
Abstract
Background:
The reported rate of surgical site infection (SSI) in breast surgery is often higher than expected. Using antibiotic prophylaxis to reduce SSI is debatable because of the risk of developing bacteria resistance and the cost burden. In this study, we evaluated the effectiveness of antibiotic prophylaxis in breast surgery and the factors predisposing patients to SSI.
Methods:
A retrospective–prospective (ambispective) study was conducted in the Department of Breast Surgery, Qilu Hospital, P.R. China. The retrospective antibiotic-using group was composed of patients found to have breast cancer between January 2008 and October 2010. The prospective non-antibiotic-using group was composed of patients identified between November 2010 and November 2013. Pre-operative, peri-operative, and post-operative clinical data were analyzed.
Results:
The SSI rate of the non-prophylaxis and prophylaxis groups was 1.1% (11/1,022) and 1.2% (12/1,034), respectively. Neoadjuvant chemotherapy was related to SSI in the non-prophylaxis group (p = 0.026). Staphylococcus aureus was the predominant microorganism responsible for SSI, without obvious resistance to a widely used first-generation cephalosporin.
Conclusions:
Peri-operative antibiotic prophylaxis is of no significant value in preventing SSI in breast cancer surgery. Our results indicated that neoadjuvant chemotherapy might be a risk factor doe SSI, but further research is needed because of the sample size disparity between infected and uninfected groups.
Breast cancer ranks in the first place in both morbidity and mortality rates among women in China [1,2]. Mastectomy has been accepted widely and is a routine surgical procedure for patients with a malignant tumor.
As is the case with other operations, post-surgical infections lead to poor consequences. Apart from various common defects [3], surgical site infection (SSI) [4] after breast operations causes more severe consequences, such as poor cosmesis and delayed chemotherapy and radiation therapy [3]. The recently reported SSI rates fluctuate between 0.95% and 25.8%, far beyond the expected rate of 1%–2% for clean surgical procedures [3,5–9].
In consideration of the significant burden of infection and the unexpectedly higher recent rate, a single dose of pre-operative prophylactic intravenous antibiotic with anti-staphylococcal activity has been standard care for many years [10]. However, the impact of antibiotic prophylaxis is different in various studies [11]. Some studies, not only on breast cancer surgery [12] but for cholecystectomy, inguinal hernia, and external dacryocystorhinostomy, have reported that prophylactic antibiotic cannot reduce the SSI rate [11,13,14], whereas other studies, including several meta-analyses, have found that antibiotics can lower the rate, especially when the SSI rate is high [3,15–20]. Another contradiction to antibiotic application is the potential jeopardization by abuse and misuse of antibiotics, including the cost and the risk of generating bacterial resistance [11]. Therefore, it is important to identify the risk factors for SSI and to take targeted measures to prevent infections. Either procedure-related or patient-related risk factors have been reported to affect the potential for SSI, with patient-related factors, including older age, hypertension [21], high Body Mass Index (BMI) [22], history of diabetes mellitus, smoking, active skin disorders, advanced tumor stage, neoadjuvant chemotherapy, and metastatic deposits in axillary nodes [8,23]), being predominant.
To evaluate the efficacy of antibiotic prophylaxis in reducing the SSI rate after breast surgery, our department discontinued antibiotics in almost all breast cancer operations since 2010 and designed an ambispective cohort study to investigate the necessity of antibiotic prophylaxis and patient-related risk factors for SSI in female breast cancer patients.
Methods
Study design and study population
This study was an ambispective cohort study based on a dynamic patient population in the Department of Breast Surgery, Qilu Hospital of Shandong University, P.R. China. With the approval of the Institutional Review Board, we conducted the prospective study from November 2010 to November 2013. It included all female breast cancer patients who underwent breast cancer operations in the Department. Meanwhile, we reviewed the medical records from patients who were found to have breast cancer between January 2008 and October 2010. Those who underwent clean-incision surgical procedures for pathologically confirmed breast cancer were included. Male patients were excluded. All patients identified between January 2008 and October 2010 (prophylactic group) received antibiotic prophylaxis peri-operatively. None of the patients identified between November 2010 and November 2013 (non-prophylactic group) was given antibiotics.
