
Abstract
Abstract
Background:
Recently, the possible use of laboratory parameters such as full blood count, neutrophil count, neutrophil to lymphocyte ratio (NLR), thrombocyte count (PLT), and mean thrombocyte volume (MPV) have been investigated in diagnosis of acute appendicitis and the prediction of complications. The aim of this study was to investigate the utility of the platelet to lymphocyte ratio (PLR) value as a biomedical marker in the prediction of acute appendicitis and perforated appendix.
Patients and Methods:
The data were retrieved from the hospital records related to age, gender, length of stay in hospital, MPV, leukocyte, neutrophil, lymphocyte, and thrombocyte counts measured in the peripheral venous blood sample on presentation, NLR and PLR values, and the pathology results. The patients were grouped according to the pathology results as follows: group 1 (normal appendix, n = 86); group 2 (acute appendicitis, n = 458); group 3 (perforated appendicitis, n = 14).
Results:
The study included a total of 558 patients (308 males; 250 females) with a mean age of 34.24 ± 14.27 years. The mean length of stay in hospital was 2.12 days. The leukocyte and neutrophil count values of group 1 were lower than group 2 and group 3 values (p < 0.001). The lymphocyte count values of group 1 were higher than those of the other groups (p < 0.001). The NLR and PLR values of group 1 were lower than group 2 and group 3 values (p < 0.001). The length of stay in hospital was shorter in group 1 than in group 2 and group 3 (p = 0.42). The receiver operating characteristic (ROC) curve test results showed that PLR and NLR values were sensitive and specific to differentiate normal appendix, acute appendicitis, and perforated appendicitis.
Conclusion:
The results of this study demonstrated that PLR value, such as NLR, could be evaluated as a new biomarker that could be valuable in the differentiation of normal appendix from acute appendicitis and in the differentiation of acute appendicitis from perforated appendicitis.
Acute appendicitis is the most common cause of acute abdomen. It has been reported in the literature that there is a lifetime incidence of this disease of approximately 7% and a perforation rate of 17%–20% [1,2]. Although the mortality risk is less than 1% in the general population, this rate can increase to 50% in elderly patients [3,4]. Although some clinical findings of acute appendicitis such as elevated leukocyte count and pain in the right lower quadrant are well known, these findings may not be determinant. Several laboratory parameters have been used to date to diagnose the disease and determine the clinical severity of acute appendicitis.
Current radiologic examination methods, especially ultrasonography and computed tomography (CT) are widely and successfully used in the diagnosis of acute appendicitis and complications [5–8]. However, because these diagnostic methods require special equipment and experienced radiologists, surgeons are still searching for simpler diagnostic tools [5–7]. In recent clinical studies, there has been research into the possible use of laboratory parameters such as full blood count, neutrophil count, neutrophil to lymphocyte ratio (NLR), thrombocyte count (PLT), and mean thrombocyte volume (MPV) in the diagnosis of acute appendicitis and the prediction of complications. However, to the best of our knowledge there has been no previous study that has examined the capability of PLR in the diagnosis of acute appendicitis and the prediction of complications. The aim of this retrospective clinical study was to investigate the utility of the PLR value as a biomedical marker in the prediction of acute appendicitis and perforated appendicitis.
Patients and Methods
Patient groups
Approval for the study was granted by the Clinical Research Local Ethics Committee (decision no: 12/07, dated: May 16, 2017). A retrospective examination was made of the clinical and laboratory data of patients who underwent surgery in the general surgery clinic for initial diagnosis of acute appendicitis between 2013 and 2017. Patients were excluded if the information was not available, if they were aged younger than 18 years, had any surgery additional to appendectomy, or if they had an appendix tumor. The patients were grouped according to the pathology results as follows: group 1, normal appendix (n = 86); group 2, acute appendicitis (n = 458); and group 3, perforated appendicitis (n = 14).
Methods
The data that were retrieved from the hospital records of the patients who had undergone surgery because of the initial diagnosis of acute appendicitis comprised the age (years), gender, length of stay in hospital (days), and histopathologic examination results. Additionally, on first admission, the MPV, leukocyte, neutrophil, lymphocyte, and thrombocyte count values, and NLR and PLR values measured at venous blood sample were recorded.
