacin among Enterobacteriaceae was low, 2.1%, but considering all isolates and given the natural resistance of VGS and Enterococcus spp. to this antibiotic, the overall activity of amikacin was lower than the activity for AMS plus CIP. Moreover, toxicity and higher failure rates than other regimens, as has been shown in one meta-analysis, make aminoglycosides not a proper option for complicated IAIs [4,7,26]. The 3GCs combined with an anti-anaerobic agent are recommended in mild to moderate IAI in a number of guidelines as an option for empirical treatment [4,7,8,27]. In our cohort, the rate of resistance to cefotaxime in Enterobacteriaceae was 9.7%. However, 3GCs have no activity against Enterococcus spp., and cefotaxime or ceftriaxone do not act against Pseudomonas spp., which explains partially the similar proportion of resistance to AMS plus CIP when all patients are considered [28]. Furthermore, 3GCs have been associated with selection of ESBL-producing Enterobacteriaceae and in one meta-analysis of observational studies were found to have the strongest association with C. difficile infection [29–31].
Pipericillin/tazobactam exhibited the lowest proportion of resistance among the regimens studied, with only 12 of 119 patients yielding an isolate not covered by it. Resistance to PTZ was mainly the natural resistance of the microorganisms involved (two E. faecium, two Candida spp., one methicillin-resistant S. aureus, and four Aeromonas spp. against which it was not tested). Only three isolates exhibited acquired resistance to PTZ, two of which were not susceptible to 3GCs. Considering that there were nine Enterobacteriaceae resistant to 3GCs, it could be argued that ESBL-producing GNB were predominantly susceptible to PTZ. Use of PTZ for infections with susceptible ESBL-producing Enterobacteriaceae is a matter of debate. Two recent meta-analyses of observational trials including 2,200 and 3,800 patients showed no difference in the mortality rate for both empiric and definitive therapy with PTZ compared with carbapenems for treatment of ESBL-producing Enterobacteriaceae blood stream infections [32,33]. On the other hand, a recent randomized trial found a lower mortality rate with meropenem than with PTZ for E. coli or K. pneumoniae blood stream infections and ceftriaxone resistance [34]. The results were consistent among different subgroups and accounted only for definitive therapy. However, the study was not blinded and had a noninferiority margin of 5%, lower than the usual 10%. Nevertheless, these studies were designed for blood stream infections. The meta-analysis made by Sfeir et al. included data on the sources of the bacteremia, and they concluded that PTZ may be considered as an option for ESBL-producing Enterobacteriaceae blood stream infections, especially when the source is genitourinary or abdominal [33]. More trials are needed to clarify this situation.
Carbapenems are recommended for CA IAI in some guidelines, especially in settings with high resistance to first-line antimicrobial drugs [7,8]. However, precaution is warranted on its use, given the wide spread of carbapenem-resistant Enterobacteriaceae (CRE) [8]. In our country, KPC-producing K. pneumoniae accounts for as many as 20% of K. pneumoniae isolates [35]. Because carbapenem use is linked to selection of CRE, sparing these antibiotics is a cornerstone of preventing CRE emergence in our setting [36,37]. Moreover, in line with our findings, ESBL-producing GNB rates are low in CA IAI, so other options could be used in this situation.
Little is known about the risk factors for resistance in CA IAIs. For patients with risk factors for ESBL infections, guidelines recommend considering antibiotics active against these microorganisms [4,7,8]. These risk factors include recent exposure to antibiotics, colonization with ESBL-producing Enterobacteriaceae, and travel to a region of high endemicity for ESBL-producing microorganisms. In a multinational survey, the risk factors for ESBL infections in non-hospitalized patients without recent healthcare contact were male sex, recent use of a cephalosporin, and age more than 65 years [38]. However, these factors were not specific for IAIs, and most of the infections were urinary. In this work, we did not look for risk factors for ESBL specifically; we intended to find risk factors for resistance, acquired or natural, to the EAT used at our institution. In both univariable and multivariable analyses, we found that diabetes mellitus was associated with an isolate from CA IAIs that was resistant to both antibiotics. Female sex showed a tendency toward resistance, but the difference did not reach statistical significance. Given the pragmatic approach, it is hard to find studies addressing this particular endpoint. Recently, it has been suggested to categorized certain patients with IAI as having healthcare-acquired IAI when certain criteria are met: Hospitalization for longer than 48 hours or within the previous 90 days; residence in a long-term care facility within the previous 30 days; home infusion therapy, wound care or dialysis within the preceding 30 days, and use of broad-spectrum antibiotics during the last 90 days [7]. However, those authors acknowledge that those factors are not specific for IAI. Therefore, we believe our findings should be taken into account when prescribing an empirical antibiotic for IAIs in our setting. Diabetic women had around a nine-fold greater chance of having an organism resistant to AMS plus CIP than did non-diabetic men. In other studies, diabetes mellitus has not been associated consistently with pathogens resistant to first-line antibiotics, including in urinary tract and extra-intestinal E. coli infections [39–41]. It could be hypothesized that diabetic patients are more prone to exposure to antibiotics or healthcare contact and that could explain our results; we did not address prior antibiotic exposure.
This study has limitations. First of all, it was retrospective, with data collected from medical records; hence, we could not address certain factors such as prior antibiotic exposure or admissions to other facilities, although most of our population belongs to a closed healthcare system. Second, we found low rates of polymicrobial cultures compared with other series. For the inclusion of patients, they had to have at least one positive aerobic culture from IAI; polymicrobial cultures in which no predominant pathogen could be identified were excluded. This could affect the results and external validity. Third, it was a single-center study, and even though the results are in line with previous work, they might not be extrapolated to other settings and geographic regions. Finally, although we tried to control for confounders using logistic regression, the results of the association of diabetes mellitus with resistant pathogens could still be confounded by factors not included in the study.
In conclusion, our data show high resistance rates to first-line antibiotics in isolates from CA IAIs. Nevertheless, AMS plus CIP appears to be a good option for patients with mild to moderate infections. For diabetic patients and patients with severe infections, PTZ should be considered. Larger multicenter studies are needed to confirm these findings and control possible confounders.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
This work was presented as an abstract at the 18th International Congress on Infectious Disease and XVIII Congress of the Sociedad Argentina de Infectología on March 1-4, 2018.