
Abstract
Abstract
Background:
Jejunal diverticulitis is rare and usually an incidental diagnosis found on imaging. Its symptoms are non-specific. Hence, the diagnosis often is delayed, and a high mortality rate has been reported. The aim of this study was to review our experience in the management of jejunal diverticulitis and to propose a management algorithm.
Methods:
A retrospective review of all cases of jejunal diverticulitis seen from November 2015 to November 2018 was performed. Data collected included demographics, history of diverticulitis, risk factors, clinical presentation, biochemistry and imaging results, and management outcome.
Results:
Eight patients were identified during the study period, five females and three males with a median age of 71 years (range 61–85 years). One patient was on steroid treatment, and one patient had a history of jejunal diverticulitis. Abdominal pain was present in all patients, but other symptoms were variable. Two patients were initially believed to have constipation and were discharged home. All patients underwent a computed tomography (CT) scan for the diagnosis, showing that three had uncomplicated jejunal diverticulitis and five had localized perforation. Five patients were managed conservatively initially; two failed this treatment because of small bowel obstruction and persistent abdominal pain with rising inflammatory markers. Three underwent emergency laparotomy (two because of sepsis; one was thought to have a foreign body). There were no deaths. A proposed management algorithm is discussed.
Conclusions:
A CT scan is the mainstay for the accurate diagnosis of jejunal diverticulitis. The proposed algorithm can aid in selection of patients suitable for conservative management.
Jejunal diverticular disease is defined as the herniation of mucosa through sites of weakening on the mesenteric border of the jejunum. The incidence ranges from 0.23%–1.3% in autopsy series [1]. The condition usually is an incidental finding on imaging performed for abdominal pain. It has a predilection for the elderly. A few studies have reported it being more common in males, but a large French series found it to be more common in females [2]. Various theories have been postulated for its pathogenesis, which include intestinal dyskinesia, stasis, and bacterial overgrowth.
Given its rarity and non-specific presentation, jejunal diverticular disease is easily misdiagnosed as other more common conditions. Diverticulitis is the most common clinical presentation followed by other rarer presentations such as bowel obstruction, pseudo-obstruction, and bleeding. Occasionally, in the chronic form, patients present with malabsorption syndrome.
The evidence in the literature is sparse and largely limited to small case series and case reports [2-7]. There is no consensus on its management. Although the complications rarely are fatal, because of the common delay in diagnosis, it can carry high morbidity and mortality rates, as the patients usually are elderly. The reported mortality rates have improved significantly, from 20%–30% in the 1960s to 0–14% at present [8]. The aims of this study were to review all cases of jejunal diverticulitis and its management and to propose a management algorithm based on our experience and a review of the literature.
Patients and Methods
The approval for this study was obtained from the St. John of God Healthcare's ethics committee (ref no. 1506). A retrospective analysis was performed of all cases of jejunal diverticulitis managed in our institute from November 2015 (the commencement of our institute) to November 2018. For the literature review, the terms “jejunum,” “small bowel,” “diverticulosis,” “diverticulitis,” “laparotomy,” and “bowel resection” were searched for in the hospital's database. Patients with duodenal and colonic diverticulosis/diverticulitis were excluded from analysis. Data collected include basic demographics, co-morbidities, history of colonic or small bowel diverticulosis/diverticulitis, presenting symptoms and findings, biochemistry and imaging findings, management options (conservative or surgical), and outcomes of patients undergoing surgical intervention. The histopathology slides were used to confirm the diagnosis.
The criteria for the diagnosis of jejunal diverticulitis are based on the work of Lebert et al.: Identification of a diverticulum that (1) exhibits signs of inflammation and (2) is at the center of the mesenteric abnormalities [2]. Inflammation was detected as thickening of the diverticular wall, mesenteric fat stranding, and other mesenteric abnormalities.
Results
Eight patients were identified with the diagnosis of jejunal diverticulitis in the database. There were five female and three male patients with a median age of 71 years (range 61–86 years). Only one patient was on steroid treatment, for exacerbation of rheumatoid arthritis. No patients were taking non-steroidal anti-inflammatory drugs. One patient had a history of jejunal diverticulitis that had been managed conservatively.
