
Abstract
Background:
The aim of this study was to determine whether incision irrigation with chlorhexidine gluconate (CHG) reduces surgical site infections (SSIs) in pilonidal disease surgery.
Methods:
Between 2013 and 2018, patients who underwent wide excision with primary closure for pilonidal disease were enrolled in this prospective observational multi-institutional cohort. The incision was irrigated with either saline or 0.05% CHG before skin closure. The infection risk of each patient was determined by the National Nosocomial Infection Surveillance System. Post-operative site care and follow-up were carried out according to the U.S. Centers for Disease Control and Prevention guideline by two surgeons blinded to the irrigation solution used. Surgical site infection rates in the saline and 0.05% CHG groups were compared. The secondary outcomes were seroma formation, incision dehiscence, and time to healing.
Results:
There were 129 patients in the control group and 138 patients in the CHG group. The mean age was 25.1 ± 5.4, and 225 patients (84.3%) were male. Surgical site infection was seen in 35 patients (13.1%): 26 (20.2%) in the control group and 9 (6.5%) in the CHG group (p = 0.001). There were no differences in seroma formation (n = 12; 9.3% in the control vs n = 12; 8.7% in the CHG group; p = 0.515) or incision dehiscence (n = 9; 7% in the control vs n = 9; 6.5% in the CHG group; p = 0.537). The primary healing rate was higher in the CHG group (n = 130; 94.2%) than in the control group (n = 104; 80.6%). Time to healing was 20.5 ± 7.8 days in the control group and 16 ± 4.3 days in the CHG group (p < 0.001).
Conclusion:
Intra-operative incision irrigation with CHG decreased the SSI rate and time to healing in pilonidal disease surgery. Further randomized trials should focus on specific irrigation methods and procedures to build a consensus on the effect of incision irrigation on SSIs.
Pilonidal disease (PD) is a challenging condition caused by hair entrapped in the gluteal cleft. The disease is characterized by epithelized sinuses and can be asymptomatic, although acute abscess or chronic painful fistulas can occur. The risk factors for PD include obesity, dense local hair structure, deep gluteal cleft, poor hygiene, long duration of sitting, and increased sweating [1,2]. Maceration of the skin, contamination from the anus and other site problems occur too frequent because of the anatomic location. Both conservative and surgical treatments require time-consuming site care and are associated with high complication rates, workday loss, and costs [3]. There always has been a quest for less invasive treatments such as simple drainage/curettage, application of sclerosing agents, laser ablation, and endoscopic debridement of sinuses in order to avoid the high morbidity rates of standard surgery [4–7]. However, surgery remains the definitive and most commonly preferred treatment [8]. Site complications are the major cause of morbidity after PD surgery. Surgical site infection (SSI) after wide excision and primary closure has been reported in as many as 38% of cases and to be associated with a high recurrence rate [9].
The practice most often used to prevent SSI is intra-operative site irrigation with antiseptic solutions. However, there is no consensus on the solutions to be used or the appropriate duration of the irrigation [10,11]. Chlorhexidine gluconate (CHG) is a safe and effective topical antiseptic that has been in clinical use for antisepsis of tissues and protheses for more than five decades [12]. In vitro studies showed that CHG solutions are more effective with shorter exposure time at eradicating microorganisms than are povidone–iodine and antibiotic solutions [13,14]. Several studies have shown that 0.05% CHG solution can be used for antisepsis of skin and surgical prostheses without impairing site healing or granulation tissue formation [15]. However, intra-operative wound irrigation with CHG has been discussed in only limited and retrospective studies in the literature. The aim of this study was to reveal whether CHG irrigation reduces the SSI rate in patients undergoing surgery for PD, which has a substantial risk of incision complications.
Patients and Methods
The study protocol was approved by the Dokuz Eylul University Ethics Committee (Approval no. 20101193-19). All the patients gave written informed consent for the surgery and participating in the study. The study protocol was put into practice at two institutions in 2013, after one of the authors (CT) adopted the use of routine intra-operative site irrigation with 0.05% CHG. Another surgeon (NCA) kept the routine irrigation custom of 0.09% saline. Since then, 293 patients with primary PD undergoing wide excision and primary closure were enrolled in a prospectively recorded database. The site complications were compared in the CHG and saline groups.
The exclusion criteria were age <18 years, acute abscess, use of an antibiotic within one week before the operation, surgical techniques other than wide excision and primary closure, use of antimicrobial sutures, use of a drain, hypersensitivity to cefuroxime axetil or metronidazole, and post-operative use of antibiotics. Patients who had acute abscess at presentation were treated by drainage and antibiotics and then underwent surgery. The surgical site was irrigated by bulb syringe before skin closure for one minute with 0.09% NaCl in the control group and 0.05% CHG–distilled water (Acar Kimya, Istanbul, Turkey) in the study group. The management of the groups was otherwise identical.
