
Abstract
Background:
More than 145,500 abdominal abscesses occur annually in the U.S. Percutaneous catheter drainage (PCD) is the primary treatment for clinically significant intra-abdominal collections (IACs), but only approximately 90% of all IACs are treatable with PCD. This leaves a significant number of patients facing long courses of management, including multiple interventions. Minimally invasive debridement techniques are now employed regularly for the treatment of infected necrosis caused by acute pancreatitis. We describe the use of minimally invasive videoscopic debridement techniques employed as part of a “step-up” approach to resolve IACs of other etiologies that are unresponsive to PCD.
Methods:
Data of all patients undergoing this procedure at a tertiary referral academic center from 2015 to 2017 after failure of different PCD techniques were analyzed retrospectively.
Results:
Four men and two women, mean age 54.6 years (range 26–70 years), with refractory IACs (mean drainage time 91.3 days; mean number of drainage procedures 4.6) following a variety of surgical interventions and inflammatory conditions underwent either video-assisted retroperitoneal debridement or sinus tract endoscopic debridement with a rigid or flexible endoscope. Technical success was achieved in all cases, and clinical success was observed in five cases. No immediate procedural complications were detected. The mean hospital stay and post-procedure drainage times were 5.5 and 25.2 days, respectively. There were no recurrent IACs.
Conclusion:
Minimally invasive debridement techniques can safely resolve IACs refractory to standard PCD techniques. Employment of these techniques as part of a step-up approach may reduce the morbidity and duration of drainage for the thousands of patients treated annually who have refractory IACs, whatever their etiology.
Intra-abdominal collections (IACs) are a significant source of morbidity and death after abdominal surgery, inflammatory intra-abdominal conditions, and trauma [1]. Percutaneous catheter drainage (PCD) is the primary treatment for clinically significant IACs [2-4], but only approximately 90% of all IACs are treatable in this way. This leaves a large number of patients facing long courses of percutaneous drainage and multiple other percutaneous interventions [5].
A step-up approach, in which percutaneous drainage is followed by minimally invasive necrosectomy when percutaneous drainage fails to resolve the infected necrosis, has become the standard of care for the treatment of infected pancreatic necrosis [6,7]. However, there is no standard treatment for intra-abdominal collections unrelated to pancreatitis that cannot be resolved with percutaneous drainage. All surgeons will be familiar with patients suffering from recalcitrant IACs who undergo multiple percutaneous procedures and long courses of percutaneous drainage. We report here the first series of patients undergoing minimally invasive debridement as part of a step-up approach for the treatment of IACs unrelated to acute pancreatitis and refractory to percutaneous drainage. The objective of this study was to describe and evaluate our experience with minimally invasive necrosectomy in the management of a series of patients suffering from IACs unrelated to pancreatitis and refractory to percutaneous drainage.
Patients and Methods
This study was approved by the Institutional Review Board at Massachusetts General Hospital. All patients 18 years or older who underwent minimally invasive debridement procedures for IACs at one tertiary referral academic center from the start of January 2015 until the end of September 2017 were included. The exclusion criteria for our study were relation of the IAC to acute pancreatitis.
For each patient, we reviewed the electronic medical record systematically to identify demographics, clinical features, imaging collection characteristics, procedure details, technical success and clinical improvement, post-operative complications, length of hospital stay, and death. All post-operative images were reviewed. “Technical success” was defined as radiographic resolution of IAC on post-operative computed tomography (CT) scan. “Clinical success” was defined as complete resolution of the IAC, abatement of symptoms, and drain removal without IAC recurrence. “Complications” were all adverse events related directly to debridement from the time of surgery to complete resolution of the IAC.
Procedure description
All the procedures were done by the same surgeon with the patient under general anesthesia using minimally invasive debridement techniques as previously described for the management of infected pancreatic necrosis. In brief, video-assisted retroperitoneal debridement (VARD) was performed by arranging the patient in a partial lateral decubitus position to expose the retroperitoneally routed percutaneous drainage catheter leading into the IAC. A 5-cm incision was made around the drainage catheter, and dissection was continued along the catheter until the IAC was entered. Retractors and a 10-mm, 0° laparoscope were then introduced into the cavity, and infected fluid and necrotic tissue were removed by debridement with forceps and irrigation. When the IAC was debrided fully, drainage catheter(s) (one or two) were placed; and the incision was closed in layers [8,9]. In one case (Patient 5), after debridement of the dominant cavity by VARD, a flexible endoscope was advanced along an indwelling drain through a narrow isthmus into a satellite presacral collection, which was debrided using the flexible endoscope.