Data collection
The demographic information, related laboratory values, and peri-operative risk factors, including co-morbidities, the American Society of Anesthesiologists (ASA) Risk Score, neoadjuvant chemotherapy, and type and duration of the operation were collected. Detailed information regarding the use of prophylactic antibiotics, including timing, type, and duration, was retrieved from medical charts.
Outcomes
The SSI events were defined according to the reported standardized criteria established by the U.S. Centers for Disease Control and Prevention [21]. In brief, to qualify as an SSI, infections should occur within 30 days after surgery with at least one of the following: (1) Organisms isolated from the aseptically obtained cultures of tissue or fluid; (2) purulent drainage from the incision; (3) presence of at least one of the classical signs or symptoms of infection, namely, erythema, pain or tenderness, heat, or localized swelling; and (4) diagnosis of SSI by the surgeon or attending physician. Time to SSI was counted from the operation day until the initial sign or symptom of infection was discovered.
Infection surveillance methods
In-patient and out-patient procedures were utilized for SSI monitoring. These surveillance methods included: (1) Review of medical records and laboratory results; (2) direct examination of the surgical incision during the follow-up visits to surgery clinics; and (3) post-charge telephone follow-up by the surgeon.
Statistical analysis
Statistical analyses were performed using SPSS software version 17.0 (SPSS Inc., Chicago, IL, USA). The Fisher exact test and t-test were used for comparison of variables as appropriate. Those with p < 0.10 by univariable analysis were entered into a stepwise logistic regression model. Values of p < 0.05 were considered statistically significant.
Results
Demographics and clinical characteristics of the study population
A total of 2,056 patients who underwent clean-incision breast cancer surgery were included in this study, with exclusion of 12 male patients. According to their medical history, 40 patients had had previous surgery for a malignant breast tumor, 136 had had previous surgery for benign breast tumor, 22 had had previous benign breast disease, 215 received neoadjuvant chemotherapy, and 69 had bilateral cancer and received simultaneously bilateral surgery. Twenty-three patients had an SSI detected, so the overall rate of infection was 1.1%.
Among the eligible patients, 1,034 received peri-operative antibiotic prophylaxis and the other 1,022 did not (Fig. 1). The prophylaxis and non-prophylaxis groups were similar except that fewer patients in the non-prophylaxis group received neoadjuvant chemotherapy. Detailed characteristics of the subjects are shown in Table 1.

Flow diagram of study design.
General Characteristics of Non-Prophylaxis and Prophylaxis Groups
Comparison of SSI rates in prophylaxis and non-prophylaxis groups
All SSIs were found during the original admission and were diagnosed within 14 days after the surgery, with most (87%) identified within the first post-operative week. No significant differences were found regarding the time to SSI between the two groups. The incidence of SSI was 1.2% (12/1,034) in the prophylaxis group and 1.1% (11/1,022) in non-prophylaxis group (p = 0.86). All SSIs were superficial, and all patients received intravenous antibiotic treatment immediately.
Peri-operative variables associated with SSI in non-prophylaxis group
Subgroup analysis was conducted to investigate the possible SSI-related risk factors, and the results are shown in Table 2. Only neoadjuvant chemotherapy (p = 0.026) was found to be related to SSI. Other risk factors such as older age (p = 0.155), hypertension (p = 0.244), smoking history (p = 0.798), co-morbidity of diabetes mellitus (p = 0.559), overweight or obesity, malnutrition (p = 0.739), high ASA score (p = 0.426), longer duration of surgery (p = 0.526), and radical mastectomy and bilateral surgery procedures (p = 0.451) were inclined to exhibit a higher risk of SSI, but the association did not reach statistical significant (Fig. 2).