The primary end-point was the SSI rate. Secondary end-points were seroma formation, incision dehiscence, and time to healing.
Surgery
All the procedures were performed with the patient under spinal anesthesia in the prone position. Antibiotic prophylaxis was given 30 minutes before incision with 1.5 g of cefuroxime axetil and 500 mg of metronidazole. The surgical site was shaved, and skin antisepsis was provided with povidone–iodine. The pilonidal cyst was removed with clean surgical borders (Fig. 1). The wound was irrigated for one minute, 1-0 monofilament polypropylene (Prolene®; Ethicon, Somerville, NJ USA) retention sutures were prepared, and the subcutaneous tissue was closed with 3-0 polyglactin (Vicryl®; Ethicon) sutures. Skin closure was created with interrupted 3-0 polypropylene (Prolene®, Ethicon), and retention sutures were tied over a compression gauze (Fig. 2). The post-operative infection risk was estimated according to the National Nosocomial Infection Surveillance System (NNIS) and recorded for every patient at the end of surgery [16].

Preparation of surgical site and excision of sinus. (
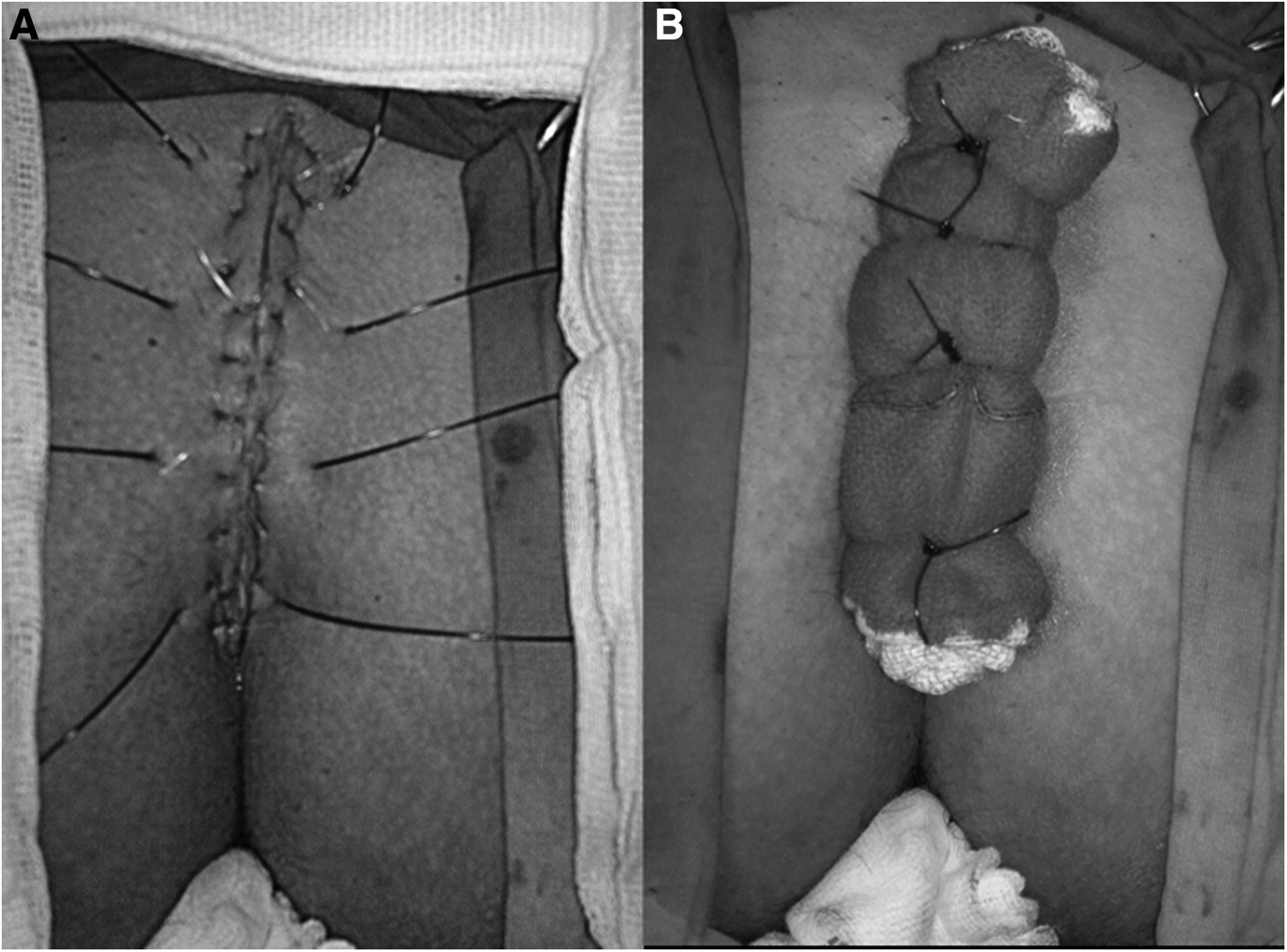
Closure of site (
Follow-up and definition of complications
Patients were trained in hygiene and hair removal at the surgical site and discharged on the day of surgery. A surgeon at each institution (AKD, YO) blinded to the type of irrigation used evaluated the incision on post-operative days (POD) 1, 3, 7, 15, and 30. The surgical dressing was removed by the blinded surgeon on POD 1; sites were swabbed with iodine solution and a new dressing applied. On POD 3, this dressing was removed, and the site was left open; patients were allowed to shower. No patients reported discomfort with respect to dressings or significant post-operative pain. In uneventful cases, retention sutures were removed on POD 7 and skin sutures on POD 14.
