
Abstract
Background:
Infection is a major cause of morbidity and mortality after heart transplantation (HT). Little information about its importance in the immediate post-operative period is available. The aim of this study was to analyze the characteristics, incidence, and outcomes of in-hospital post-operative infections after HT.
Methods:
We conducted an observational, single-center study based on 677 adults who underwent HT from 1991 to 2015 and who survived the surgical intervention. In-hospital post-operative infections were identified retrospectively according to the medical finding in the clinical records.
Results:
Over a mean hospital stay of 24.5 days, 239 patients (35.3%) developed 348 episodes of infection (2 episodes per 100 patient-days). The most common sources of infection were those related to invasive procedures (respiratory infections, 115 [33%]; urinary tract infections, 47 [13.5%]; bacteremia, 42 [12.1%]; surgical site infections, 25 [7.2%]), in addition to abdominal focus (33, 9.5%). Enterobacteriaceae (76, 21.8%) and gram-positive cocci (58, 16.7%) were the predominant germs, although opportunistic infections were not infrequent (69, 19.8%). Ninety-five septic episodes were detected with a mean Sequential Organ Failure Assessment Score of 9.5 ± 5.3 points, with hemodynamic failure being the most severe organ dysfunction and renal dysfunction the most frequent one. Management included broad-spectrum antibiotics in 48.8% of episodes and surgical management in 13.8%. The overall antimicrobial success rate was 96.3%. Higher in-hospital mortality was observed among infected patients (15.1% vs. 10.3%), but this difference was not statistically significant (p = 0.067). The one-year survival and events were not different between patients suffering from a post-operative infection and those who did not.
Conclusions:
In-hospital infections were frequent in the post-operative period after HT and were associated with a poor short-term outcome. Patients who survived sepsis had a similar one-year morbidity and mortality compared with patients who did not develop an infection.
In-hospital post-operative infections remain a major complication of healthcare, including after cardiac surgery. They occur in 5% to 21% of patients who undergo cardiac surgery and increase by more than five times the risk of post-operative death, the length of hospital stay, and the cost of care. The most common infections are those caused by bacteria related to invasive procedures such as surgical site infections, respiratory infections, catheter-related bacteremia, and urinary tract infections (UTIs) [1].
Heart transplantation (HT) patients constitute a particularly high-risk population because of previous advanced heart failure and immunosuppression. Infectious complications appear in 30%–60% of HT [2–4], leading to a death rate of 12%–17% in the first month and 29%–36% in the first year [5,6]. Although data on the epidemiology of post-surgical infections are limited, the available evidence suggests that early after transplant, health-care–related infections prevail, as has been described for general cardiac surgery patients, but it is not unusual for opportunistic infections to concur [7].
Because the local epidemiology would not be comparable to those on registries and the overall incidence and mortality of infection has been decreasing with changes in antibiotic prophylaxis, immunosuppression, and more effective treatment regimens [8], an investigation of local epidemiology and management might be required to detect problems and to typify the local microbiota resulting from particular pre-emptive measures and more accurate antibiotic treatment, which produce better probable outcomes although these benefits have not been assessed during the immediate perioperative period. The goal of this study was to determine the epidemiologic characteristics of in-hospital infections after HT and their effect on short- and long-term clinical outcomes.
Patients and Methods
Study description
We conducted a single-center retrospective cohort study including adult patients who underwent HT at the Complexo Hospitalario Universitario de A Coruña from the start of the program in April 1991 until December 31, 2015. Patients younger than 18 years or those with intra-operative death were excluded from the study.
Patients
Baseline demographic and clinical parameters reflecting the clinical status and comorbidities of the donor and recipient were collected, as well as conditions of the surgical procedure. Data were extracted from a prospectively maintained database (Advanced Heart Failure and Heart Transplantation Database, SIMON®, A. Coruña, Spain), completed by a comprehensive review of clinical records and critical care clinical information systems (CareVue® and ICIP®, Koninklijke Philips Electronics N.V. Amsterdam, The Netherlands). Patients were followed until time of death or cardiac re-transplantation. Otherwise, follow-up ended by December 31, 2016. The Regional Committee for Ethics in Clinical Investigation of A Coruña–Ferrol, Galicia, Spain, approved the study protocol.
Clinical protocol
The bicaval technique has been used routinely for HT surgery in our hospital since 1994. All patients undergoing the surgical procedure are admitted to the intensive care unit (ICU).
The immunosuppression regimen of all patients included induction therapy using muronab-CD3 until 2001 or basiliximab after 2001. Maintenance treatment includes a combination of steroids, a calcineurin inhibitor (cyclosporine A or tacrolimus), and an antiproliferative agent (azathioprine or mycophenolate mofetil). A mammalian target of rapamycin (mTOR) inhibitor (sirolimus or everolimus) was used instead of the calcineurin inhibitor or the antiproliferative agent when coronary allograft vasculopathy, severe renal failure, refractory rejection, or post-transplant malignancy were present beyond the first post-transplant year. Mycophenolate mofetil, tacrolimus, and m-TOR inhibitors were first used in our program in 1998, 2000, and 2005, respectively.
The perioperative infectious prophylaxis protocol included prophylaxes against opportunistic infections, the administration of antibiotic agents immediately prior to intervention for prevention of surgical site infections, and a mouthwash of chlorhexidine and nystatin for oral care. Surgical antimicrobial prophylaxis has not varied for some time. Intravenous cephazolin was administered to all patients who were not allergic to β-lactam class of antibiotic agents (2 g before surgery and 1 g every six hours after that over the next 24 hours) and intravenous vancomycin was prescribed in allergic recipients (1 g every 12 hours starting before surgery). Antibiotic treatment of those patients with a controlled infection at the time of transplantation was maintained as long as required by pre-operative infection.
