
Abstract
Background:
Our study sought to describe the incidence of culture-confirmed postsurgical Staphylococcus aureus infection after elective hysterectomy and evaluate patient characteristics, risk factors, and economic consequences associated with Staphylococcus aureus infection.
Methods:
This was a retrospective cohort study of patients in the United States (≥18 years old; Kaiser Permanente health plan members) who underwent elective hysterectomy from 2007 to 2013. Hysterectomies were categorized by surgical setting (inpatient vs. outpatient) and procedure (abdominal, laparoscopic, or vaginal). We estimated the cumulative incidence of culture-confirmed Staphylococcus aureus infection (90 days post-surgery) and compared healthcare resource utilization and costs (within 120 days post-surgery) among patients with/without Staphylococcus aureus infection or with other infection.
Results:
Among 30,960 patients identified, 20,675 underwent inpatient hysterectomy (abdominal: 47.8%; laparoscopic: 24.8%; vaginal: 27.3%), and 10,285 underwent outpatient hysterectomy (laparoscopic: 86.1%; vaginal: 13.9%). The incidence of culture-confirmed Staphylococcus aureus infection was 0.8% and 0.4% for inpatient (abdominal: 1.2%; laparoscopic: 0.5%; vaginal: 0.2%) and outpatient (laparoscopic: 0.5%; vaginal: 0.1%) surgery, respectively. Patients with Staphylococcus aureus infection had more emergency department visits, hospitalizations, and re-operations compared with patients without infection or with non-Staphylococcus aureus infection. Mean total costs for patients with Staphylococcus aureus infection were higher (inpatient: $18,261; outpatient: $4,422) compared with patients without infection (inpatient: $6,171; p < 0.0001; outpatient: $905; p = 0.0023) or non-Staphylococcus aureus infection (inpatient: $11,207; p = 0.0117; outpatient: $3,005; p = 0.2117).
Conclusions:
Culture-confirmed postsurgical Staphylococcus aureus infection incidence was predominately associated with procedure type rather than surgical setting. Patients with post-surgical Staphylococcus aureus infection had higher health care utilization and costs than those without infection or with other infection types. Additional effective infection control strategies are needed to reduce the morbidity and costs associated with Staphylococcus aureus infection.
Hysterectomy is the most common elective major operation for women in the United States, with approximately 600,000 hysterectomies performed annually in the inpatient setting, resulting in 6,000–24,000 surgical site infections (SSIs) each year [1–3]. Infection is the leading post-surgical complication for these procedures [4], affecting 10.5% of abdominal, 13.0% of vaginal, and 9.0% of laparoscopic [4,5] surgeries.
Surgical site infections are associated with increased length of hospital stay and post-surgery costs [6,7], and are the most common reason for re-admission after hysterectomies. The recently implemented Hospital-Acquired Condition Reduction Program by Centers for Medicare & Medicaid incentivizes hospitals to reduce health-care–acquired infection by tying payments with performance on indicators such as rate of SSIs after abdominal hysterectomy [8]. Staphylococcus aureus is a frequent cause of post-surgical infection after hysterectomy [4].
Although prior studies have estimated the rate of SSIs after hysterectomy, none have specifically examined SSIs and other non-surgical site infections caused by Staphylococcus aureus, despite the large hospital- and community-based burden of Staphylococcus aureus disease [9–12]. Prior studies lacked the longitudinal follow-up required to capture infections after surgery discharge in outpatient settings [10,13,14]. Additionally, more hysterectomies are being performed in outpatient settings, including hospital-based ambulatory units [15–19], and limited data are available on outpatient postsurgical infections, compared with inpatient surgeries.
Our objective was to estimate the incidence rates of culture-confirmed Staphylococcus aureus infection after hysterectomy surgery, evaluate patient characteristics and risk factors associated with developing Staphylococcus aureus infection, and assess healthcare resource utilization (HCRU) and costs associated with Staphylococcus aureus infection among women who underwent elective hysterectomy in the inpatient and outpatient setting of an integrated healthcare system.
Patients and Methods
Study setting and data source
The research database was from Kaiser Permanente Southern California (KPSC), a non-profit, integrated health services delivery system with approximately four million health plan members. Kaiser Permanente Southern California provides comprehensive medical services through its own facilities, including approximately 14 hospitals and 200 outpatient clinics. As such, the likelihood of patients needing to obtain medical care outside of a KPSC facility (e.g., when traveling interstate) would be low. All patient data for this study were de-identified. The study was approved by the KPSC Institutional Review Board.