For the clinical presentation, four patients had nausea and vomiting; all patients complained of abdominal pain (five generalized and three left-sided); two patients had altered bowel habits, and two patients reported fever. The median duration of symptoms was 2.5 days (range 1–7 days). Four patients were tachycardic; none was hypotensive; two patients were mildly tachypneic; three patients were febrile on admission; two patients were examined for localized peritonitis. On presentation, all but one patient had raised white blood cell count (median 11.5 × 109/L; range 7.8–21.1 × 109/L). The median of the C-reactive protein (CRP) concentrations was 132.5 mg/L (range 4.3–221 mg/L).
Two patients were assessed in the emergency department and believed to have constipation. They were discharged home but subsequently re-presented and underwent a computed tomography (CT) scan of the abdomen/pelvis, which confirmed acute jejunal diverticulitis (one with localized perforation). The remaining six patients underwent CT scans on admission. Of the six cases, four had jejunal diverticulitis with localized perforation (one causing small bowel obstruction) (Fig. 1). There was a case of jejunal diverticulitis that was indeterminate for localized perforation. There was a case where the radiologist reported “a foreign body consistent with a bone” within the jejunal diverticulum with surrounding inflammation (Fig. 2A, B).
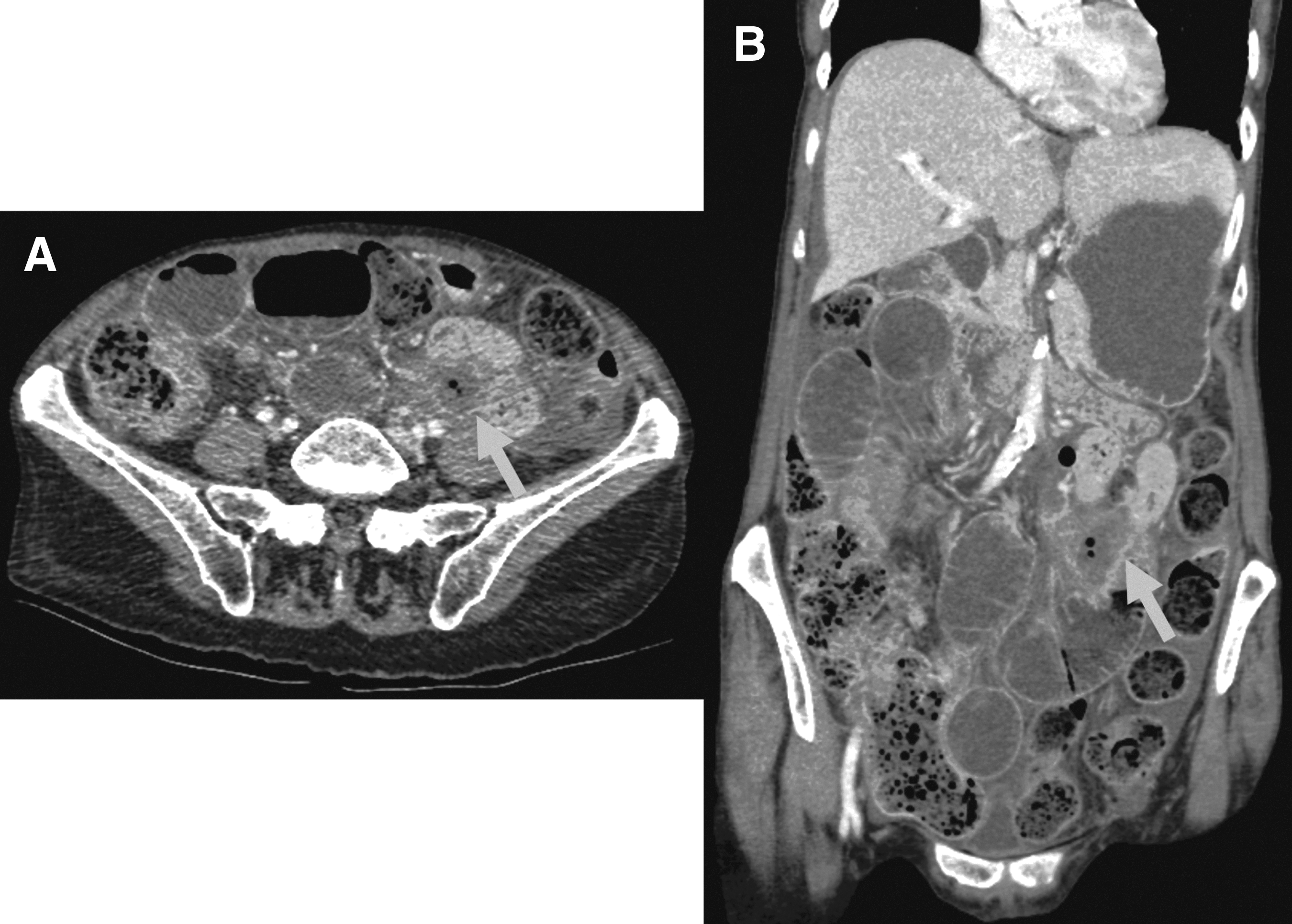
Axial (

Axial (
Five patients were managed non-operatively with intravenous antibiotics and bowel rest. Two failed this conservative management, requiring surgical intervention because of persistent abdominal pain with rising inflammatory markers and small bowel obstruction that failed a Gastrografin challenge (Fig. 3). Two patients underwent urgent laparotomy on presentation, as both had localized