
Abstract
Background:
Surgical site infection is a common cause of post-operative morbidity. Although a number of studies on negative pressure dressings including PICOTM (Smith & Nephew, St. Petersburg, PL) have shown reduced rates of surgical site infections (SSI), more evidence is required. This study sought to determine if PICO dressings reduce surgical site infections or other surgical site complications in primarily closed laparotomy incisions after clean-contaminated surgery in moderate-risk patients.
Methods:
Patients undergoing laparotomy and bowel resection were randomly assigned to PICO or conventional dressings. The incision was assessed one-week post-operatively for any infection. Patient notes including outpatient appointments were later examined for any delayed infection during the same or subsequent admissions or in the outpatient setting. Patient characteristics such as body mass index (BMI), incision depth, and comorbidities were noted to identify any group who may show more benefit from the negative pressure dressings.
Results:
From March 1, 2015 until September 30, 2017, 217 patients consented to participate in the trial. Twenty-nine were subsequently excluded, leaving 188 patients with 96 receiving PICO and 92 receiving a standard dressing. Twenty-seven (14%) patients developed a surgical site infection; 13 received a PICO dressing and 14 received standard dressing (p = 0.73), indicating no difference in surgical site infections between the two types of dressing (odds ratio [OR] 1.1). Thirty-one (16.5%) patients developed other surgical site complications. Eleven of these patients received a PICO dressing and 20 received the standard dressing (p = 0.06, OR 2.1).
Conclusion:
This study does not support the routine use of PICO dressings on uncomplicated laparotomy incisions in moderate-risk patients.
Incision healing and incision complications are an important and costly aspect of surgical care. Rates of surgical site infection (SSI) generally vary in the literature from 1%–11% of surgical patients [1–4] but can be as high as 25% in higher risk patients such as those undergoing colorectal and other abdominal surgeries [5–7]. Although SSIs tend not to be as morbid as other hospital-associated infections, SSI is the most common type and therefore incurs the most substantial costs [1,8]. These costs include a doubling (or more) of the cost of inpatient care [1,2,9,10] because of doubling of the length of stay [4], up to five times higher rates of re-admission to hospital [2], intensive care admissions, and unplanned returns to the operating room. Patients with SSIs are also twice as likely to die [2]. Other costs include reduced productivity (for the patient and family members), temporary or permanent loss of function, and impaired mental health and quality of life. In the case of oncologic surgery, adjuvant treatments may be delayed and therefore reduced in efficacy.
Most SSIs occur within three weeks of surgery, however, any infection within 30 days, is considered to be an SSI [1]. They are classified as superficial (skin/subcutaneous tissue) or deep (fascia or muscle) [1,11].
A multitude of risk factors have been linked to SSIs. These may be caused by unmodifiable risk factors either related to the patient such as obesity and smoking or to the disease, for example, bowel perforation. Other risk factors are modifiable, such as incision size or type of skin preparation [3,12,13] . Many strategies have been utilized to minimize these risk factors [1,9,14,15]. One of these strategies is the choice of dressings on the surgical site.
There is a range of incision dressings available, all with theoretical benefits, but a lack of definitive evidence to support the choice of any particular dressing, or even whether a dressing is better than no dressing at all. A Cochrane Review of studies on incision dressings and their effect on SSI rates found insufficient evidence to draw any conclusions as to whether dressing choice has an effect on SSIs [16]. This meta-analysis mainly looked at passive dressings, which are designed mainly to protect the incision from contamination with basic moisture absorbance to keep the incision dry. Negative pressure dressings aim to allow moist incision healing while actively absorbing moisture, potentially reducing seroma, maceration, and excess exudate with subsequent bacterial overgrowth [17]. It is also theorized that the strain of sub-atmospheric pressure promotes cellular proliferation by promoting cellular deformation [18].
PICOTM (Smith & Nephew, St. Petersburg, FL) is a negative pressure dressing that is lightweight and designed to be left in place for seven days, making it lower maintenance and easier to carry around than standard negative pressure dressings. This has made it increasingly popular for prophylactic use on surgical incisions, despite greater cost than a standard dressing.
A number of studies have examined the effect of negative pressure dressings on rates of incision complications. These include a number of randomized controlled trials (RCTs), some showing a trend [19,20] or a statistically significant benefit in negative pressure dressings [21–23]. There have also been a number of retrospective and cohort studies published, with mostly positive [24–30] but some negative findings [31].