Surgical procedure
Open appendectomy comprising intra-abdominal access via a McBurney incision and a muscle-split peritoneal incision was performed to all patients. After ligation of the mesoappendix with suture, the stump of the appendix was divided with absorbable sutures, without the use of a purse-string suture and cut and the appendix was then removed. At the end of the operation, the surgical area was washed using saline solution and closed anatomically after placement of the drainage catheter. All collected specimens were examined histopathologically.
Biochemical analysis
Routine biochemical parameters were examined in venous blood samples taken on admittance and sent to the biochemical laboratory. The thrombocyte (reference range, 150,000–450,000 per microliter), MPV (reference range, 0.00–15.00 fL), leukocyte (reference range, 4,400–11,300 per microliter), neutrophil (reference range, 1,100–9,600 per microliter), and lymphocyte (reference range, 500-6,000 per microliter) counts were determined using an automatic analyzer (Mindray BC-6800, Shenzen, China).
Statistical analysis
Non-parametric data were analyzed using the Kruskal-Wallis test (p < 0.05). The Mann-Whitney U test was applied for the binary comparisons of the groups (p < 0.05). The receiver operating characteristic (ROC) curve test was performed to determine the predictive properties of the parameters of the disease and the sensitivity-specificity ratios were determined by setting cutoff values. Spearman ρ correlation test was used to determine the correlation between disease parameters (p < 0.05).
Results
The study included a total of 558 patients, including 308 (55.2%) males and 250 (44.8%) females with a mean age of 34.24 ± 14.27 years. The mean length of stay in hospital was 2.12 days. The histopathologic results of the patients treated with appendectomy were normal appendix in 86 (15.4%; group 1), acute appendicitis in 458 (82.1%; group 2), and perforated appendicitis in 14 (2.5%; group 3).
No statistically significant difference was determined between the groups in terms of age, PLT count, and MPV. The neutrophil count (p < 0.001), lymphocyte count (p < 0.001), leukocyte count (p < 0.001), NLR (p < 0.001), PLR (p < 0.001), length of stay in hospital (p = 0.045), and gender (p = 0.004) were statistically different among the groups (Table 1). In binary comparisons of the groups, the male gender ratio in group 1 (40.7%) was lower than in group 2 (57.2%; p = 0.005). The neutrophil count (p < 0.001), leukocyte count (p < 0.001) NLR value (p < 0.001), PLR value (p < 0.001), and length of stay in hospital (p = 0.042) in group 1 were found to be lower than in group 2. However, lymphocyte count in group 1 was higher than in group 2 (p < 0.001) (Table 2). The ratio of male gender was found to be lower in group 1 (40.7%) than in group 3 (78.6%; p = 0.009). The neutrophil count (p < 0.001), leukocyte count (p < 0.001), NLR value (p < 0.001), and PLR value (p < 0.001) in group 1 were lower than in group 3. The lymphocyte count in group 1 was higher than in group 3 (p = 0.004; Table 2). The values of neutrophil count (p = 0.003), leukocyte count (p = 0.004), NLR value (p = 0.012), and PLR value (p = 0.041) in group 2 were lower than in group 3 (Table 2; Fig. 1).