peritonism. The last patient, who was thought to have a foreign body, underwent a diagnostic laparoscopy and was found to have a contained perforation (Fig. 2C). The operation was converted to a laparotomy. A small bowel resection was performed, and the resected specimen showed an enterocolith within the perforated jejunal diverticulum and no evidence of a foreign body. On-table gastroscopy and small bowel run-through up to the terminal ileum did not reveal any foreign body.
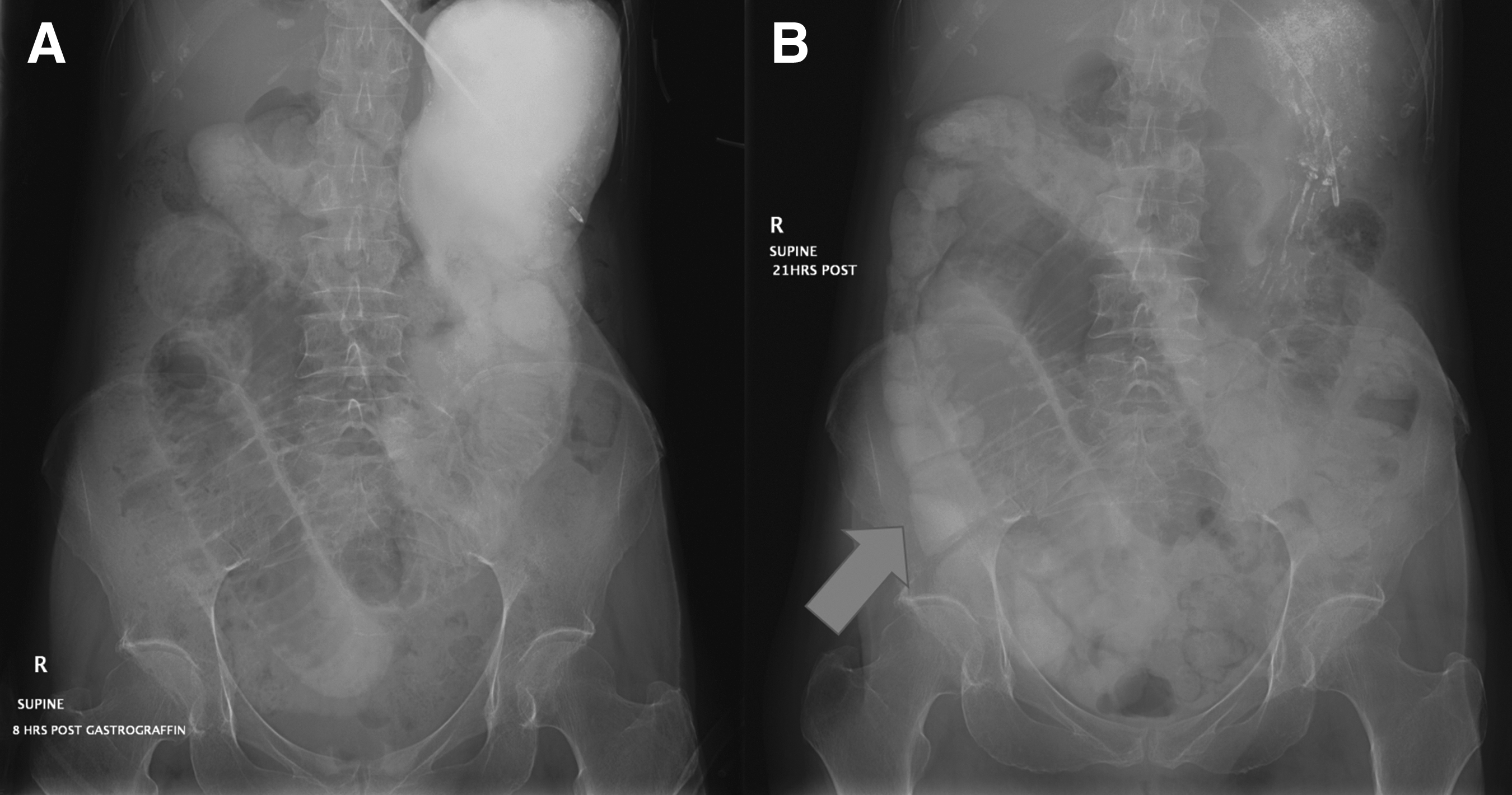
Abdominal radiographs after administration of Gastrografin. (
There were no cases of anastomotic leak or abscess formation. No patients required total parenteral nutrition. There was a case of atrial fibrillation post-operatively requiring cardioversion. The same patient (on steroids for rheumatoid arthritis) also developed melena on day 6 post-operatively. Gastroscopy showed gastric ulcers with no active bleeding, and he required transfusion of one unit of blood.
The median length of stay was six days (range 3–18 days). The histopathology results of the five cases confirmed the findings of one patient with jejunal diverticulitis and four with localized perforation. There was no recurrence with a median follow-up of 11 months (range 2–36 months).
Discussion
Jejunal diverticular disease has an estimated incidence of 0.3%–2.3%. The median age of 75 years in this study is consistent with other studies, where it has a predilection for elderly persons, those over the age of 60 years. Studies have shown mixed results of gender predominance likely because of the small cohorts. The lesion is commonly associated with colonic diverticular disease. Patients usually have multiple jejunal diverticula rather than a solitary diverticulum [2,9].