Meta-analyses have shown possible benefits to negative pressure in infected incisions [32] and chronic wounds [33], as well as on clean wounds and closed incisions [34–37]. However, many of the studies included in these meta-analyses are not RCTs, and therefore subject to the inherent biases in other types of study design. A Cochrane Review of negative pressure dressings concluded that the benefits of negative pressure dressings are uncertain, and more research is required [38].
Negative pressure dressings are more expensive, however, a reduction in incision complications with reduced length of stay and re-admissions as well as improved quality of life may balance that cost. A pilot RCT [21] with cost-benefit analysis showed greater monetary cost but better quality of life scores in the patients treated with PICO dressings.
Aim
Our goal was to determine if there is any reduction in infections in laparotomy incisions after clean-contaminated surgery in moderate-risk patients by using negative pressure dressings, specifically PICO system, as a prophylactic measure on primarily closed incisions.
Methods
This was an RCT. The trial was approved by the Monash Health Human Research Ethics Committee.
Power calculations
Estimated SSI of 20% with conventional dressings, based on SSI rates in colorectal patients in the literature and SSI rates reported previously in our institution. Estimated SSI of 5% with the PICOTM dressing, as this would constitute a clinically significant risk reduction. Aiming for power of 80%, alpha 0.05 with estimated effect size 15%, the number of patients required per arm was 88 patients.
Inclusion criteria
Patients were included if they were adult patients undergoing laparotomy for at least clean/contaminated surgery and those patients at moderate to high risk for SSI, with one or more of the following risk factors: overweight or obese (body mass index [BMI] >25); diabetes; contaminated surgery (perforation or abscess); non-elective (subacute) clean/contaminated surgery; and incision primarily closed. Patients were excluded if they underwent mini-laparotomy or relook surgery or were pregnant.
Clinical management
Pre-operative preparation included shaving as required, povidone iodine skin preparation (chlorhexidine/alcohol for iodine allergy), and prophylactic antibiotic agents. Patients were randomized in blocks, with pre-prepared randomization envelopes opened at the time of consent. Most patients were recruited pre-operatively but as a result of slow recruitment, a small number of patients undergoing laparoscopic surgery that was converted to an open procedure were recruited in the first 24 hours post-operatively, and any such patient randomly assigned to the PICO dressing would undergo a change of dressing at that time.
Dressings remained in situ for seven days, or until the day of discharge if they went home earlier, unless there was suspicion of infection or the dressing was soaked or leaking. The incision was assessed for infection or other complications at this time. Patient records, including outpatient clinic notes, were inspected for any later infections. Patients were also sent a questionnaire to detect any cases in which infection was managed outside of the original hospital.
Primary end point: Incision infection
Incision infection was defined according to VICNISS definitions [11] of superficial (skin and subcutaneous tissue) and deep (fascia and/or muscle) incisional or organ/space infection (VICNISS is the major healthcare infection surveillance organization for Victoria, which is based on a model from the U.S. Centers for Disease Control and Prevention, and widely used and published).
Secondary end point
Possible risk factors associated with incision breakdown such as incision length, thickness (at its thickest from fascia to skin, in millimeters), height and weight (and BMI), and comorbidities including diabetes.
Statistical analysis
Continuous data were tested for normality of distribution and summarized as means with standard deviations (± SD) or medians with interquartile range (interquartile range [IQR}; 25th–75th percentile). When comparing means or medians we used the Student t-test or Mann–Whitney U test, respectively. Categorical variables were summarized as participant numbers and percentages, and when comparing between groups we used the χ2 test. The binary logistic regression model was used to examine the association treatment type and the risk of incision complications and post-operative infections. Univariable analysis was conducted to assess the main effects. Age, gender, and BMI were forced into all multivariable models because they were considered clinically significant a priori. Subgroup analysis was performed to evaluate the efficacy of the treatment method on gender, BMI category, age category, incision depth, diabetes status, insulin, major comorbidities, and incision complications and the results are delineated in forest plots. Statistical analyses were performed using Stata software, version 14.2 (StataCorp, College Station, TX) and level of significance set at 5%.
Results
From March 1, 2015 until September 30, 2017, 217 patients consented to participate in the trial. Twenty-nine were subsequently excluded for a variety of reasons (withdrawal of consent, cancellation of surgery, different/ineligible surgery performed, major breach of trial protocol, e.g., wrong dressing applied in the operating room). Ultimately 188 patients were included. Ninety-six received the PICO dressing and 92 the standard dressing (Fig. 1).