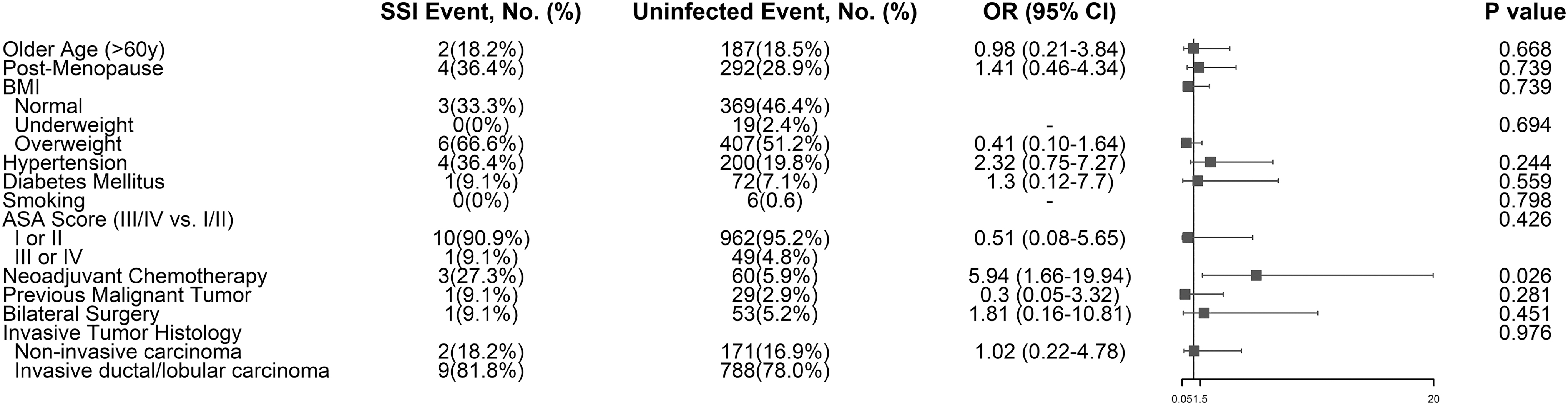
Odds ratios for risk of developing surgical site infections requiring antibiotic treatment determined by univariable analyses.
Comparison of Variables in Patients with Surgical Site Infection and Uninfected Patients in Non-Prophylaxis Group
According to the univariable analysis of risk factors potentially associated with SSI, neoadjuvant chemotherapy was the only significant factor. In consideration of the potential clinical confounding factors, a history of breast disease was included in the logistic regression analysis. However, it turned out that only neoadjuvant chemotherapy (odds ratio [OR] = 5.9; 95% confidence interval [CI] 1.5–23.0; p = 0.01) was an independent factor that predisposed to SSI. Compared with the SSI rate of patients receiving neoadjuvant chemotherapy in the non-prophylaxis group (4.8%; 3/63), the SSI rate was significantly lower in patients receiving neoadjuvant chemotherapy in the prophylaxis group (0.7%; 1/152; p = 0.043) and also in patients not having neoadjuvant chemotherapy in the non-prophylaxis group (0.8%; 8/959; p = 0.027).
Current microbiologic spectrum of SSI in breast cancer patients in our institute
The microbiologic data with susceptibility testing of the eight infected patients who did not receive antibiotic prophylaxis were retrieved. All the infections were monomicrobial. Of these, Staphylococcus aureus-associated infections accounted for five episodes (62.8%), followed by two episodes of Escherichia coli (25%) and one episode (12.5%) of Acinetobacter lwoffii. Obviously, the most prevalent SSI-related bacteria were gram-positive (62.8%), of which S. aureus was predominant. We also found that all S. aureus were ceftriaxone sensitive.