Study population
We conducted a retrospective database cohort study using the KPSC database for the seven-year study period: January 1, 2007 through December 31, 2013. Cohort members had an elective hysterectomy during the study period. Hysterectomies were categorized as inpatient or outpatient surgeries, and further stratified as abdominal, laparoscopic, or vaginal procedures, based on International Classification of Disease, 9th revision, Clinical Modification (ICD-9-CM) or Current Procedural Terminology Coding System, 4th edition (CPT-4) procedure codes.
All patients had continuous medical membership with drug benefit eligibility 12 months before surgery date. Enrollment gaps ≤30 days were considered continuous membership eligibility. Patients were required to be ≥18 years of age on the surgery date.
Elective inpatient hysterectomy was defined by the following criteria: hysterectomy performed during an inpatient hospitalization with at least an overnight stay (Centers for Disease Control National Healthcare Safety Network [CDC NHSN]), admission not started in an emergency department (ED), admission type indicated as “elective,” patient not transferred from another acute-care hospital, and surgery performed within two days of hospital admission [13]. Elective outpatient hysterectomy was defined using the following criteria: hysterectomy conducted in an outpatient ambulatory center or a hospital-based unit where dates of admission and discharge were the same (CDC NHSN) and patient not admitted from the ED.
Staphylococcus aureus infection was defined as any Staphylococcus aureus growth from clinical microbiologic culture (i.e., any source except nasal, groin, and “surveillance”) collected two days or more post-surgery (based on date of culture collection). To remove patients with pre-existing Staphylococcus aureus infection, we excluded those with positive Staphylococcus aureus cultures within 12 months before surgery, on surgery date, or day after surgery. Patients who started as outpatients and were converted to inpatients as a result of procedural complications were classified as inpatients in this study.
Descriptive variables
Baseline characteristics included age, race, comorbid conditions, Charlson comorbidity index (CCI), and risk factors such as anemia, asplenia, blood transfusion, malnutrition, peripheral vascular disease, transient ischemic attack, and body mass index (BMI). Body mass index measurements were obtained most proximate to the surgery date (within 12 months before) and categorized using U.S. Centers for Disease Control and Prevention and World Health Organization international classifications [20,21]. Patients were followed from surgery date until one of the following end points: Staphylococcus aureus infection, other surgery, death, disenrollment from health plan, end of 90-day follow-up period, or end of study (December 31, 2014), whichever came first.
Outcomes of interest
The primary outcome was the cumulative incidence rate of Staphylococcus aureus infection within 90 days of elective hysterectomy, as well as at hospital discharge, and 30, 60, and 90 days post-surgery. Staphylococcus aureus infection was reported by clinical setting (inpatient or outpatient) and procedure type (abdominal, vaginal, or laparoscopic). Staphylococcus aureus infection (including methicillin-resistant Staphylococcus aureus [MRSA]) was defined using clinical culture reports and sources of culture collection (superficial and invasive). Infection onset was determined by culture collection date. Patients with multiple cultures positive for MRSA and methicillin-susceptible Staphylococcus aureus (MSSA) were assigned to the MRSA group. The incidence rate of postsurgical Staphylococcus aureus infection was calculated as the percentage of patients with hysterectomy who had a positive Staphylococcus aureus culture.
Time to infection was defined as the number of days elapsed from day of surgery to day of collection of the first positive Staphylococcus aureus culture. Infections involving a positive culture for an organism other than Staphylococcus aureus (e.g., Acinetobacter species, Enterococcus species, Escherichia coli, etc.) were categorized as other non-Staphylococcus aureus infection. Similarly, patients with negative cultures or no culture data were defined as having no infection. Gram stain results were not included in the categorization of the patients' infection status
To assess the healthcare system burden of post-surgical Staphylococcus aureus infection and capture treatment costs after Staphylococcus aureus diagnosis within 90 days of the surgery, HCRU and costs were evaluated within 120 days post-surgery for all patients. Healthcare resource utilization included all-cause outpatient, hospital, and ED visits; all-cause hospital length of stay (LOS); and all-cause reoperations. Re-operations were defined using procedure codes from the clinical record during the follow-up period. The calculated total costs did not include the cost of the initial hysterectomy, however, LOS included the initial hospital stay for the hysterectomy. Costs were computed as the sum (US$) paid by the plan and the patient, based upon 2014 KPSC standard fee schedules [22,23]. All comparisons were conducted between patients with Staphylococcus aureus infection versus other infection or without infection.