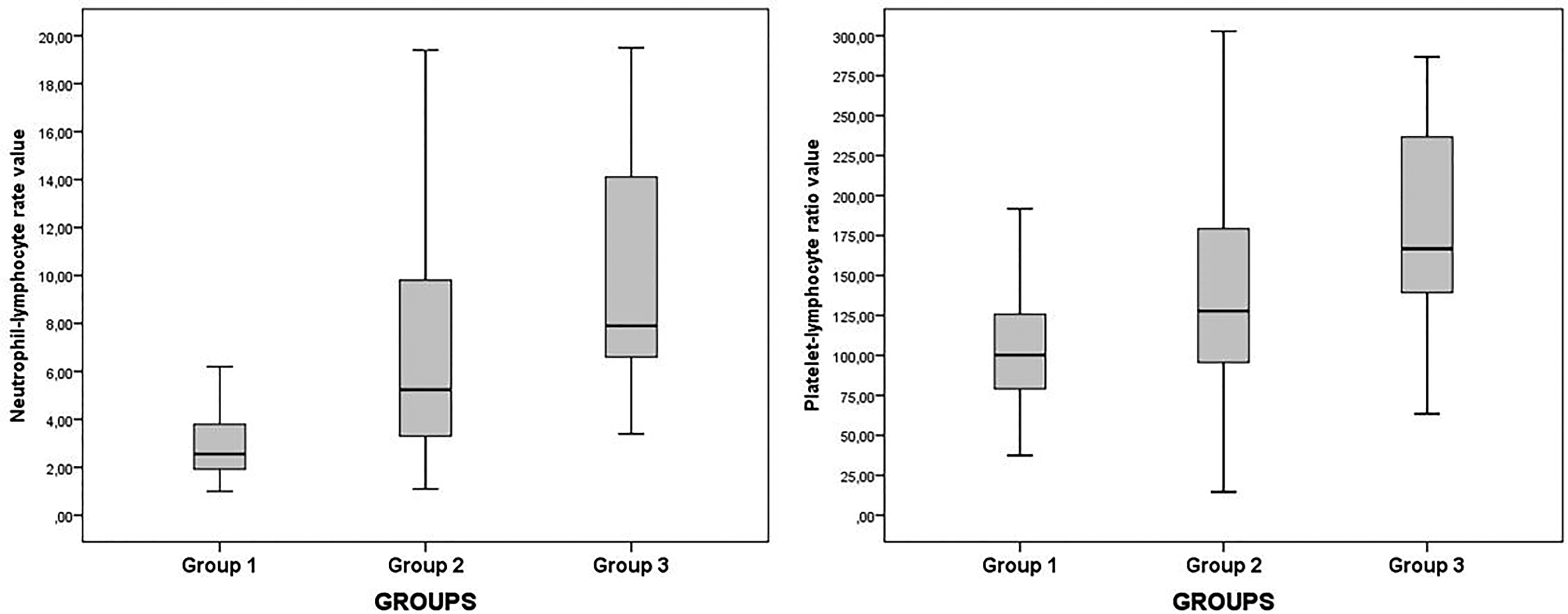
Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) values of each group.
Differences İn Neutrophil, Lymphocyte, and Leukocyte Counts, Neutrophil to Lymphocyte and Platelet to Lymphocate Ratios, Duration of Hospital Stay, and Gender
Kruskal-Wallis test, p < 0.
Min = minimum; Max = maximum; SD = standard deviation.
The Post Hoc Test Results of the Parameters of the Groups
Mann-Whitney U test, p < 0.05
Receiver operating characteristic curve analysis
When the PLR value was greater than 107.43, sensitivity was determined as 64.4% and specificity as 61.5% in the differentiation of acute appendicitis from normal appendix (area under the curve [AUC] = 0.673, p < 0.001). When the PLR value was greater than 140.45, sensitivity was determined as 71.4% and specificity 88.9% in the differentiation of perforated appendicitis from normal appendix (AUC = 0.819, p < 0.001). When the PLR value was greater than 163.27, sensitivity was determined as 64.3% and specificity as 67.5% in the differentiation of perforated appendicitis from acute appendicitis (AUC = 0.660, p = 0.041; Table 3; Fig. 2).
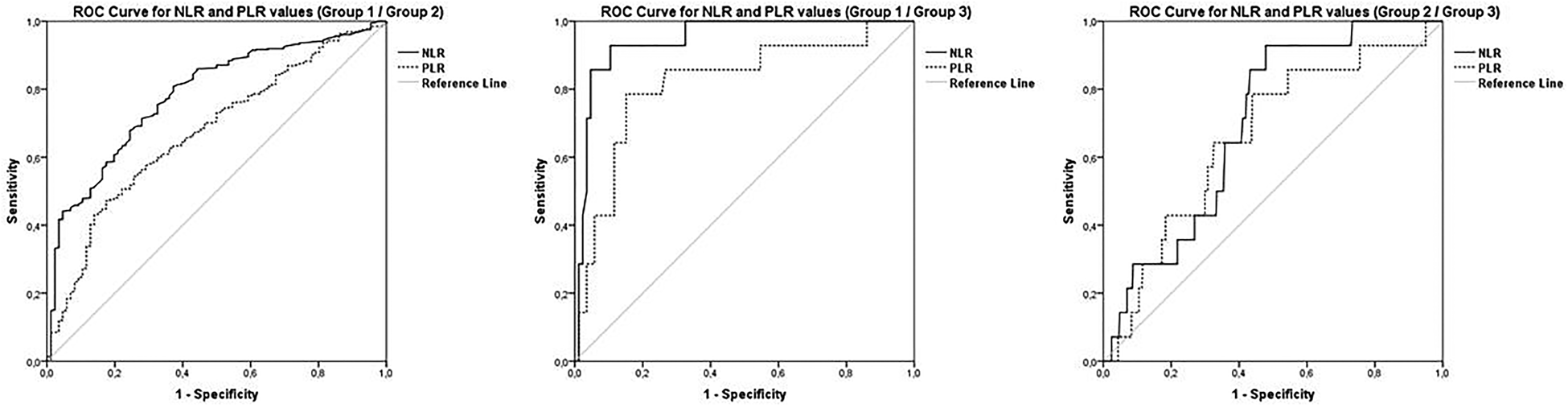
The receiver operating characteristic (ROC) curve analysis results of the neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR).