Specific prophylactic treatment was not added if the spectrum of the ongoing regimen included the main germs causing surgical site infection. If the patient experienced clinical signs of active infection immediately after intervention, prophylaxis treatment was replaced by appropriate antimicrobial coverage. Broad-spectrum antibiotic prophylaxis (piperacillin-tazobactam plus vancomycin or linezolid) was occasionally prescribed in recipients admitted to the ICU for a long time before transplant, at the discretion of the intensive care medical staff.
All recipients received chemoprophylaxis against Pneumocystis jirovecii at least for the first 12 months after HT (trimethoprim/sulfamethoxazole 800/160 mg daily) and against cytomegalovirus (CMV) infection during the first month (oral valganciclovir 450–900 mg daily), extended up to the sixth month in seronegative recipients of a seropositive donor. If valganciclovir was interrupted after the first month, oral acyclovir (200 mg every eight hours) was maintained for the subsequent three months for the prevention of herpes simplex infection. To prevent pulmonary aspergillosis, oral itraconazole (200 mg daily) for the first three months after HT was prescribed routinely before 2004, however, inhaled amphotericin B (50 mg weekly) is currently the elective therapy for this goal. When a positive Mantoux test was detected before HT, oral isoniazid 600 mg daily was administered for 12 months after surgery for the prevention of tuberculosis. Heart transplant recipients with a negative pre-transplant serology against Toxoplasma gondii received oral pirimetamine (25 mg daily) for the first six months after HT.
Microbiologic diagnostic tests were included in the screening procedure when infection was suspected. Blood, urine, tracheal aspirate, and clinical-directed samples were analyzed routinely to identify etiologic germs, including nosocomial and opportunistic microbes. No routine surveillance cultures were performed. The management of infection included early broad-spectrum antibiotic therapy based on focus and patients' characteristics, followed by de-escalation as soon as possible, in addition to surgical management if required.
Parameters
The main end point of this study was the description of in-hospital infections after HT, defined as any clinically relevant infection occurring after transplantation and before the first hospital discharge. Infections were identified retrospectively according to the medical findings reflected in the clinical records and confirmed subsequently by two independent investigators. Discrepancies were resolved according to the consensus criteria of the Infectious Disease Society of America [9–11].
Opportunistic infection was defined as that caused by germs that do not cause illness except in patients with a weakened immune system. In our study, we considered opportunistic infections those caused by protozoa, fungi, herpes virus (primoinfection or reactivation), or opportunistic bacteria. Only primary bacteremia or catheter-related bacteremia were assigned a bacteremia diagnosis. Patients suffering from a secondary bacteremia were classified according to the source. An unknown foci infection was diagnosed when microbiologic tests had negative results, but high clinical suspicion remained. Surgical site infections were classified as site infection (superficial and deep) or organ/space (sternal instability and mediastinitis).
In addition to the causative agent and location, the associated organ dysfunction of each episode was investigated. Sepsis was considered if a life-threatening organ dysfunction caused by infection was present. Consistent with this, the severity was classified as sepsis, severe sepsis, or septic shock [12]. The maximum Sequential Organ Failure Assessment Score (SOFA) [13,14] was used to grade organ dysfunction.
In-hospital and one-year mortality were determined and considered as secondary end points. Differences in hospital stay, ICU stay, mechanical ventilation duration, and the incidence of short- and long-term complications such as rejection, ICU re-admission, post-HT non-scheduled admission, or graft dysfunction were also evaluated. Rejection was considered if a grade ≥3A (according to the International Society for Heart and Lung Transplantation classification) was detected in an endomyocardial biopsy or if there were clinical manifestations; graft dysfunction was considered when the left ventricular ejection fraction was lower than 55%. To analyze temporal trends in the incidence and type of in-hospital post-operative infection, the study cohort was divided in three groups according to the year of transplantation (1991–1999; 2000–2007; 2008–2015).
Statistical analysis
Qualitative parameters are expressed as proportion and quantitative parameters as mean and standard deviation. Categorical parameters were compared using a χ2 or Fisher exact test as appropriate. Quantitative variables were compared using a Student t-test. Kaplan-Meier plots and Cox regression were used to assess the survival probability and the cumulative incidence of in-hospital post-operative infection, where patients who were never infected were censored at the time of hospital discharge. A p value <0.05 was considered statistically significant. Analyses were carried out using SPSS software (IBM SPSS Statistics for Windows, version 19.0; IBM Corp., Armonk, NY) excluding incidence rate, which was calculated using Epidat software (Consellería de Sanidade, Xunta de Galicia released, in cooperation with OPS-OMS and CES University. Epidat: programa para el análisis epidemiológico de datos, version 4.2. July 2016).
Results
Population
Between April 1991 and December 31, 2015, 726 patients underwent HT at our center. Patients aged less than 18 years (n = 35) and patients who died intra-operatively (n = 14) were excluded from the analyses. Therefore, the surviving 677 patients comprised the study population. Their main baseline characteristics are described in Table 1.
Baseline Clinical Characteristics at the Time of Transplantation
INTERMACS = Interagency Registry for Mechanically Assisted Circulatory Support; ICU = intensive care unit.
The majority of patients was male (565; 83.5%). Coronary artery disease (280; 41.4%) and dilated cardiomyopathy (270; 40%) were the most frequent causes of heart disease leading to transplantation. Forty percent (n = 271) of the subjects were hospitalized at the time of HT; in 145 subjects (21.4%) HT was performed urgently. Pre-operative mechanical support with an intra-aortic balloon pump, mechanical circulatory devices, and mechanical ventilation were required in 123 (18.2%), 16 (2.3%) and 74 (10.9%) patients, respectively. Pre-operative Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profile 1 was present in 43 (6.4%) patients, INTERMACS profile 2 was present in 51 (7.5%) patients, and INTERMACS profile 3 was present in 107 (15.8%) patients. The remaining 476 (70.3%) patients showed a pre-operative INTERMACS profile 4 or higher. Pre-transplant recipient infection requiring active therapy was noted in 64 (9.5%) cases and donor infection was detected in 74 (10.9%).