Surgical site infection
The definitions of the U.S. Centers for Diseases Control and Prevention Guideline were used to identify site complications [17]. (17).
Superficial SSI: Infection of the skin and subcutaneous tissue occurred within 30 days with at least one of the following
Purulent drainage (with or without wound culture);
Positive wound culture;
Incision opened by the surgeon (with at least one of the findings pain, tenderness, swelling, redness, and heat) unless the culture was negative;
Diagnosis of superficial incisional infection made by the physician.
Deep SSI: Infection of deep tissues occurred within 30 days with at least one of the following
Purulent drainage from the deep incision;
A deep incision spontaneously dehisces or is opened by the surgeon with at least one of fever, pain, tenderness unless a culture is negative,
Abscess or deep infection detected radiologically or histologically;
Diagnosis of deep incisional infection made by a surgeon or attending physician.
Incision dehiscence
Superficial or partial separation of the incision edges occurred without any signs of infection. Spontaneous separation of the entire incision is described as complete dehiscence and included in deep SSI (see above).
Seroma
Fluid collection was seen in the subcutaneous tissue without any sign of infection.
Cultures
Cultures were obtained when any incision complications were observed. If there was a strong suspicion of severe infection (fever, increased white blood cell count, wide cellulitis), empirical antibiotics were started before culture confirmation. Daily open dressing or negative-pressure wound therapy were performed in patients with SSI. Either primary closure or secondary healing was preferred depending on the condition of the site. Incision dehiscence was closed primarily after ensuring negative culture. When a seroma was detected, culture and intermittent aspiration of the fluid was performed. Time to healing was defined as the number of days until the skin sutures were removed in uncomplicated cases and healing without a need for site care in complicated cases.
Sample size and statistical analysis
An SSI rate of 25% was accepted in the control group. We estimated that CGH irrigation might reduce the SSI rate to 10%. The minimum sample size for α = 0.05 and 90% power was 133 patients in each group.
Data were analyzed with SPSS for Windows v. 21. Continuous variables were expressed as means and standard deviation, categorical variables as frequency and percentages. Association between categorical variables and morbidity was measured by the χ2 test. Association between continuous variables and morbidity was measured by the independent samples t test. P < 0.05 was accepted as statistically significant.
Results
Of the 298 patients enrolled in the database between 2013 and 2018, 267 were included in the analysis. The reasons for exclusions and a flow diagram of the study are given in Fig. 3. There were 129 patients in the control and 138 patients in the study group. The mean age was 25.1 ± 5.4, and 225 patients (84.3%) were male. The mean Body Mass Index (BMI) was 25.9 ± 2.8. A relevant family history was present in 33 patients (12.4%), and 123 patients (46.1%) were smokers. The mean duration of the symptoms was 12 ± 19.1 weeks, and the NNIS score was 0.12 ± 0.33. The institutional distribution was as follows; 189 patients (70.8%) at institution 1 and 78 (29.2%) at institution 2. There was no difference between these groups in demographic or clinical characteristics (Table 1).

Flow diagram of study.
Demographic and Clinical Characteristics of Patients
BMI = Body Mass Index; CHG = chlorhexidine gluconate; NNIS = National Nosocomial Infections Surveillance System; PD = pilonidal disease, SD = standard deviation.