Statistical analyses
For both inpatient and outpatient hysterectomies, separate analyses were conducted to compare patients with Staphylococcus aureus infection versus patients with other infection and patients without infection. Risk factors associated with Staphylococcus aureus infection were analyzed using χ2 tests for categorical variables and Student t-test for continuous variables. If the frequency was <5, then Fisher exact test was used. To create best-fit models, different analyses were conducted to evaluate each outcome. Multivariable logistic regression was conducted to identify risk factors associated with post-operative Staphylococcus aureus infection for inpatient and outpatient surgeries separately.
For outcomes after hysterectomy, multivariable logistic regression models with a stepwise backward selection were conducted to identify the relation with all-cause hospitalization visits and all-cause reoperation among the three groups. A p value <0.05 was considered significant. Generalized linear models with gamma distributions using log-link functions were conducted to analyze total costs and LOS. All models controlled for potential confounding factors, such as age, CCI score, comorbidities, and other baseline characteristics. All analyses were carried out using SAS software, version 9.3 (SAS Institute, Inc., Cary, NC).
Results
Study population
A total of 30,960 patient surgeries, including 20,675 (67.8%) inpatient and 10,285 (33.2%) outpatient surgeries, were included in the analysis (Table 1). Inpatient surgeries included: 9,890 (47.8%) abdominal, 5,131 (24.8%) laparoscopic, and 5,654 (27.3%) vaginal surgeries. Outpatient surgeries included: 8,852 (86.1%) laparoscopic and 1,433 (13.9%) vaginal surgeries (Table 1).
Identification of the Study Cohort for Inpatient and Outpatient Elective Hysterectomy
Only applicable to inpatient surgeries.
Only applicable to outpatient surgeries.
Patients with a positive Staphyloccus aureus culture from non-MRSA screening tests (blood, urine, wound, respiratory, sputum, etc).
ED = emergency department; MRSA = methicillin-resistant Staphylococcus aureus.
Descriptive baseline characteristics and incidence rate
In all, 205 (0.7%) patients developed Staphylococcus aureus infection ≤90 days after surgery: 160 (0.8%) after inpatient and 45 (0.4%) after outpatient hysterectomy (Fig. 1). Staphylococcus aureus infection incidence rates were highest among patients who underwent an inpatient abdominal hysterectomy (1.2%) and lowest among patients who underwent outpatient vaginal hysterectomy (0.1%; Fig. 1). Incidence rates were similar among the same surgery type despite the clinical setting for laparoscopic (inpatient 0.5% vs. outpatient 0.5%) and vaginal (inpatient 0.2% vs. outpatient 0.1%) surgeries. The proportion of MRSA isolates was higher among inpatient (32.5%) versus outpatient (26.7%) surgeries. The major sources of Staphylococcus aureus infection were wound and incision site for both inpatient and outpatient procedures (Table 2). Of the 205 patients who developed Staphylococcus aureus infection, 100 (48.8%) had less than one source for positive cultures and approximately 10% had Staphylococcus aureus cultured from their blood, indicating a blood stream infection. The median time to Staphylococcus aureus infection was similar among inpatients (abdominal, 23 days [range 4–90]; laparoscopic, 27 days [range 9–87]; vaginal, 38 days [range 14–66]) and outpatients (laparoscopic, 31 days [range 5–80]; vaginal, 41 days [14–68]).

Incidence rates of Staphylococcus aureus infection within 90 days from hysterectomy procedure
Source of Staphylococcus aureus Infection
These are not mutually exclusive. Some patients with positive cultures for Staphyloccus aureus infection had ≥1 source for positive cultures.
Patients with Staphylococcus aureus infection after inpatient hysterectomy were older than those without infection (age 54 vs. 50 years, respectively; p = 0.0061; Table 3). Mean BMI and mean CCI scores, respectively, were higher among inpatients with Staphylococcus aureus infection (36.2 ± 11.2 and 3.2 ± 3.6) than those with other infection (30.5 ± 7.4, and 1.8 ± 2.7; both p < 0.001) or without infection (30.3 ± 6.9, and 1.0 ± 2.0; both p < 0.0001). Patients with Staphylococcus aureus infection had higher frequency of comorbid conditions, such as anemia, chronic pulmonary disease, diabetes, any malignancy, blood transfusions, and hypertension, versus patients without infection or other infection (all p < 0.05; Table 3). Among outpatient surgeries, the proportion of patients with anemia, diabetes, and history of hospitalization was higher in those with Staphylococcus aureus infection compared with patients without infection or with other infection.