Incidence of in-hospital post-operative infection
Over a mean in-hospital post-operative stay of 25.4 ± 37.3 days, corresponding to 17,196 days of follow-up from 677 HT recipients, 239 patients (35.3%) suffered at least one infection. Three hundred forty-eight episodes of infection were detected, among which 175 (50.3%) were diagnosed during the stay in the ICU and 173 (49.7%) were diagnosed during the stay in the surgical ward. One hundred seventy-four (25.7%) patients suffered one episode of infection, 33 (4.9%) suffered two episodes of infection, 20 (2.9%) suffered three episodes of infection, and 12 (1.8%) suffered four episodes of infection. The average number of infections per patient in the overall population was 0.52 ± 0.86 and for infected patients was 1.45 ± 0.85.
An incidence density rate of two episodes of infection per 100 patient-days of in-hospital post-operative stay was estimated (95% confidence interval [CI] 1.82–2.25). The incidence density rate during the ICU stay was 3.2 episodes per 100 patient-days (95% CI 2.76–3.69), whereas the incidence density rate during ward stay was 1.5 episodes per 100 patient-days (95% CI 1.27–1.71). Figure 1 represents a Kaplan-Meier estimation of the cumulative probability of in-hospital post-operative infection in the study population over time.

Cumulative probability of in-hospital postoperative infection among 677 heart transplant recipients who survived heart transplant intervention (Kaplan–Meier analysis).
The cumulative incidence of post-operative infection increased over time (1991–1999: 29.5%; 2000–2007: 39.6%; 2008–2015: 40.1%; p = 0.021). Figure 2 represents annualized infection rates, as related to changes in immunosuppressive protocols and transplant volume.
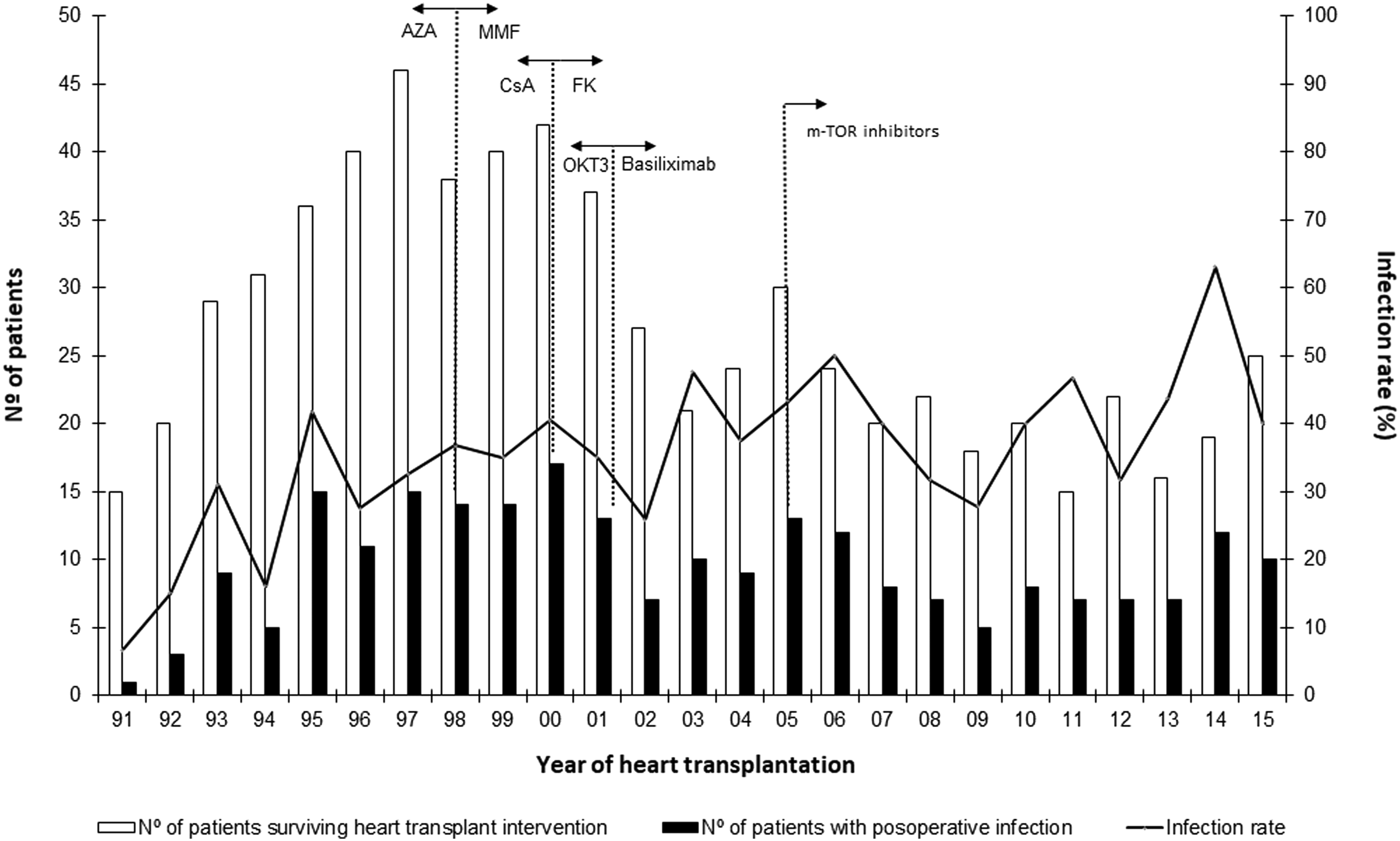
Temporal trends in number of infections and infection rates with regard to changes in immunosuppression. AZA = azathioprine; MMF = mycophenolate mophetil; CsA = cyclosporine A; FK = tacrolimus; OKT3 = muronab-CD3.