Patterns of antibiotic use
We also investigated the antibiotic administration pattern before 2011. The antibiotic choice was at the discretion of the surgeon, as there was no institutional standard. The course of antibiotics ranged from 1 to 10 days, with the average duration being 2.1 ± 0.8 days. A total of 835 patients received a single dose within 120 min before the incision and a post-operative antibiotic duration of the first 24 hours, with 232 patients receiving an additional 24 hours of antibiotics. Cephalosporin 3 g/dose was administered in most cases (86%). Broad-spectrum penicillin 4 g/dose (0.8%), fluoroquinolones 500 mg/dose (2.0%), lincomycin 1.2 g/dose (2.2%), and aminoglycoside 300 mg/dose (0.3%) were used as alternatives. Combined medication was applied in 89 cases, mainly a broad-spectrum penicillin/cephalosporin and a β-lactamase inhibitor. The SSI rate was reported as 1.3% (9/674) after the administration of a first-generation cephalosporin, 0.5% (1/187) after a fourth-generation cephalosporin, and 5% (1/20) after a fluoroquinolone. Because of the uneven sample size for the different types of antibiotics, the statistical power of these results needs further investigation.
Discussion
Surgical site infection is the most common healthcare-associated infection, especially in patients suffering from cancer. Although the underlying causes have not been studied as thoroughly as in hematologic malignancies [24], some investigations have shown that circulating amounts and activities of regulatory immune cells are mildly below the normal adult range during surgery and anesthesia, which is a manifestation of subtle immune suppression [23] and vulnerability to infection. The reported incidence of SSI for breast cancer surgery ranged from 0.95% to 25.8% [6,7,19,25,26], greatly above the expected 1%–2% for clean surgical procedures. Several clinical guidelines and Cochrane reviews suggest that antibiotic prophylaxis should be used or at least considered in breast cancer surgery, although there is a lack of agreement about the necessity for antibiotic prophylaxis in these patients.
In this ambispective single-institution study, we demonstrated that SSI after clean-wound breast cancer surgery was infrequent (1.1%) as expected. The SSI rate did not decrease in proportion to the administration of peri-operative antibiotic prophylaxis. The result corroborated the non-inferiority of not using peri-operative antibiotic prophylaxis to prevent SSI in female breast cancer patients undergoing clean-incision surgery.
Buggy et al. [27] categorized factors affecting surgical wound healing into three aspects: surgical considerations, anesthetic considerations, and patient-related factors. The reported SSI rates are high in patients undergoing complex surgical procedures, such as reconstructive breast implantation, as high as 35.4% [28–30]. In contrast, the SSI rate we saw was 1.1% and 1.2% in the prophylactic and non-prophylactic groups, respectively. This may be related to the fact that the majority of the operations we performed were modified radical mastectomies.
The putative predominant risk factor for SSI is patient related. Plenty of factors, including greater age, hypertension, high BMI, a history of diabetes mellitus, smoking, active skin disorders, advanced tumor stage, neoadjuvant chemotherapy, and metastatic deposits in axillary nodes have been reported as risk factors for SSI. However, because of the small number of SSI cases, we identified only adjuvant chemotherapy as a significant risk factor. In this subgroup, the incidence of SSI was reduced significantly in patients receiving antibiotic prophylaxis.
Currently, only one related article based on a Chinese population has been published [31]. The overall SSI rate was 9.1% (5/55), and the occurrence of SSI in patients with or without neoadjuvant chemotherapy was 21.1% (4/19) and 3.2% (1/31), respectively. None of the patients was given antibiotic prophylaxis. Our results also indicated that neoadjuvant chemotherapy was an independent risk factor for SSI. Furthermore, the SSI rate of patients receiving neoadjuvant chemotherapy in the non-prophylaxis group was significantly higher than in those receiving neoadjuvant chemotherapy in the prophylaxis group. We could draw a conclusion that the incidence of SSI was reduced significantly with targeted application of antibiotic prophylaxis in patients receiving neoadjuvant chemotherapy. Penel et al. [7] reached similar conclusions, namely that antibiotic prophylaxis is beneficial for patients with a history of chemotherapy. Angarita et al. [8] also concluded that SSI was significantly associated with neoadjuvant chemotherapy (p = 0.003). However, a contrary meta-analysis by Xue et al. [21] indicated that pre-operative chemotherapy was a negligible risk factor for SSI after breast cancer surgery. Therefore, the role of neoadjuvant chemotherapy as a risk factor for SSI in breast cancer patients should be investigated with large-scale randomized, controlled clinical trials.