Patient Baseline Characteristics by Infection Categories
Note: comorbidities present at <1% of population were not listed individually.
n (%) except where noted.
Indicates statistical significance against S. aureus infection group (α < 0.05).
Indicates statistical significance against S. aureus infection group (α < 0.05) across the whole categorical group.
BMI = body mass index; CCI = Charlson Comorbidity Index; CHF = congestive heart failure; CPD = chronic pulmonary disease; CVD = cerebrovascular disease; MI = myocardial infarction; PVD = peripheral vascular disease; SD = standard deviation.
Risk factors
For both inpatient and outpatient surgeries, multivariable regression models identified anemia, CCI, diabetes, hypertension, malnutrition, obesity, and surgery type (laparoscopic vs. vaginal) as factors significantly associated with Staphylococcus aureus infection (Table 4). Several risk factors were uniquely associated with inpatient (blood transfusion and surgical route) and outpatient (black race, history of prior hospitalization, and drug and substance abuse) surgeries (Table 4). Controlling for other risk factors, laparoscopic route versus vaginal route of hysterectomy had a higher risk for Staphylococcus aureus infection. Overall, both regression results indicated that the type of procedure was associated with much higher risk relative to patient's background characteristics.
Multivariate Regression Analysis Displaying the Factors Associated with Staphylococcus aureus Infection (Inpatient Hysterectomy and Outpatient Hysterectomy Analyzed Separately)
Indicates statistical significant factors (p < 0.05).
aOR = adjusted odds ratio; CI = confidence interval; BMI = body mass index; CCI = Charlson Comorbidity Index.
All-cause HCRU and total healthcare costs
The unadjusted ED visits, hospital visits, mean hospital LOS, and reoperations for inpatient surgeries, respectively, were all significantly greater among patients with Staphylococcus aureus infection (46.9%, 31.9%, 7.8 days, and 14.4%, respectively) versus other infection (38.7%, 20.8%, 4.8 days, and 6.5%; all p < 0.05) or without infection (15.5%, 5.0%, 2.7 days, and 0.8%; all p < 0.05; Table 5). Outpatients with Staphylococcus aureus infection had more ED visits (40.0% vs. 13.7%; p < 0.05), hospital visits (17.8% vs. 3.3%; p < 0.05), and re-operations (11.1% vs. 0.4%; p < 0.05) and longer hospital LOS (mean, 1.6 vs. 0.1 days; p < 0.05) than those without infection (Table 5).
All-Cause Descriptive Healthcare Resource Utilization during One Hundred Twenty Days Post-Index for Elective Hysterectomy
Excludes the index hospital surgery, these visits are post-index hospital surgery.
Indicates statistical significance against Staphylococcus aureus infection group (p < 0.05).
HCRU = healthcare resource utilization, LOS = length of stay, SD = standard deviation.
Based on multivariable analysis, both inpatients and outpatients with Staphylococcus aureus infection had more hospital visits compared with those without infection (inpatient: adjusted odds ratio [aOR]: 4.8, 95% confidence interval [CI]: 3.0–7.6; p < 0.0001; outpatient: aOR: 6.5, 95% CI: 2.4–11.8; p = 0.0002) or with other infection (inpatient: aOR: 1.1, 95% CI: 0.7–1.8; p = 0.2187; outpatient: aOR: 1.2, 95% CI: 0.4–2.8; p = 0.1791). Patients with Staphylococcus aureus infection after inpatient or outpatient surgery were also more likely to have all-cause re-operations than patients without infection (inpatient: aOR: 14.47, 95% CI: 7.9–16.3; p < 0.0001; outpatient: aOR: 22.3, 95% CI: 14.7–35.5; p < 0.0001) or patients with other infection (inpatient: aOR: 1.7, 95% CI: 0.9–3.0; p = 0.3597; outpatient: aOR: 2.1, 95% CI: 0.4–10.3; p = 0.5479). After inpatient hysterectomy, patients with Staphylococcus aureus infection had a mean total (adjusted) LOS that was approximately 30% longer than patients without infection (p < 0.0001) and approximately 10% longer than patients with other infection (p < 0.0001). After outpatient hysterectomy, patients infected with Staphylococcus aureus had approximately 65% longer LOS versus no infection (p = 0.0482) and 24% longer LOS versus other infection (p = 0.4078).