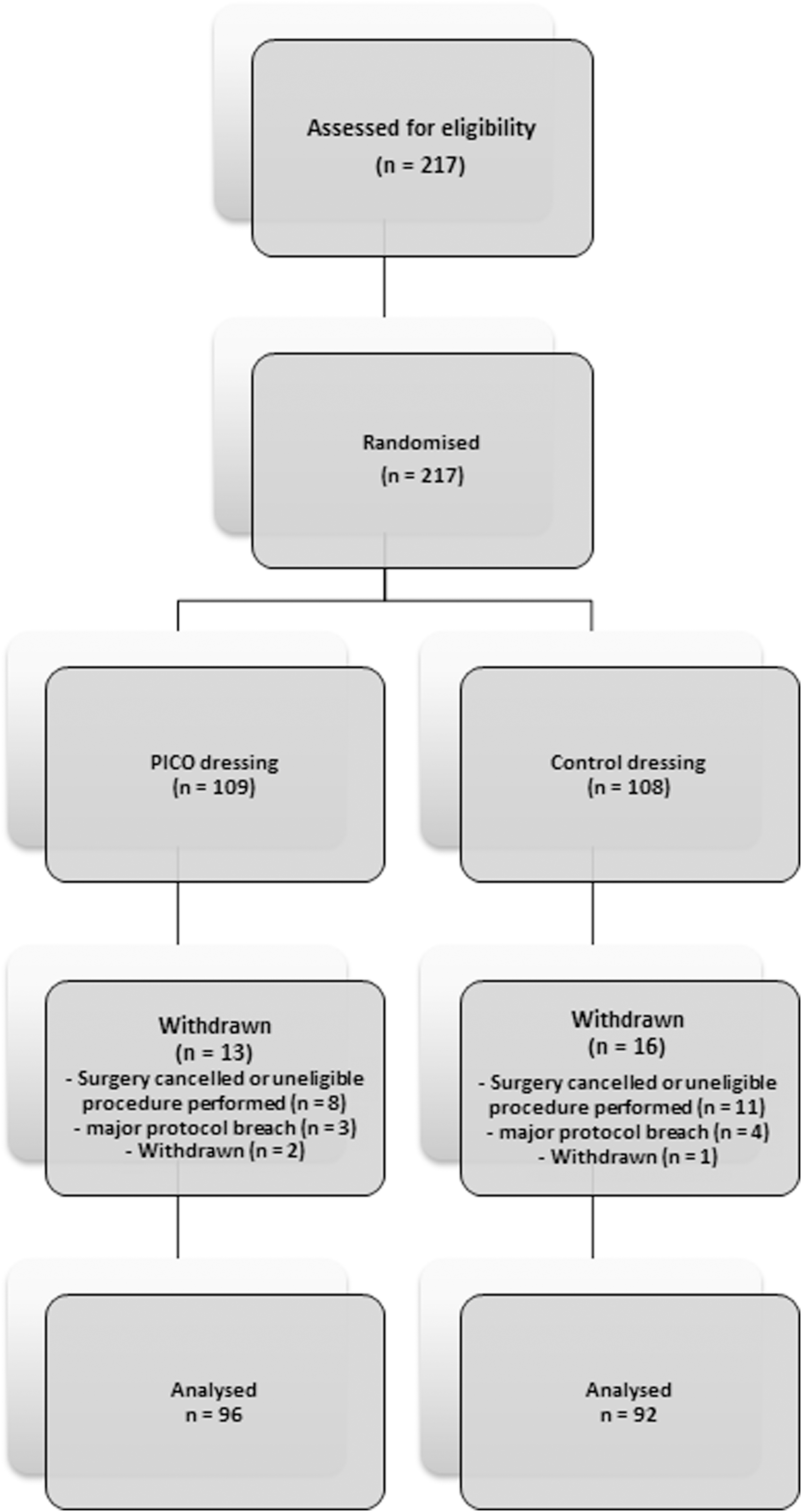
Study design.
There were no substantial differences in the demographics, incision depth, or comorbidities between patients receiving PICO or the control dressing (Table 1). All patient underwent clean/contaminated surgery. The majority underwent colorectal procedures, with seven patients having small bowel resections (Table 2) and more than half of these were bowel cancer resections (Table 3). Most were elective procedures (Table 4), however, 43 patients were subacute. Subacute was defined as patients who were admitted acutely and required same-admission (but not immediate) surgery, usually in the next few days, when an in-hours operating room was available. This was largely because we lacked the resources to identify, recruit, and randomize potential candidates after hours and to a reluctance of the ethics committee to allow acutely unwell patients to be recruited. Patients who were initially planned for laparoscopic surgery and left colon/anterior resections received mechanical bowel preparation. Patients received prophylactic antibiotics at induction of surgery. One to two grams of intravenous cephazolin was used for the majority (all but 15 cases).