The Results of the Receiver Operating Characteristic Curve Analysis of the Neutrophil to Lymphocyte ratio and Platelet to Llymphocyte Ratio Values
Receiver operating characteristic (ROC) curve test, p < 0.05.
NLR = neutrophil to lymphocyte ratio; PLR = platelet to lymphocyte ratio.
When the NLR value was greater than 3.53, sensitivity was determined as 71.4% and specificity as 72.1% in the differentiation of acute appendicitis from normal appendix (AUC = 0.784, p < 0.001). When the NLR was greater than 6.08, sensitivity was determined as 85.7% and specificity as 93.0% in the differentiation of perforated appendicitis from normal appendix (AUC = 0.946, p < 0.001). When the NLR value was taken as 7.65, sensitivity was determined as 64.3% and specificity as 64.2% in the differentiation of perforated appendicitis from acute appendicitis (AUC = 0.698, p = 0.012; Table 3; Fig. 2).
Correlation analysis
The histopapathologic examination results (1 = normal, 2 = acute appendicitis, 3 = perforated appendicitis) were positively correlated with male gender (r = 0.141, p < 0.001), neutrophil count (r = 0.343, p < 0.001), leukocyte count (r = 0.307, p < 0.001), NLR (r = 0.292, p < 0.001), PLR (r = 0.199, p < 0.001) and length of stay in hospital (r = 0.128, p = 0.002), and negatively correlated with the lymphocyte count (r = −0.171, p < 0.001).
Discussion
As a result of technological advances in radiologic examination methods and other diagnostic methods, a successful diagnosis can be more easily made in most patients, but serious problems may still be experienced in the ability to diagnose some patients and in the prediction of unwanted complications such as perforation and peritonitis [1,5,6,9,10]. When this is taken into consideration, there is an increasing need for research into simple and inexpensive biochemical laboratory parameters that could be helpful in the diagnosis of acute appendicitis [6].
Twenty years ago Goodman et al. [11] reported that the NLR value could be a more sensitive parameter than leukocyte count. It is accepted that an increase in the difference between neutrophil and lymphocyte counts could reflect the severity of inflammatory response as they are known to be components of the cellular response in the systemic inflammation of neutrocytosis and lymphocytopenia. Based on this, the NLR has been used as a biomarker for several pathologic events such as primarily malignancies, chronic inflammatory diseases, and post-operative complications [5,12–16]. Neutrophil to lymphocyte ratio values have also been used to diagnose acute appendicitis and to predict appendix perforation [1,5,17,18]. In the current study, a 3.35 cutoff value of the NLR was found to have 71.4% sensitivity and 72.1% specificity in the differentiation of acute appendicitis from normal appendix and a 7.65 cutoff value of NLR could be predictive in the differentiation of perforated appendicitis from acute appendicitis with sensitivity of 64.3% and specificity of 64.2%.