Sinus tract endoscopy (STE) was performed by positioning the patient on a radiolucent table with the percutaneous drain entering the IAC accessible. Under fluoroscopic guidance, an Amplatz wire was advanced through the drain into the target IAC and the drain removed. The drain tract was then dilated using a 30F Bard X-Force nephrostomy balloon dilator (Bard Medical, Covington, GA). The associated working sheath was then advanced over the balloon until the tip entered the IAC. A rigid nephroscope was then advanced through the sheath into the IAC and debridement performed under continuous saline irrigation. When the IAC was fully debrided, a wire was again advanced into the cavity and a drainage catheter advanced over the wire under fluoroscopic guidance and sutured into place [10,11].
Case Reports
History of Patient 1. (
Course of Patient 2. (

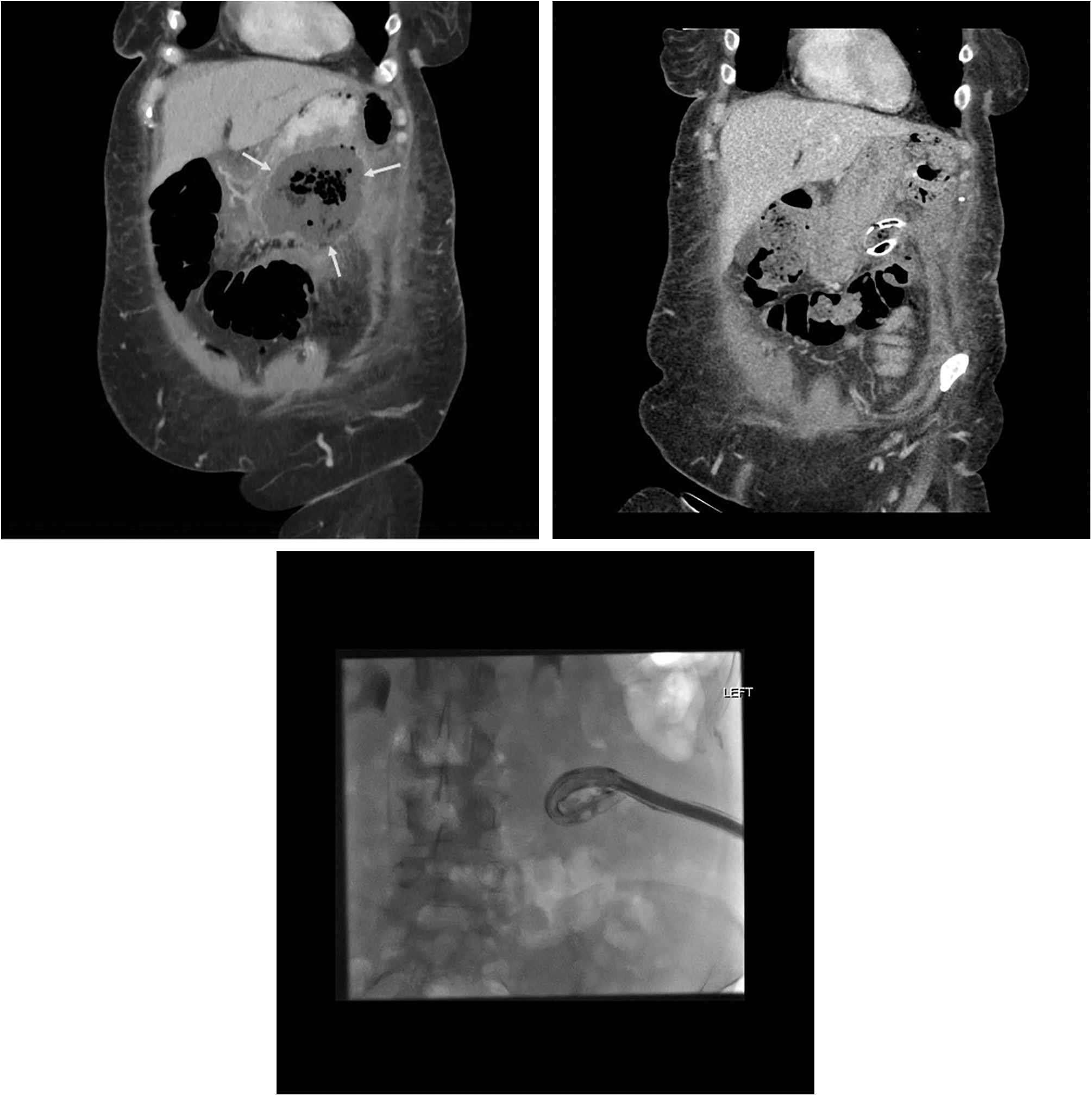
Computed tomography scans of Patient 3. (

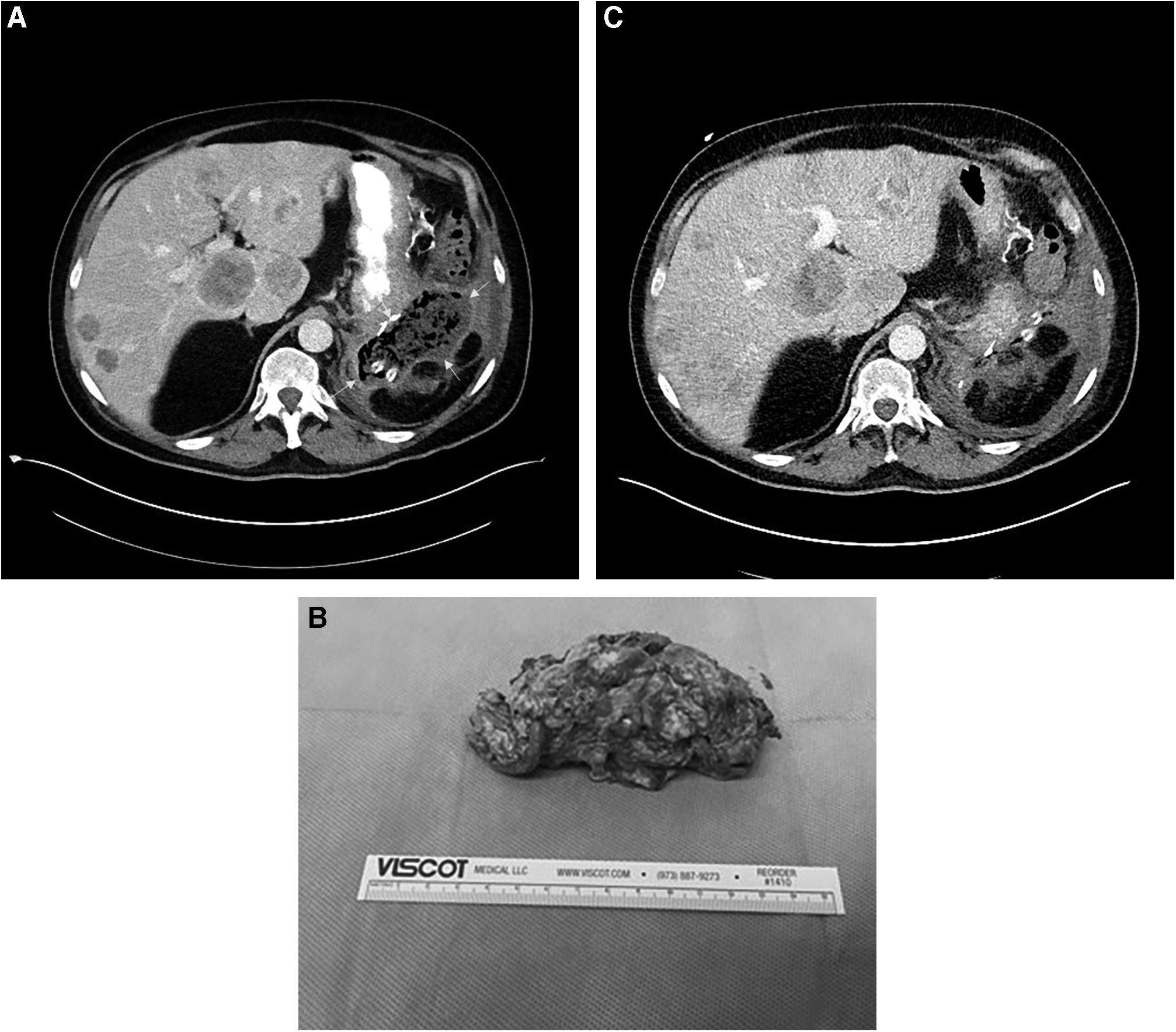
Computed tomography scans of Patient 6. (
Results
The cases above represent all six seen from January 2015 until September 2017 who underwent minimally invasive debridement for IACs after a variety of surgical interventions and inflammatory conditions. The mean drainage time before our intervention was 91.3 days, and the mean number of drainage procedures was five, including drain placement, re-positioning, and exchange. With minimally invasive debridement, technical success was achieved in all six collections. Clinical success was observed in five of the six of our cases; one patient (Patient 5) required a drain to be left in place to allow safe initiation of chemotherapy. This patient was the only one to develop a recurrent IAC. No immediate procedural complications were detected. The mean duration of post-operative drainage after our procedure for five of our patients was 25.2 days. A description of our population demographics and collection characteristics has been recorded in Table 1.