Patient Characteristics
SD = standard deviation; BMI = body mass index; IQR = interquartile range.
Wilcoxon-Mann-Whitney test was conducted to derive the p value.
Types of Surgery
Part of bowel resected or operated on.
Colostomy with no resection.
Diagnoses
Level of Urgency
Non-elective admission requiring same admission surgery, but not within first 24 h.
Of the 49 patients with diabetes, 27 received PICO and 22 standard dressings. The average hemoglobin A1C was not substantially different between the two groups (7.9 vs. 7.6). Rates of incision infection and other complications (hematoma or blistering, non-infected incision collection, skin dehiscence, hernia) were compared between the two groups (Tables 5 and 6).
Rates of Incision Complications
Main Effects
OR = odds ratio; aOR = adjusted odds ratio.
Adjusted for age, gender, and body mass index (BMI).
Twenty-seven (14%) patients developed an incision infection; 13 received a PICO dressing and 14 received the standard dressing (p = 0.73), indicating no substantial difference in incision infections between the two types of dressing, with odds ratio of 1.1. Management of incision infections in summarized in Table 7.
Management of Incision Infections
Thirty-one (16.5%) patients developed other incision complications, the most common complication being skin dehiscence (Table 8). Eleven of these patients received a PICO dressing and 20 the standard dressing (p = 0.06), with odds ratio of 2.1 in favor of the PICO dressing.
Incision Complications
Further analysis was performed to detect any differences in infection rates between subgroups such as gender, BMI, age, incision depth, diabetes, and comorbidities, all of which showed insignificant differences, and no meaningful trends to identify a group that may benefit more from the PICO dressing in terms of reduced incision infections or other incision complications (Fig. 2 and 3).
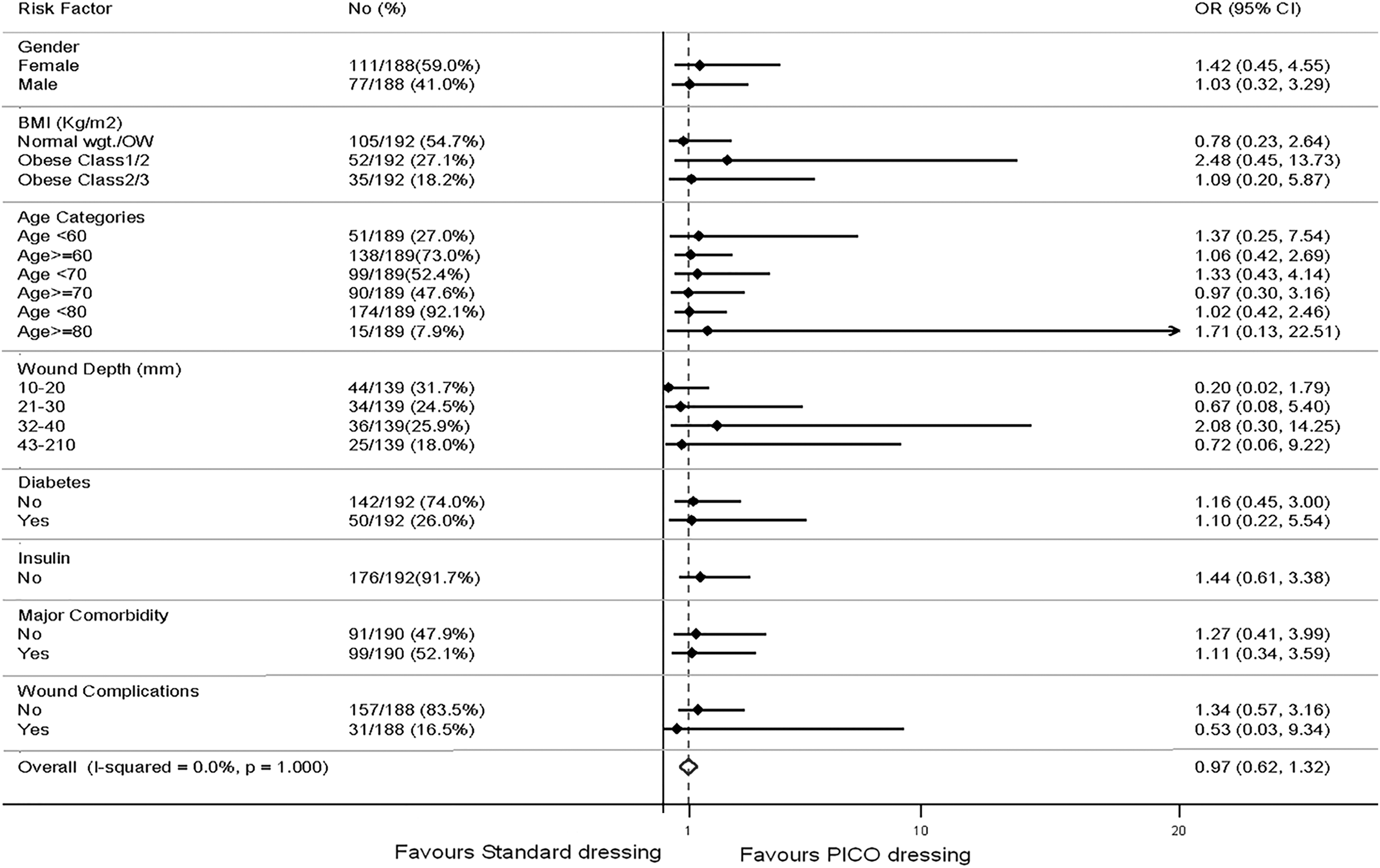
Analysis of post-operative wound infections and dressing type by patient risk factors.
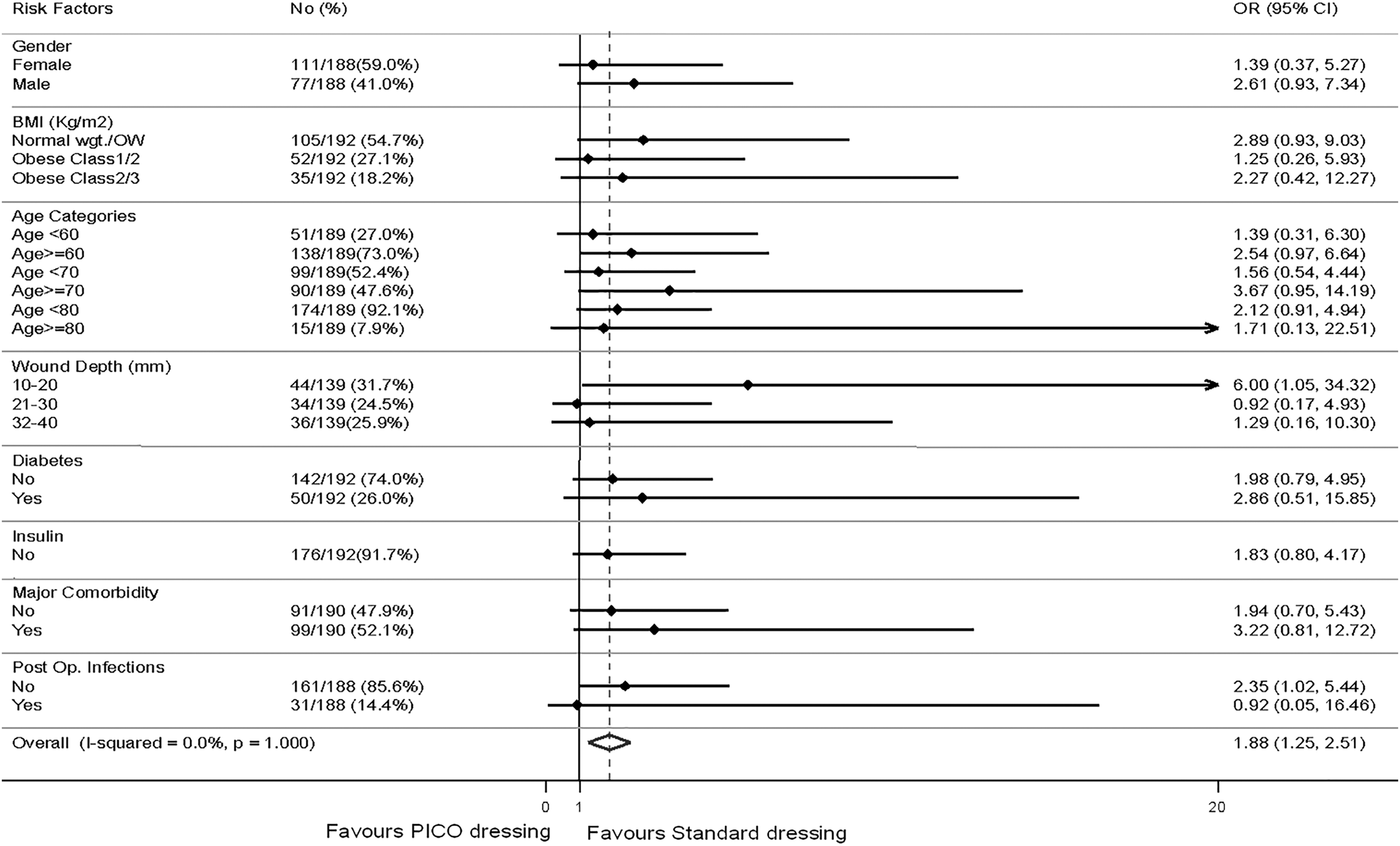
Analysis of post-operative incision complications and dressing type by patient risk factors.