The mean total costs of healthcare visits (unadjusted; U.S. dollars) across different surgery types were higher for patients with Staphylococcus aureus infection (inpatient: $18,261; outpatient: $4,422) than for those without infection (inpatient: $6,171, p < 0.0001; outpatient: $905, p = 0.0023) or other infection (inpatient: $11,207, p = 0.0117; outpatient: $3,005, p = 0.2117). Most hysterectomy-related costs were associated with hospital visits for both surgical settings (Fig. 2). For inpatients with Staphylococcus aureus infection, the overall costs after abdominal hysterectomies were higher than costs after laparoscopic or vaginal hysterectomies. After adjustment for confounding factors, the mean total costs of treatment for patients with Staphylococcus aureus infection were higher than for patients without infection (inpatient: 91% higher, p < 0.0001; outpatient: 250% higher, p < 0.0001) or other infection (inpatient: 25% higher, p < 0.0001; outpatient: 9% higher, p = 0.5268).
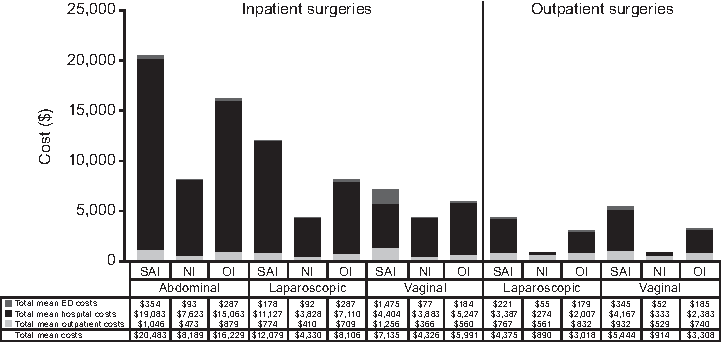
Total mean costs per infection category. ED = emergency department, NI = no infection, OI = other infection, SAI = Staphylococcus aureus infection.
Discussion
To our knowledge, this is the first study to evaluate the clinical and economic burden of culture-confirmed Staphylococcus aureus infection after elective hysterectomy using an integrated managed care healthcare system. Few studies have evaluated the incidence of post-operative Staphylococcus aureus infection after hysterectomies, particularly outpatient hysterectomies. In addition, most literature is focused on SSI alone and is not pathogen-specific.
In the current study, the incidence of Staphylococcus aureus infection was higher for inpatient versus outpatient surgeries (0.8% vs. 0.4%), largely because of the higher infection rate (1.2%) associated with more invasive abdominal surgeries conducted in the inpatient setting. Interestingly, the incidence of Staphylococcus aureus infection in patients who had laparoscopic and vaginal hysterectomies was similar between inpatient and outpatient surgeries, suggesting procedure type is a more important influence on infection risk than surgical setting. In our study, approximately one in 200 patients experienced Staphylococcus aureus infection, regardless of setting. Using hospital administrative claims data, Campbell et al. [13] reported the overall incidence of post-operative Staphylococcus aureus infection was 0.6% at 90 days after gynecologic/genitourinary procedures, similar to our observed rate of 0.8% at 90 days for inpatient hysterectomies. The higher incidence of postoperative Staphylococcus aureus infection in this study is likely because of better capture of infections after hospital discharge and/or infections not treated at the initial surgical hospital.
Numerous risk factors and clinical characteristics were associated with postsurgical Staphylococcus aureus infection. Most were consistent with prior studies, including hysterectomy route, anemia, malnutrition, diabetes, hypertension, obesity, cancer/malignancy, and long pre-operative stays/prior hospitalizations, and drug/substance abuse [5,13,14,24–27]. In our study, patients with Staphylococcus aureus infection were older than those without infection or with other infection, consistent with prior literature indicating that women older in age have an association with increased risk of SSIs, compared with younger women [28,29], and that patients with MRSA or MSSA are older than those without Staphylococcus aureus infection [13]. Similar to Campbell et al. [13], we found patients with Staphylococcus aureus infection had more chronic comorbidities and higher CCI scores than patients without infection. Our results also indicated that the hysterectomy route had a more profound impact on Staphylococcus aureus infection risk than other risk factors, although the reasons for choosing a specific route were not captured.