Site of infection
The most frequent sources observed were respiratory tract infection (n = 115; 33%), UTI (n = 47; 13.5%), bacteremia (n = 42; 12.4%), abdominal infection (n = 33; 9.5%) and surgical site infection (n = 25; 7.2%). Other foci were present in 51 patients (14.6%). Thirty-five episodes (10.1% of episodes) were considered unknown foci infections, clinically expressed as unknown foci fever (23 cases; 65.1%) or distributive shock of unknown origin (12 cases; 35.5%). Only six of these cases were diagnosed on the ward, five as result of an unknown foci fever over the first two days after ICU discharge and the others caused by septic shock causing late re-admission to the ICU. The distribution and temporal trend of major infectious sites over the study period is shown in Figure 3.
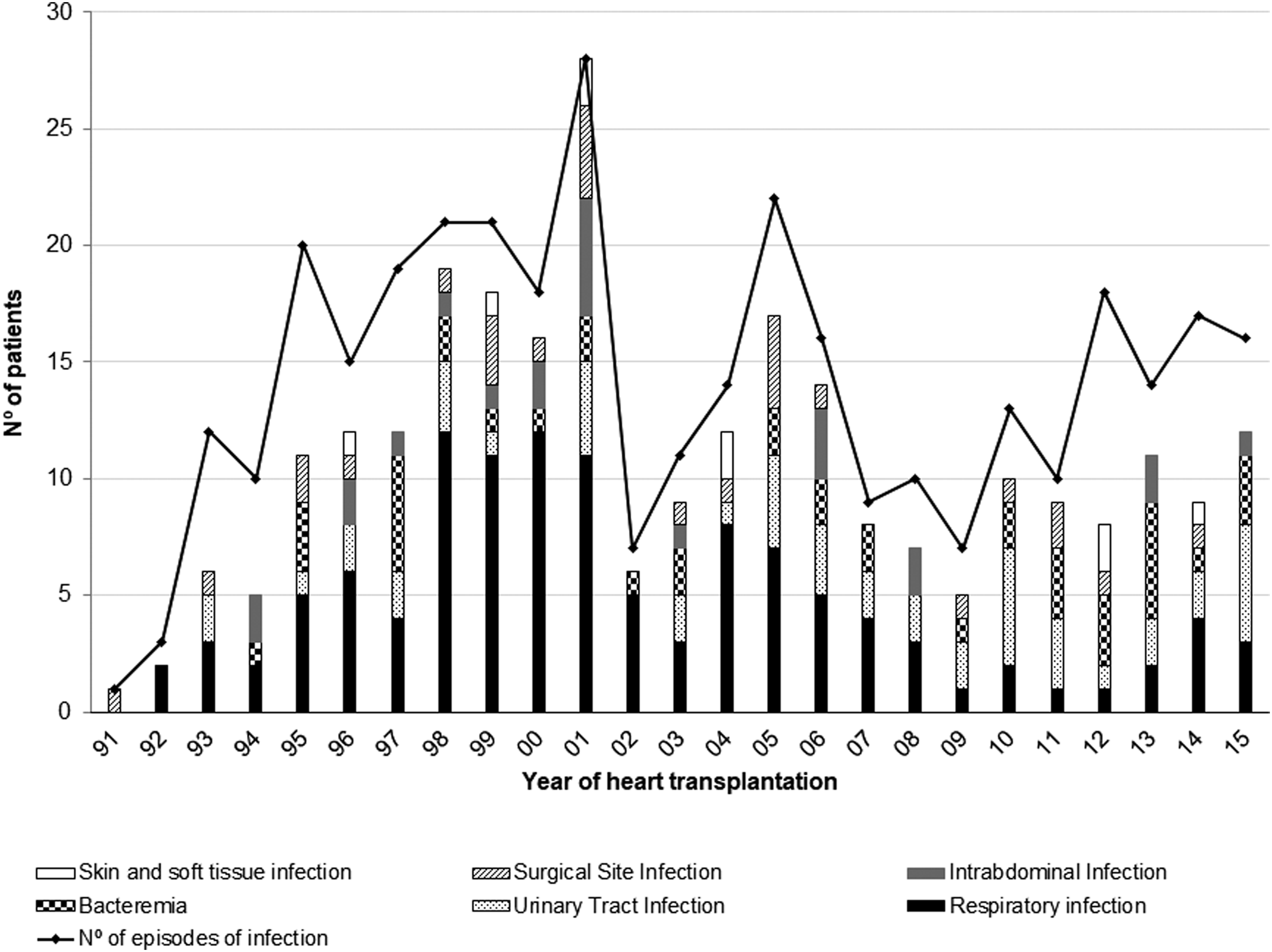
Temporal trends in number of episodes of in-hospital infection and the distribution among the most frequent sources.
Pathogens
Causal germs were detected in 225 episodes (64.6% of infections: 162 [46.5%] bacteria, 34 [9.8%] viruses, 23 [6.6%] fungi, and 6 [1.7%] protozoa). Enterobacteriaceae was the most frequent group (76; 21.8%), followed by gram-positive cocci (58; 16.7%). Polymicrobial infection was diagnosed in 16 cases (4.6%). A granular description of isolated germs according to infectious sites is provided in Table 2. Opportunistic germs were detected in 69 (19.8%) episodes of infection. Herpes virus (n = 33) and fungi (n = 23) prevailed, whereas bacteria (n = 6) and protozoa (n = 7) were less frequent.
Microbiologic Isolates of In-Hospital Post-Operative Infection by Source of Infection
Over each source of infection recount.