Limitations
Power calculations were based on infection rates of 20% and the overall infection rate was only 15%. It is therefore possible that the sample size was not adequate to detect a significant difference. However, because there was not even a trend to reduced infections with the PICO dressing, it would seem unlikely that a larger sample will show anything more significant.
This trial was initially intended to include both acute and elective cases. However, we soon found that we were under-resourced to identify and recruit acute cases adequately, and as such only a small number of such patients were included. This increased the heterogeneity of the sample without being a large enough part of the sample to extrapolate our results to this category of patient.
The study was not blinded; patients obviously could not be blinded, and the small research team meant the recruitment and post-operative assessment were often performed by the same people. As a result, there is a possibility for bias in the post-operative incision assessment. In the majority of cases, the diagnosis of incision infection was made or confirmed by the treating clinician, who was not involved directly in the trial but also not blinded.
Because patients were assessed by the research team post-operatively and discharge summaries were reviewed after more prolonged admissions, identification of in-hospital SSI was accurate. However, infections after discharge may have been missed; notes from the hospital outpatient appointments and most of the reviews taking place in the surgeons' private offices were able to be reviewed, but patients treated by other hosptials or their general practitioner may not have been picked up. The questionnaire sent to all patients to try to pick up on any post-discharge events did identify a small number of additional SSIs or other complications, however, the questionnaire response rate was poor (19%).
Discussion
This RCT sought to compare the rates of incision infection in closed laparotomy incisions in patients receiving PICO dressings versus a standard passive dressing. Secondary goals were to detect any subgroup such as the obese, those with deeper incisions, or comorbidities, who may show more benefit from a particular dressing and to detect any relation between dressing type and other incision complications such as skin dehiscence or hernia.
With regard to the primary end point, i.e., incision infections, no difference was seen between the dressing types, suggesting that the use of the more costly PICOTM dressing in this type of moderate-risk patient (diabetic or overweight or obese patients undergoing elective, clean-contaminated colorectal surgery) is not warranted. The finding of a reduced rate of incision complications in PICO patients was not significant and difficult to interpret given the heterogeneity of complications in this group and questionable clinical significance of some of these complications. Subgroup analysis also failed to show any significant benefits according to gender, BMI, age, wound depth, or comorbidities, however the study was not powered to detect a difference in these subcategories. Further research could be directed to higher risk categories of patients, however, this would likely need to take place in a higher volume center or as a multi-center trial in order to recruit adequate numbers in a timely fashion.
Conclusion
This study does not support the routine use of PICO dressings on uncomplicated laparotomy incisions in moderate-risk patients. Given the volume of research that has suggested benefits from negative pressure dressings including PICO, there may be a place for further research to define more clearly which patients will benefit most from negative pressure dressings.
Footnotes
Acknowledgments
We acknowledge Mr. Brian Hodgkins for critiquing the paper prior to submission for publication.
Funding Information
This trial was funded by Smith and Nephew, the company that produces the PICO dressing. Smith and Nephew received ongoing updates of all findings but did not have any active input or editorial power over the study protocol, day-to-day running of the trial or reporting of findings.
Author Disclosure Statement
Several of the authors (K.L., L.C., K.L.) received some financial payment from the trial budget to cover additional hours worked as a part of the study.
The study statistician (S.R.) is a paid employee of the School of Public Health and Preventive Medicine, Monash University who also received payment for the statistical analysis, which was received via the trial investigators, with no direct contact with the sponsors.