Despite the similarities and inconsistencies, it was determined as a result of this study that the NLR value could be a significant parameter in the diagnosis of acute appendicitis and in the differentiation of patients with perforated appendicitis. In this study, the lymphocyte count was found to be lower in the acute appendicitis and perforated appendicitis patients compared with patients with a normal appendix. Although the lymphocyte count was found to be lower in patients with perforated appendicitis compared with patients with acute appendicitis, the difference was not statistically significant. However, in other studies, it has been reported that the lymphocyte count could be decreased in acute appendicitis and this decrease could be even greater in complicated appendicitis [19–22]. Consequently, it was believed that the high cutoff values of the NLR and PLR obtained in the current study could be explained by these findings. Moreover, it was also believed that the high NLR values obtained in patients with complicated appendicitis could be explained by the greater increase in neutrophil count compared to leukocyte count at the onset of the acute phase in inflammation. An increase in leukocyte count is an early test showing sensitivity of 82%–96% in appendix inflammation [23–25]. Previous studies have found a relation between the increases in neutrophil and leukocyte counts and the severity of acute appendicitis [23,26]. The sensitivity of neutrophil count in acute appendicitis has been shown to be 60%–87% in previous studies [23,27].
In the current study, a difference was seen between the groups regarding leukocyte and neutrophil counts. Furthermore, correlation analysis results demonstrated that neutrophil count, leucocyte count, NLR, and PLR values may increase substantially in patients with perforated appendicitis than patients with acute appendicitis; duration of length of stay in hospital may be prolonged in these patients.
Although it has been reported in the literature that thrombocyte count is a marker of the severity of systemic infection [5,15], there are also some studies that have stated that thrombocyte count is not a helpful marker in the comparison of perforated appendicitis with simple appendicitis [5,28,29]. In addition, although there have been several studies examining the relation between acute appendicitis and NLR values, to the best of our knowledge, except for a few studies with a limited number of patients and pregnant patients related to use of PLR values, there has been no extensive, comprehensive study [30,31]. In a study by Yazar et al. [31] including 28 pregnant patients diagnosed with acute appendicitis, it was reported that a diagnosis of acute appendicitis could be made accurately at the rate of 90.5% when the NLR and PLR values were used in combination with leukocyte count, C-reactive protein level, and lymphocyte count. Cinar et al. [30] conducted a study of 47 pregnant patients diagnosed with acute appendicitis and reported that the NLR and PLR values were a sensitive and specific test for the diagnosis of acute appendicitis.
In the current study, thrombocyte count was not seen to be successful either in the diagnosis of acute appendicitis or in the differentiation of perforated appendicitis. In fact, the platelet count results did not differ between the study groups, however, it was seen that compared with the patients with a normal appendix, lymphocyte count results decreased in patients with acute appendicitis and in patients with perforated appendicitis. Moreover, these lymphocyte count results were much more decreased in patients with perforated appendicitis. On the other hand, PLR values were different among the groups and it was found that compared with the patients with a normal appendix, these values increased much more in patients with acute appendicitis and perforated appendicitis. Therefore, it could be hypothesized with these findings that that increased PLR values could be related with low lymphocyte count values; and correlation analysis results also supported this hypothesis. Moreover, ROC curve analysis results demonstrated that a PLR cutoff value of 107.43 was found to be predictive in the differentiation of acute appendicitis from normal appendix with sensitivity of 64.4% and specificity of 61.5% and a cutoff value of 163.27 had 64.3% sensitivity and 67.5% specificity in the differentiation of perforated appendicitis from acute appendicitis. Based on these findings, it can be strongly suggested that PLR value could be a new biomarker that could be of diagnostic value in patients with acute appendicitis and perforated appendicitis and it could be of and predictive value in differentiation of acute appendicitis from perforated appendicitis.
There are studies with different results about the relation between active inflammatory processes and MPV. Kim et al. [32] stated that an increase in the MPV value could be an independent risk factor for mortality in patients with sepsis. In contrast, a decrease in the MPV value has been reported to be related to the activation of rheumatoid diseases such as systemic lupus erythematosis, ankylosing spondylitis, and especially rheumatoid arthritis [33]. In studies that have considered the relation between acute appendicitis and MPV, conflicting results have been reported [28,29,34–37]. In the current study, no difference was found between the groups in respect of the MPV value, and therefore it was considered that MPV may not be a useful parameter for clinical application.
In a study by Kahramanca et al. [1], the female to male ratio was reported to be higher in the negative appendectomy group. In the current study, female patients were also determined at a statistically higher rate in the negative appendectomy group, which was believed to be caused by gynecologic diseases mimicking the clinical findings of acute appendicitis.
Conclusion
The results of this study demonstrated that PLR values, such as NLR, could be evaluated as a new biomarker that could be valuable in the differentiation of normal appendix from acute appendicitis and in the differentiation of acute appendicitis from perforated appendicitis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.