CMV = cytomegalovirus; CNS = coagulase-negative staphylococcus; HSV = herpes simplex virus; ICD = implantable cardioverter defibrillator.
Cytomegalovirus was the most prevalent opportunistic agent, causing 21 mononucleosis-like diseases (19 cases of reactivation and two cases of primoinfection), as well as eight cases of end-organ disease, including six cases of colitis (four reactivations, two primoinfections), one case of pneumonitis (reactivation) and one case of myocarditis (reactivation). Invasive pulmonary aspergillosis was diagnosed in 12 patients.
The temporal trend of the cumulative incidence of opportunistic infections over time is presented in Figure 4. No statistically significant differences of the cumulative incidence of this type of infections over time were detected (1991–1999: 9.8%; 2000–2007: 6.7%; 2008–2015: 13.3%; p = 0.089).
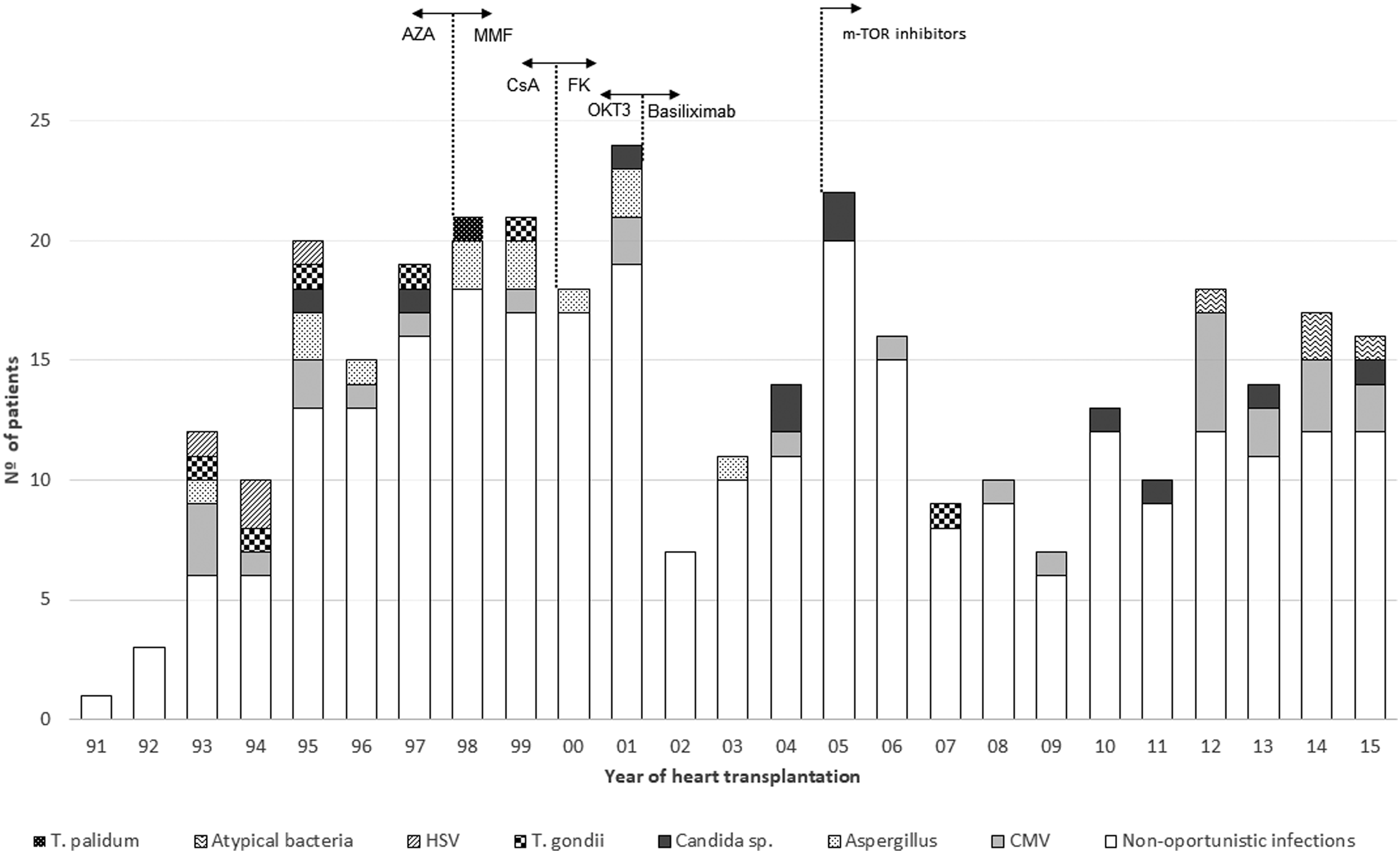
Evolution of in-hospital opportunistic infections over time regarding changes in immunosuppression. CMV = cytomegalovirus; HSV = Herpes Simplex Virus.
Severity of infection
Organ dysfunction was detected in 95 episodes of infection (27.3%; 26 [7.5%] severe sepsis and 69 [19.8%] septic shock) distributed among 75 patients. The mean SOFA score was 9.5 ± 5.3 points.
The incidence of organ dysfunction was 90.5%, 89.5%, 85.3%, 71.6%, 62.1%, and 47.4% for renal, respiratory, hemodynamic, hematologic, liver, and neurologic dysfunction, respectively. Severity, as assessed by the SOFA score, was 2.93 ± 1.56, 2.49 ± 1.48, 1.96 ± 1.11, 1.49 ± 1.23, 1.05 ± 1, and 0.77 ± 1.1 points for hemodynamic, renal, respiratory, hematologic, hepatic, and neurologic dysfunction, respectively.