The mean operative time was 27.4 ± 5.7 minutes. The groups were similar regarding the site dimensions and surgical characteristics (Table 2). Overall, primary healing was observed in 234 patients (87.6%), being higher in the CHG group (n = 130; 94.2%) than in the control group (n = 104; 80.6%) (p = 0.001). The mean time to healing was 18.2 ± 6.6 days: 20.5 ± 7.8 days in the control group and 16 ± 4.3 days in CHG group (p < 0.001) (Table 3). The details of the patients who had positive wound cultures are given in Table 4.
Surgical Characteristics of Patients (Mean ± Standard Deviation)
CHG = chlorhexidine gluconate; SD = standard deviation.
Comparison of Complications in Control and Study Groups
CHG = chlorhexidine gluconate; SD = standard deviation.
Details of Patients with Surgical Site Infection
CHG = chlorhexidine gluconate.
Discussion
Incision complications constitute a substantial part of the major morbidity after PD surgery. In this study, we found that irrigation with 0.05% CHG reduced the SSI rate and workday loss and provided a higher rate of primary healing.
The risk factors for SSI after PD surgery have been defined as older age, obesity, male gender, accompanying chronic gastrointestinal disease, midline closure techniques, smoking, and lack of antibiotic prophylaxis [18,19]. Our study groups were similar in demographic and surgical characteristics. The SSI risk estimated by the NNIS score likewise did not differ between the groups. The surgical technique preferred in our institution is a midline closure, which seems to carry a higher SSI risk. Moreover, the tendency to use minimally invasive approaches has been rising during recent years. As our study started in 2013 and we have not observed unacceptable results from wide excision and primary closure, we maintained the study protocol until the enrollment reached adequate power. Besides, our overall SSI rate of 13.1% was relatively satisfying compared with our historical series and the literature [3,20,21].
Incision irrigation is an inexpensive and easy method believed to prevent SSI [22]. Several antiseptic and antibiotic solutions have been suggested for such irrigation; however, there are no evidence-based recommendations. Randomized studies are limited and heterogenous regarding surgical procedures and antiseptics. In a recent meta-analysis, 21 studies, including intra-peritoneal, mediastinal, and incisional sites irrigated with povidone–iodine, saline, and antibiotic solutions were reviewed; and low-quality evidence for the value of aqueous povidone–iodine solution to reduce the SSI rate was reported [23]. No beneficial effect of antibiotic solutions was found. This meta-analysis involved no studies with CHG solution. Normal et al. published a Cochrane review of studies comparing irrigation with no-irrigation (20 studies; 7,192 patients), antibacterial irrigation with non-antibacterial irrigation (36 studies; 6,136 patients), and two paired solutions of the same type (e.g. povidone–iodine with superoxidized water) (10 studies; 2,118 patients). Those investigators reported only a low-certainty beneficial effect for antibacterial irrigation. This review of 59 randomized trials and 14,738 patients analyzed the subgroups in terms of several surgical procedures and irrigation solutions; none of the subgroups revealed remarkable results specific to PD or irrigation with CHG [11].
There are no data in the literature assessing the effect of intra-operative site irrigation with CHG in PD. In a study of knee arthroplasty, 248 patients in a 0.05% CHG irrigation group were compared with 411 historic patients receiving 0.9% NaCl; and no difference in SSI rates was found [24]. This study was of a retrospective design and underpowered. Our group recently published a report using the same design of the present study and presented the results of CHG irrigation in ileostomy closure [25]. The SSI rate was 4.8% in the CHG group and 31.6% in the saline group (p < 0.001). Seroma (13.3% versus 1.6%; p = 0.014) and wound dehiscence (31.6% and 4.8%; p = 0.001) also were significantly more common with saline irrigation. In PD, we found no difference in seroma and incision dehiscence rates between CHG and saline irrigation. Both studies were prospective cohorts.
Apart from non-randomized design, our study has some other limitations: Cost analysis and long-term follow-up for recurrence were not performed. Moreover, the study protocol was conducted simultaneously in two institutions by different surgeons. There was no difference in SSI rate between the institutions. Nevertheless, considering that the surgeon is one of the most important independent variables, the major drawback of our study is in not performing a multivariable analysis to evaluate the independent effect of the institution and the surgeon.
Intra-operative incision irrigation with 0.05% CHG is an easy, safe, and effective method to prevent SSI and workday loss in PD surgery. The literature on intra-operative site irrigation is heterogenous and scarce for CHG. Large randomized trials specific to different surgical procedures are needed to establish standardized recommendations on site irrigation.
Author Disclosure Statement
The authors declare no conflicts of interest.