The condition usually is asymptomatic but can present acutely in various ways such as diverticulitis, perforation, bleeding, bowel obstruction, and pseudo-obstruction. It is believed that some patients experience chronic symptoms as a result of jejunal diverticulosis attributable to stasis and bacterial overgrowth, which can lead to malabsorption syndrome. Given its rarity and non-specific symptoms, jejunal diverticulitis is easily misdiagnosed. In a French series, there were only 33 cases of jejunal diverticulitis identified across three French hospitals over a period of nine years [2].
In our review of the literature, patients generally complain of abdominal pain. However, the site usually has non-specific changes unless there is perforation. Other symptoms, such as nausea/vomiting and altered bowel habits, also are variable. In a review by El-Haddawi et al., none of the nine patients was suspected to have small bowel diverticulitis clinically [8]. In another study, a significant proportion of the patients were found to have jejunal diverticulitis only intra-operatively [6]. Modern imaging such as CT of the abdomen and pelvis has become the mainstay of accurate diagnosis of the condition. Nevertheless, a review by Fintelmann et al. found that jejunal diverticulosis was diagnosed prospectively on CT in only two of 28 patients (7%). These patients had previous barium studies, the results of which may have been known to the radiologist prior to reporting [9]. Lebert et al. also systematically described the features of symptomatic diverticulum based on identification, location, size, contents, wall thickness, and associated complications [2]. Fintelmann et al. also classified the degree of diverticulosis on barium studies and CT scan [9]. The CT scan was more likely to underestimate the degree of diverticulosis. However, there was no correlation with the degree of diverticulosis and the likelihood of bacterial overgrowth syndrome.