Management of infection
All infections were treated with antimicrobial drugs, with a mean therapy duration of 15.2 ± 10.8 days. Empiric therapy was indicated in 270 infection episodes (77.6%), using broad-spectrum combination therapy in 239 (68.7%). Thirteen regimens (3.7%) failed, therefore broad-spectrum antibiotic coverage was needed. The mortality of patients needing an escalation of treatment was 33.3% (3/9), whereas that of patients with the correct treatment was 14.5 (p = 0.323).
In total, 143 (41.1%) infections were treated according to culture results (78 [22.4%] as starting therapy and 65 [8.7%] as de-escalation therapy). One hundred sixty-one infections (46.3%) were treated with a complete cycle of broad-spectrum antibiotic agents. Twenty-seven (18.5%) patients treated with broad-spectrum antibiotic therapy died, compared with nine (9.7%) of those whose antibiotic coverage could be restricted (p = 0.063).
Surgical intervention on the infective source was required in 48 episodes of infection (13.8%). Debridement for surgical site infections and skin and soft tissue infections was the most frequent intervention (22 procedures/33 infection episodes: 11 mediastinitis, five superficial wound infections, four fasciitis, and two pocket infections), followed by abdominal surgery (18 procedures/21 infection episodes: five cholecystectomies and 13 laparotomies for abscess drainage or intestinal resections due to ischemia or perforation). Less invasive approaches were also required (three venous lines replaced because of catheter-related bacteremia, three pleural drainages to control empyema, one pericardial drainage of an infective myocardial effusion, and one double J catheter insertion for an infected urinary obstruction).
Five (10.4%) patients died as a result of infection despite surgical management. Two patients required a second surgical procedure because of a new source of infection (peritonitis and later mediastinitis in one case; skin and soft tissue infection and later mediastinitis in other case).
Differences in mortality between patients who required surgical procedures to control the source of infection and those who did not were not statistically significant (21.7% vs. 13.5%, p = 0.158). No statistically significant differences in mortality were observed between patients treated surgically versus conservatively in the specific cases of mediastinitis (18.2% vs. 20%, p = 0.93) and peritonitis (25% vs. 33.3%, p = 0.82). Other types of infection that potentially could have been managed invasively or conservatively were not frequent enough to perform specific analyses.
Short-term clinical impact
Eighty-one patients (12%) in the overall cohort died during post-operative hospitalization after transplantation. Graft failure was the main cause of death (29 patients; 35.8% deaths). Infection was considered the main cause of death in 14 patients (17.5%) and a secondary relevant contributor to death in another 14 patients (17.5%).
No statistically significant difference regarding infection-related mortality was observed over time (1991–1999: 3.7%; 2000–2007: 6, 2%; 2008–2015: 1.9%, p = 0.102). The annual trend of infection-related mortality over time is represented in Figure 5.

Changes in all-causes and infection-related mortality over study period.
In-hospital post-operative mortality among patients who presented post-operative infection was 15.1% (n = 36), compared with 10.3% (n = 45) among patients without infection (p = 0.067). In-hospital post-operative mortality was especially high among patients who presented some specific types of high-risk in-hospital infections, such as sepsis with organ dysfunction (29/75; 38.7%), mediastinitis (4/16; 25%), bacteremia (10/43; 23.2%), respiratory tract infection (26/89; 22.6%), and Escherichia coli infection (9/41; 21.9%).
Invasive aspergillosis was the individual infection with a higher lethality rate in our series (7/12; 58.3%). All patients who suffered from this complication had received induction therapy, eight with muromonab-CD3 and 4 with basiliximab. Eight of 12 patients who developed invasive aspergillosis were receiving specific chemoprophylaxis with oral itraconazole.
The mean post-operative time on mechanical ventilation beyond 24 hours was higher among infected patients (8.2 ± 13.1 vs. 1.0 ± 2.3 days, p < 0.001). Both post-operative ICU stay (14 ± 17.9 vs. 4.9 ± 3.1 days, p < 0.001) and overall post-operative in-hospital stay (43.0 ± 57.6 vs. 15.7 ± 8.7 days, p < 0.001) were higher among patients who suffered at least one episode of post-operative infection.
The cumulative rate of re-admission to the ICU during the post-operative stay was 15.1% for patients with post-operative infection (n = 36), compared with 4.6% (n = 20) for patients without infections (p < 0.001). Infection was the major cause of re-admission to the ICU in five patients.
Pre-transplant infection
Overall, 271 (40%) recipients had been hospitalized for more than 24 hours before transplant surgery and 64 (9.5%) were being treated for an active infection. Pneumonia (n = 29), bacteremia (n = 10), and UTI (n = 7) were the most frequent pre-operative infections in these patients. Also, 13 patients were receiving empiric antibiotic therapy because of febrile syndrome of an unknown origin.
Thirty-six (56.3%) patients with pre-operative infection developed a new infectious episode after HT, but no reactivation of pre-operative infection was detected. Mortality rates of patients with or without pre-operative infection were not statistically different (10.9% vs. 12.1%, p = 0.80).
One-year clinical impact
Over the first year after transplantation, 104 patients (15.4%) died. The cumulative one-year mortality rate was 17.9% among patients with post-operative in-hospital infection and 13.9% among patients without it (p = 0.16). Figure 6 shows Kaplan-Meier one-year survival curves for both groups of individuals.

Clinical impact of in-hospital postoperative infection. One-year survival of 239 heart transplant recipients who suffered an in-hospital postoperative infection compared to 438 who did not (one-year Log rank test p = 0.262).
Overall, 587 patients required post-operative hospital admission after transplantation (203 patients with infection and 394 patients without infection). Over the first year of follow-up, 95 (46.8%) patients with post-operative in-hospital infection and 183 (46.4%) without infection required at least one unscheduled hospital admission (p = 0.9); ICU admission was required for 20 (9.8%) patients with infection and 40 (10.1%) patients without infection (p = 0.9).