It has been reported that the SSI rate is associated with the habits of admission and discharge [32]. In our department, patients always are discharged from the hospital one day after the stitches are taken out, during which period, their drainage tubes get removed one day after the daily drainage volume decreases to <15 mL The ward is sterilized every 24 hours. The visiting time is limited, and the patients' activity area is restricted in order to reduce the risk of cross infection. The longer duration of hospital stay not only provides more professional, timely, and routine care to the incisions but also helps detect early signs of infections to obtain better recovery and cosmetic outcomes. Gulluoglu et al. [33], who conducted a randomized controlled trial that included 369 breast cancer patients, reported a total of 34 SSIs, among which 33 were discovered after discharge. Although it is not reasonable to extend the duration of hospitalization indiscriminately, it is worthwhile to discover the high-risk group and protect them from SSI by extending the hospital stays appropriately. In a nutshell, there are many other factors associated with discrepant SSI rates, including inconsistent definitions of SSI, disparities associated with patient and operation characteristics, variance in the rate of identification and surveillance, and whether preventive measures were taken [34].
Another concern about antibiotic usage is the development of resistance. Therefore, we collected data on the bacterial spectrum from the infected patients and examined whether the targeted microorganism of broad-spectrum antibiotics applied nowadays corresponded to the microbiologic spectrum to guide antibiotic usage in surgery. The majority of the SSI-related bacteria were gram-positive (62.5%), with S. aureus predominating. In accordance, a first-generation cephalosporin was used for surgical prophylaxis in most cases. We also compared our results with a retrospective review from the University of Texas M.D. Anderson Cancer Center [35]. From the perspective of breast surgery, the predominant bacteria and most widely used antibiotics were similar in our studies [35]. At M.D. Anderson Cancer Center, 22% of the staphylococcal isolates were methicillin resistant (MRSA), and the predominant gram-negative pathogen was Pseudomonas aeruginosa. In a level of infections of various sites, 40% of monomicrobial infections (MRSA; P. aeruginosa) were resistant to cephalosporin, indicating that the antibiotic prophylaxis selected several decades ago calls for changes.
There are some limitations to our study. First and foremost, it is not a randomized clinical trial but a before-and-after study. Therefore, threats to internal validity cannot be ignored. Second, as a single-institution study, the validity and reliability of our results need further verification and analysis. In our study, the SSI rate is low, and consequently, it takes a much larger sample to obtain a significant difference. Therefore, our conclusions may be more suitable for generalization to hospitals with low SSI rates [36]. Third, information about patients undergoing clean-contaminated versus contaminated-incision operations are not included or analyzed. Besides, we did not take hospital stay and hospital cost into account. Seeking a feasible balance between good care and a prolonged hospital stay is of great value. Although SSIs are among the most common and costly of all complications after surgery, they also are among the most preventable. Even for the not-amenable host factors, they can remind surgeons of the desirability of cautious performance. Although not being a strictly designed randomized controlled trial, our study had high credibility, and our results suggested that peri-operative antibiotic prophylaxis was of no significant value in preventing SSI in clean-incision breast cancer surgery regardless of most reported risk factors.
Footnotes
Acknowledgments
We thank Dr. Smith at DICAT Biomedical Computation Centre for proofreading the manuscript. No funding was received for this study. All authors agree with the content of the manuscript and declare no conflicts of interest.
All procedures were in accordance with the standards of the Ethics Committee of Scientific Research of Shandong University and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all participants included in the study.
Contributions of authors: Study conception and design: Y. Zhang; data acquisition, analysis, and interpretation: H. Zhang, Y. Wang, S. Yang; Quality control of data and algorithms, statistical analysis, manuscript review, and manuscript editing: H. Zhang, Y. Wang; manuscript preparation: H. Zhang.
Author Disclosure Statement
No competing financial interests exist.