Patient Characteristics and Outcomes
CT = computed tomography, POD = post-operative day.
Discussion
Percutaneous drainage of IACs has become the standard of care and has essentially replaced surgical management as first-line treatment. Recent literature clearly demonstrates higher clinical success rates and lower complication rates for radiologic compared with surgical drainage [5]. However, in a significant minority of IACs, percutaneous drainage cannot resolve the lesion, with failure rates ranging from 9%–26.9% [12–14]. The total burden of these refractory IACs is not defined in the literature; but given the high incidence and prevalence of IACs, even this relatively small percentage of refractory IACs likely amounts to thousands and possibly tens of thousands of cases annually.
A variety of techniques has been described to treat refractory IACs, including catheter upsizing, catheter exchange [13], catheter manipulation, placement of additional drainage catheters [14], and instillation of fibrinolytic agents. Even with judicious use of these adjuncts, there is a subset of IACs that will not respond fully to percutaneous drainage. Gervais et al. [15] describe surgery as the only solution after failure of PCD for management of refractory IACs related to appendicitis and Crohn's disease, and this may be the best option in these diseases and in many scenarios. However, many patients with IAC such as those described here are in the early post-operative period or have significant co-morbidities, including advanced malignant disease, that render surgical re-exploration exceptionally risky. Surgeons are understandably reluctant to re-operate under these circumstances, but this reluctance can translate into prolonged patient suffering and significant radiologic resource utilization when a low-yield percutaneous strategy is stubbornly pursued. The median time from initial drainage to debridement in our study was more than 90 days, and two patients waited five months, while the median number of percutaneous procedures was five. Thus, a minimally invasive technique that offers a choice between prolonged, futile percutaneous interventions and risky open surgery is a welcome addition to the arsenal of techniques used to treat IACs.
A “step-up” approach beginning with minimally invasive drainage and escalating to minimally invasive debridement is the current standard of care for the management of symptomatic necrotic collections related to acute pancreatitis [6,7]. Some techniques for treating necrotic collections related to pancreatitis have been used already to treat post-operative IACs. Ulla-Rocha et al. [16] described endoscopic ultrasound-guided transluminal drainage for post-operative IACs. However, the use of such drainage is limited to well-demarcated IACs abutting endoscopically accessible portions of the gastrointestinal tract. In contrast, VARD and STE can reach any IAC accessible by PCD and thus have the potential to access any percutaneously drainable IAC that is refractory to treatment.
When exactly to employ these techniques is open to debate. A number of factors have been associated with failure of percutaneous drainage, including septations or loculations, the presence of necrotic tissue within the IAC, fluid attenuation higher than 20 HU, and the presence of an enteric fistula [5,13,17,18]. In our series, at least four of the patients had pancreatic fistulas related to their initial surgical interventions, and this may be an important predictor of failure of percutaneous drainage. Enteric fistulas may be treatable by achieving IAC collapse and with the use of endoscopic adjuncts as in Patient 4. Gee et al. [18], from our institution, recommend a management algorithm for IACs persisting in spite of adequately positioned percutaneous catheters, including CT before catheter exchange to determine collection fluid density, catheter exchange, and fibrinolytic therapy. We recommend extending this algorithm to include minimally invasive necrosectomy when the original pathway proves inadequate. Our early experience suggests that persistent necrotic tissue in the IAC and persistent fever despite appropriate antibiotics and catheter position extending six weeks beyond the initial PCD should prompt consideration of minimally invasive debridement, although the data are too sparse to establish categorical criteria.
Our early experience with minimally invasive necrosectomy for IACs unrelated to pancreatitis is the first report in the literature and offers a novel approach to the treatment of the refractory IACs that frequently vex surgeons, interventional radiologists, and their patients. Although the number of patients we treated is too small to establish hard criteria regarding when to “step-up,” we can hope dissemination of these techniques will provide clinicians a new option for treatment of IACs when PCD clearly is going nowhere. Future studies should focus on early identification of patients who would benefit from these techniques before they are subjected to prolonged courses of percutaneous drainage.
Conclusion
Minimally invasive necrosectomy is effective and should be considered for the treatment of intra-abdominal and pelvic collections refractory to percutaneous drainage alone, whatever their etiology.
Footnotes
Author Disclosure Statement
We certify that all listed co-authors have no commercial associations that might create a conflict of interest in connection with submitted manuscripts. No grants or other forms of funding or assistance were utilized in the creation of this manuscript.
All the co-authors were integrally involved in the writing of this manuscript via study conception/design and/or data acquisition and analysis/interpretation. Furthermore, all authors made significant contributions to the drafting or critical revisions of the manuscript, and all authors gave final approval prior to submission for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.