Table 3 shows the cumulative incidence of relevant clinical outcomes one year after transplantation in patients who developed post-operative in-hospital infection compared with patients who did not. Graft dysfunction was diagnosed in 13 patients with infection and in 39 without (6.4% vs. 9.8%; p = 0.15) and graft vascular disease in seven and 23 patients, respectively (3.4% vs. 5.8%; p = 0.2). Statistically significant differences between the groups were noted for the cumulative incidence of acute rejection (53.5% vs. 65.1%; p = 0.014). However, after multivariable adjustment by age and sex of the recipient and tacrolimus, mycophenolate, and basiliximab use, this association was no longer statistically significant (p = 0.06).
Cumulative Incidence of Relevant Clinical Events at One-Year of Follow-Up after Transplantation
ICU = intensive care unit.
Discussion
This single-center, observational retrospective study of 677 consecutive adult heart transplant recipients showed a cumulative incidence rate of in-hospital post-operative infection of 35.3% and a daily incidence density rate of 2%. These results indicate that in-hospital post-operative infection is a frequent complication after HT. Previous studies have shown a varying incidence rate from 22%–70% [2–4]. Differences in the population's characteristics and management, diagnostic criteria, or surveyed timeline could explain the differences among the surveys.
Whereas infective episodes diagnosed in the ICU were only slightly higher in number than those diagnosed during the ward stay, the cumulative incidence of ICU episodes was almost three times higher than that of ward episodes. The timing of post-operative infectious episodes suggests, in general terms, an early onset after transplantation, probably related to the start of immunosuppression, critical clinical state, and invasiveness. Furthermore, in our series, the respiratory tract was the most frequent infection site, followed by UTI, bacteremia, and surgical site infections, supporting the hypothesis that handling is a major source of infection in these patients. In prior studies, the distribution of infection sites was analyzed irregularly [2–4,7,8,15–22], however, in general terms, published data are concordant with our findings. These data together led us to argue that prevention, surveillance, and acting on suspicion of infection, especially in the early post-operative period, could be crucial factors for these patients, and also highlights the importance of asepsis, antibiotic prophylaxis of surgical infections, and preventive programs of nosocomial infections [23] (e.g., bacteremia [24], pneumonia [25], or ITU Zero [26]) as a part of the clinical protocol.
The cumulative incidence of in-hospital post-operative bacteremia was 6.3%, which is lower than previously published (10%–28%) [15,16,27–29]. It should be noted that in our study, only patients who had primary bacteremia were classified in this category, and infectious episodes involving hematogenous dissemination from a local source were classified according to the primary site.
Despite being rarely assessed in previous reports [30–32], attention should be paid to abdominal infections. This study shows a substantial number of abdominal infections after HT, ranking the fourth most common site of infection. Although the observed cumulative incidence of cholecystitis was comparable to that prior to the HT series, bowel perforation was the main gastrointestinal complication. Because no diverticulitis was detected, ischemia became difficult to manage. It is well known that both gallbladder and intestinal malperfusion during cardiac surgical procedures are related to poor splanchnic blood flow or oxygen supply, mainly secondary to blood redistribution during cardiopulmonary bypass, shock, or hypoxia. Hypoperfusion is particularly frequent in congestive patients with a New York Heart Associate (NYHA) stage IV, poor left ventricular function, emergent surgery, re-operation, or multiple blood transfusions, which could explain why the HT population is particularly prone to these complications, but it cannot justify the higher incidence in this study. Further analyses of patient characteristics, cardiopulmonary bypass conditions, and their post-operative management are imperative to identify areas for improvement.
Infectious colitis is not often analyzed in similar surveys. Most cases in this study were caused by early CMV infection, but a few cases were also noted in early citations [2–4,16–18,32,33]. Clostridium difficile diarrhea was not as frequent as previously reported [34], which could be explained by the restrictive antibiotic protocol and routine early enteral feeding approach.
In addition to CMV colitis, post-operative opportunistic infections were relatively frequent in our report and have also been reported in similar studies [7]. Cytomegalovirus is the prevailing microbe of this group and is the systemic infection of major clinical manifestation, followed by colitis, pneumonia, and myocarditis, similar to the patterns found in previous reports [2–4,16–18,32,33]. Nevertheless, the overall incidence and mortality rate are low compared with those in previous reports, which can be explained by the strict chemoprophylaxis protocol. Cases of unknown foci infection and colitis without an isolated germ should be considered when dealing with this subject. Historical reports and limitations of diagnostic tests in the early era of this cohort could have led to an underestimation of the number of cases.
Aspergillosis was the most frequent fungal post-operative infection in this study. Although its overall cumulative incidence was low (1.7%), its early mortality was especially high in our patients, who presented pulmonary invasive disease. It should be noted that most of cases occurred before 2001, when muromonab-CD3 was switched to basiliximab as induction therapy, and all cases happened before 2004, at which time amphotericin was incorporated into the clinical protocol instead of itraconazole. This could reflect the important impact of immunosuppression and this prophylaxis on the outcome of our patients [35], even though the mortality rates according to induction therapy observed in our series differs from previous reports [36,37]. These differences could be caused by the small number of patients with aspergillosis or other potential confounders, such as drug interactions or absorption abnormalities involving itraconazole, not titratable in our series because determination of the level of drugs different from tacrolimus has not been routinely available candidiasis was scarce in this research. Previous articles indicate blood stream and surgical site infections as leading sources for this germ, however, in our institution, fungemia and fungal mediastinitis were rarely detected, instead peritonitis and mild infections such as candiduria were the most usual problems caused by yeast [2]. The use of nystatin as part of oropharyngeal hygiene routine and the restrictive antibiotic protocol could be related to these findings.