Post-operative Staphylococcus aureus infection is associated with higher HCRU, and patients with Staphylococcus aureus infection were more likely to have all-cause hospital visits and re-operations than patients without infection. A similar pattern was observed in comparison with patients with other infection, although this trend was not statistically significant. The estimated cost per SSI ranges from $11,000 to $35,000, and the estimated total cost in the United States is $3–10 billion annually [30]. In 2005, Noskin et al. [11] estimated the total economic burden of Staphylococcus aureus infection as $14.5 billion for all inpatient stays, of which $12.3 billion was attributable to surgical inpatient stays. After controlling for patient differences, the mean total costs were still significantly higher for both inpatients and outpatients with Staphylococcus aureus infection versus patients without infection.
Given that Staphylococcus aureus is the leading cause of SSIs in the United States, additional preventive interventions are needed [13,31–33], particularly among high-risk patients. New interventions could potentially reduce readmissions, HCRU, and costs and improve health outcomes. Both patients and healthcare providers should take appropriate steps to minimize infections. Within a managed-care setting, our findings can be used to guide efforts to develop effective infection control interventions that help mitigate the risk of Staphylococcus aureus infection, especially within populations at high risk because of comorbidities or procedural characteristics.
The strengths of this study include the use of an integrated database in which patients are followed throughout the continuum of care, which more accurately captures infections diagnosed in the outpatient setting. Also, we evaluated Staphylococcus aureus infection rates for both inpatient and outpatient surgeries, in contrast to prior studies, which focused primarily on inpatient surgeries. We also used clinical microbiology laboratory reports to identify Staphylococcus aureus infection and categorize patients with Staphylococcus aureus infections, other infection, or no infection, which has not been previously presented.
One major limitation of this study is that costs were potentially underestimated because only the cost of the ED, outpatient, and hospital visits were evaluated and not the cost of any procedures or additional actions (e.g., laboratory work, imaging studies, and consultations) related to the visits. Second, only Staphylococcus aureus infection rates based on positive clinical microbiology reports were evaluated, and this likely underestimates the incidence of Staphylococcus aureus infection because some healthcare providers administer antibiotic agents without taking cultures or before culture collection, which may result in a negative bacterial culture. Furthermore, patients whose infection status was not determined (e.g., patients treated with antibiotic agents but not cultured) were included in the same group as those who had no infection. On this basis, an infection may be present despite an absent or negative bacterial culture. Only patients who failed treatment or who were more clinically severe would have had cultures taken and this may also have contributed to underestimating the incidence of Staphylococcus aureus infection. We also note that clinical microbiology reports alone cannot distinguish between superficial and invasive infections. Third, we did not control for smoking history in our analyses. We also lacked access to data on duration of hysterectomy; longer procedures are associated with higher postoperative infection rates. Last, this study cohort was from an integrated healthcare system, which may not be representative of patients without insurance or with other types of insurance. However, our findings are similar to prior studies in other populations.
In summary, Staphylococcus aureus infection after hysterectomy constitutes a substantial medical burden, considering the large number of hysterectomies performed each year. The incidence rate of culture-confirmed infection was largely determined by procedure type rather than clinical setting. HCRU and corresponding costs were higher for patients with culture-confirmed Staphylococcus aureus infection than for those without infection or with other infection. These results support the development and/or application of additional strategies to prevent Staphylococcus aureus infection. Knowledge and understanding of risk factors for Staphylococcus aureus infection may enable surgeons and healthcare policymakers to implement innovative targeted preventive measures.
Footnotes
Acknowledgments
The authors wish to thank Dr Jim Nomura, MD, of the Southern California Permanente Medical Group, for his assistance with this study. Editorial support was provided by Chu Kong Liew, PhD, and Tom Gegeny, PhD, of Engage Scientific Solutions and was funded by Pfizer Inc.
Funding Information
This study was funded by Pfizer Inc.
Author Disclosure Statement
This study was conducted and completed when N.R and K.J.L were both employed by Kaiser Permanente Southern California. N.R. and K.J.L. do not have any financial interests or potential conflict of interest with regard to the work. H.Y. and E.B. are employees of Pfizer Inc.