There is no consensus about its management in the literature likely owing to its rarity, non-specific location of disease, and difficulty in accurate diagnosis despite the use of modern imaging. In this paper, we describe our experience with the management of jejunal diverticulitis and propose a management algorithm. Lebert et al. recently tried to classify the cases based on the Modified Hinchey classification originally described for colonic diverticulitis [2]. This classification is useful for its description but may not be applicable entirely, as the small bowel resection differs from large bowel resection, rarely require a two-stage approach.
In our proposed algorithm, the patients with acute presentations of jejunal diverticulitis are divided into three main groups: (1) Uncomplicated diverticulitis (Grade 1); (2) complicated diverticulitis (Grade 2); and (3) other presentations, including bowel obstruction (Grade 3). Uncomplicated jejunal diverticulitis corresponds to peri-jejunal inflammation or phlegmon. Complicated jejunal diverticulitis is further subdivided into localized contained perforation (Grade 2A) and perforation causing generalized peritonitis (Grade 2B). Pitfalls in CT interpretation can occur, especially in the presence of small diverticula in close contact with the inflammatory diverticulum, which can simulate extra-intestinal gas on CT [9-11]. Pneumoperitoneum does not necessarily equate to a perforation, as the distended diverticular mucosa may behave as a semipermeable membrane through which gas can travel until an equilibrium is reached [12]. The precise interpretation has significant implications for management.
The mainstay treatment for uncomplicated jejunal diverticulitis should be intravenous antibiotics and bowel rest. There is some evidence suggesting that the peak for perforation is 72 hours; we suggest monitoring the patient for clinical deterioration and inflammatory markers for at least 72 hours prior to discharge. There has been a case report of laparoscopic washout, but in that case, the diagnosis was a dilemma and hence the measure should not be advocated routinely [5]. Similarly, for localized contained perforation, non-operative management should be attempted unless the patient is hemodynamically unstable on arrival or has risk factors such as immunosuppression and steroid use. Garcia-Granero et al. have identified three criteria for conservative management: (1) No signs of diffuse peritonitis; (2) haemodynamic stability; and (3) no more than localized air close to the perforated diverticulum at CT scan [6]. However, if there is no clinical improvement within 48 hours, surgical intervention should be considered.
In cases of small bowel obstruction secondary to a localized perforation, non-operative management can be attempted (i.e., intravenous antibiotics, nothing by mouth, nasogastric tube decompression, fluid resuscitation, and possibly Gastrografin challenge) depending on the clinical status of the patient on arrival. In one of our cases, 21 hours after Gastrografin administration, there still was evidence of incomplete small bowel obstruction on abdominal radiography. Other situations such as intussusception, acute volvulus, or extrinsic bowel compression from a large fluid-filled diverticulum may require urgent surgical intervention [8].
Small bowel resection with primary anastomosis by open or a laparoscopy-assisted approach is the desired method. There have been cases of laparoscopy reported, but it may be technically difficult. In cases with a diagnostic dilemma, laparoscopy could be helpful, such as our case [5]. Either an end-to-end or side-to-side anastomosis by handsewing or staples is acceptable. Other approaches described are primary suture of the defect or diverticulectomy; these are not encouraged owing to their higher risk of death [6]. A mortality rate as high as 37.5% has been reported with primary closure of the defect [13]. The extent of resection or whether to include other uncomplicated diverticula is still debated. Currently, resection only of the affected diverticulum is recommended, as the risk of occurrence at other sites is unknown; but there is no evidence of a high risk of recurrence of jejunal diverticulitis.
For the uncomplicated cases, recurrence in the same diverticulum is rare; this problem usually occurs at other sites [2,6]. The incidence of recurrence may be underestimated because of the small numbers reported in the literature.
Conclusion
This study has demonstrated the challenges in diagnosing jejunal diverticulitis accurately on clinical grounds. Clearly, CT imaging remains the most reliable tool to aid in diagnosis and guide management. Nevertheless, the interpretation of CT imaging requires an experienced radiologist. The management algorithm based on our experience and review of the literature can help identify patients suitable for conservative management.
Author Disclosure Statement
The authors declare no competing financial interests.
Presented as an E-poster at the 17th Congress of the Asia Pacific Congress of Coloproctology, Kuala Lumpur, Malaysia, March 15–17, 2019.