Bacteria, particularly nosocomial bacteria, are the predominant germs in surveys dealing with in-hospital post-operative infections after HT, and different species are highlighted according to the local flora of each hospital and the study design [2–4,15–22]. In accordance with these studies, gram-negative bacilli (mainly Enterobacteriaceae) and gram-positive cocci prevailed in our center, even though small differences should be considered when selecting the optimal empiric antimicrobial therapy in this institution. Acinetobacter was anecdotal, therefore, concern about nosocomial non-fermenting gram-negative bacilli should be directed to the control of Pseudomonas aeruginosa (20% of infections caused by gram-negative bacilli). Escherichia coli was confirmed as the main Enterobacteriaceae, however, it was associated with a higher risk of mortality in the present study (21.9%) than in previous studies [4]. Factors influencing this, such as antimicrobial resistance or involved serotypes, were not assessed in this survey, therefore, they should be considered in further investigations in order to judge what the underlying problem is and how it can be treated.
Gram-positive cocci remain a main cause of infection, especially when pneumonia, bacteremia, and surgical site infections are reviewed. Systematic nasal decontamination might explain the difference in the proportion of Staphylococcus aureus in this report and the published literature, in which coagulase-negative staphylococcus and enterococci infection prevail [2–4,27–29].
Nearly one-third of our infected patients developed sepsis. Hemodynamic failure was the most severe organ dysfunction, probably related to the intrinsic susceptibility of the cardiovascular system of HT patients, and prevailed over other organ dysfunctions, except for renal and respiratory dysfunction. The subsequent in-hospital outcome was poorer (38.7% vs. 8.6%; p < 001) and required a longer hospital stay and life support. Candel et al. [29] described a septic shock incidence of 14% among patients suffering from bacteremia after solid organ transplantation, with a mortality rate of 54.5%. Nevertheless, comparison with our results would not be appropriate because the population study included only bacteremia and only one HT patient. Similarly, using non-transplanted critically ill patients as a point of reference would not be appropriate because a different survival based on the inherent regulation of the immune response by immunosuppression has been observed [38]. The outcome of the septic transplant cohort of the latter study is comparable to that of our sample.
Few reports commenting on the management of in-hospital post-operative infections in HT have been published [29,38,39]. They agree with general sepsis studies on the higher risk of mortality if inappropriate antibiotic coverage is administered or if surgical source control is not used. Our post-operative antibiotic protocol recommending early broad-spectrum antibiotic agents followed by de-escalation as soon as possible explains the high success rate (96.3%) at our institution. Some authors warn of the risk of developing more side-effects when a combination of second-line antimicrobial agents is prescribed, worsening the prognosis of the graft and the patient [39], however, that was not observed in our population.
Surgical management formed the basis of the treatment of surgical site and abdominal infections. The rates of these sources, rate of mortality, and the proportion of cases managed conservatively was similar to those described previously [23,40–43]. No differences were found comparing the mortality of patients treated with a surgical approach to those managed conservatively, although the small sample size and the subjective indication of surgery limits the interpretation of these results.
The difference in one-year events was analyzed between patients suffering from in-hospital post-operative infections and those who did not. Graft function, often affected acutely by septic myocardial dysfunction, was in the normal range one year later in both groups. Vascular graft disease, proposed to be related to CMV infection, was a rare circumstance at the one-year follow-up and no difference between the two groups was observed.
Differences in rejection episodes were detected in a univariable analysis at the time of estimating the one-year outcome. This relation was not found when a multivariable analysis was conducted adjusting for age, sex, and immunosuppression, suggesting differences in treatment affected the retrospective observational character of the study.
Infection is described as a risk factor for death in HT patients [2–8,15–22,27–31]. In our study, differences in hospital survival were observed but not statistically significant. The sample size, high volume of non-septic patients, aggressive sepsis resuscitation, and antimicrobial management could explain the differences between our study and reports from registries and other centers. The comparison among the three time periods in our cohort shows that the incidence of this kind of infections is increasing regardless of changes in immunosuppression, without a substantial impact on overall and infection-related mortality rates. This fact contradicts the results of studies focused on overall infections (not only in-hospital episodes) that expose a reduction of the incidence and mortality of infections over time related to changes in immunosuppression [8]. This difference is reasonable because factors influencing in-hospital infections go beyond immunosuppressants and those factors suffer a simultaneous increment in our series [44]. Once discharged from hospital, the one-year risk of death was no different between patient with or without in-hospital post-operative infection, suggesting that once early post-operative complications have been overcome, they do not have an impact on the future transplant status.
This study has limitations intrinsic to a retrospective single-center design. The relevant findings, such as those of the impact of Escherichia coli or abdominal infections, are only suggestive of potential problems, therefore proper studies are needed in order to find solutions. The extrapolation of these results is difficult because the infection criteria applied was based on reports and microbiota and protocols of care that are highly dependent on each center. Furthermore, the wide period of the study includes different eras of immunosuppression, infectious chemoprophylaxis, and post-operative and infection management, resulting in a heterogeneous sample that could lead to confusing results such as the one described regarding rejection. Moreover, some aspects of infections were not analyzed, such as antibiotic resistance or the tax of bacteremia related to primary foci. Finally, risk factors for infections were not assessed in this article.
In conclusion, in-hospital post-operative infection after HT is a frequent complication, affecting more than one-third of patients and having poor short-term outcomes. Episodes secondary to invasive treatments are predominant, although opportunistic infections are not rare. Patients who survive sepsis have a similar one-year morbidity and mortality to patients who did not suffer a post-operative infection.
Footnotes
Acknowledgments
We would like to give a special thanks to the intensive care unit staff, in particular Dr. Salvador Fojón, and to those involved in the care of heart transplant recipients and donors.
Some of the authors of this article are part of the CIBERCV (Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares), Instituto de Salud Carlos III, España.
Funding Information
This work was partially co-financed by FEDER Funds.
Author Disclosure Statement
The authors declare there are no competing financial interests.